Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
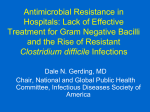
ClinicalArticle Clostridium difficile– Associated Disease Diagnosis, Prevention, Treatment, and Nursing Care Maria E. Pelleschi, RN, MS, CCRN This article has been designated for CE credit. A closed-book, multiple-choice examination follows this article, which tests your knowledge of the following objectives: 1. Discuss the incidence of Clostridium difficile–associated disease (CDAD) in the critical care setting 2. Identify key preventive measures for decreasing CDAD 3. Describe nursing care of patients with CDAD in the critical care setting I magine that your beloved grandmother has been hospitalized with a stroke. You are devastated as you imagine the lifestyle changes that will shortly ensue. You contemplate rehabilitation, physical therapy, and extended care possibilities. Her progress is good, except for a small bout of pneumonia that is successfully treated with a course of oral antibiotics. Therapy resumes, as do discussions about moving forward. Then she begins to complain of abdominal pain, has a mild fever, and experiences multiple liquid, Author Maria E. Pelleschi has more than 20 years of experience as a critical care nurse. Recently a staff nurse in the cardiovascular surgical intensive care unit at St Vincent Charity Hospital in Cleveland, Ohio, she is now a nursing instructor at Bryant and Stratton College in Parma, Ohio. Corresponding author: Maria E. Pelleschi, RN, MS, CCRN, Bryant & Stratton College, 12955 Snow Rd., Parma, OH 44130 (e-mail: [email protected] or [email protected]). To purchase electronic or print reprints, contact The InnoVision Group, 101 Columbia, Aliso Viejo, CA 92656. Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; e-mail, [email protected]. http://ccn.aacnjournals.org foul-smelling stools. She has been placed in isolation, and you don gloves and gown and lean over to listen as she whispers “I have something called C-diff.” Clostridium difficile–associated disease (CDAD) is a confounding complication. Experienced by patients in extended care facilities, acute care areas, and intensive care units, it has become increasingly prevalent in the United States since 2003, when 178000 cases were diagnosed.1 The rate of CDAD is 7 times higher in persons more than 65 years old than in persons from 45 to 64 years old.1 Possible explanations for these different rates include greater exposure to hospitals and extended care facilities, greater use of antimicrobial drugs, and decreased host defenses among older persons.2 CDAD has become so rampant that reporting infection with C difficile has become mandatory in Ohio.3 Conservative estimates suggest that patients with CDAD incur at least $3669 extra in hospital costs and spend at least 3.6 CRITICALCARENURSE Vol 28, No. 1, FEBRUARY 2008 27 additional days in the hospital.4 Costs may exceed $600 million per year in short-term care facilities alone.1 Nurses must care for patients with CDAD and are therefore in position to prevent its spread. In this article, I provide an overview of this disease, its mode of transmission, diagnosis, prevention, and current methods of treatment. I also discuss the nursing care of patients who have CDAD. Susceptible host (one or more risk factors) Loss of protective normal flora (antibiotic exposure and/or decreased stomach acidity) Exposure to C difficile spores (bedside items, caregiver’s hands) Ingestion of spores (transmission via fecal-oral route) Definition and Description CDAD is used to describe a constellation of illnesses caused by the toxins, A and B, produced by the C difficile bacillus. The illnesses include diarrhea, pseudomembranous colitis, toxic megacolon, perforation of the colon, and, in some instances, sepsis.5 The emergence of a new, more virulent strain of C difficile partly explains the recent increase in CDAD. This new strain, the North American pulsed-field gel electrophoresis type I (NAP I) is more virulent and can produce greater quantities of toxin A (16 times more) and toxin B (23 times more) than other strains.2,5 Binary toxin, a third toxin, is also produced by NAP I, although its significance is unknown.5 Researchers6 in Quebec identified use of fluoroquinolones as the most important risk factor in the development of this new strain of C difficile. Other factors associated with diarrhea, such as predominant use of highrisk antibiotics, reduction in housekeeping staff, increased nursing workloads, antiquated facilities, and general changes in hospital populations (ie, increased number of immunocompromised, debilitated, and elderly patients) may also be contributing factors.7 Proliferation of C difficile bacteria causes secretion ofa Toxin A (exotoxin) Activation of macrophages and mast cells Fluid secretion and increased mucosal permeability because of increased inflammation Toxin B (cytotoxin) Increased leukocytes Increased cytokines Profound colonic inflammatory response Possible necrosis of borders of colon with sloughing of cells Massive fluid secretion into lumen of the colon Diarrhea results Focal ulceration (possibly) Accumulation of purulent and necrotic debris Formation of pseudomembranes Figure Development of Clostridium difficile–associated diarrhea2,5,9-12 a NAP I strain also produces binary toxin, which is associated with more severe signs and symptoms and with increased production of toxins A and B. Etiology and Transmission of C difficile Infection Clostridium difficile is an anaerobic, spore-forming, gram-positive bacillus.8 The spores are resistant to many types of disinfectants, heat, and dryness and may persist for months on surfaces such as bed rails, commodes, electronic thermometers, stethoscopes, skin folds, and the hands of caregivers.2 The 28 CRITICALCARENURSE Vol 28, No. 1, FEBRUARY 2008 spores can cause disease in persons at high risk for CDAD. Transmission of C difficile is via the fecal-oral route (see Figure). In healthy persons, growth of C difficile is kept in check by normal flora in the gut. Possibly, use of antibiotics and medications that decrease stomach acidity, such as proton pump inhibitors, cause C difficile bacteria to proliferate.9 http://ccn.aacnjournals.org often mucoid and foul smelling. Some have described it as having a characteristic “barnyard” odor.13 Associated signs and symptoms include nausea, dehydration, and low-grade fever. Leukocytosis may occur.5,10 Colitis occurs with severe forms of the disease and causes profuse diarrhea and abdominal pain, often with fever, nausea, abdominal distension, and dehydration. Characteristic raised white and yellow Table 1 Risk factors for Clostridium difficile–associated disease6,9 Exposure to antimicrobial agents such as clindaymycin, cephalosporins, quinolones, and penicillin Gastrointestinal surgery Advanced age Presence of a feeding tube Chemotherapy agents Environmental exposure Severe underlying illness Decreased stomach acidity (H2-blockers or proton pump inhibitors) Pathophysiology Once in the colon, C difficile, its growth unchecked by normal flora or stomach acid, produces 2 toxins: an enterotoxin (toxin A) and a more potent cytotoxin (toxin B).10,11 Toxin A activates macrophages and mast cells,11 which release inflammatory mediators. The mediators cause disruption of the cell wall junction, resulting in increased permeability of the intestinal wall and subsequent diarrhea.5,11 Meanwhile, toxin B causes degradation of epithelial cells in the colon.5 As the colitis worsens, purulent and necrotic debris accumulates and forms characteristic ulcers, the pseudomembranes11 (see Figure). cramping in the lower part of the abdomen without systemic signs and symptoms.5 The diarrhea is Table 2 Clinical manifestations and treatment of various severities of Clostridium difficile–associated disease Clinical manifestations5,13 Mild to moderate nonbloody diarrhea Cramping in lower part of abdomen Vomiting Dehydration Fever Mild abdominal tenderness Leukocytosis Treatments and interventions14-21 Cessation of suspected causative agent Administration of metronidazole, orally or intravenously Administration of vancomycin, orally or via nasogastric tube Contact isolation Monitoring for dehydration Fluid replacement as indicated Frequent skin assessment Use of moisture barriers and fecal containment devices Frequent mouth care Severe Colitis Profuse, watery diarrhea Abdominal pain Fever Nausea Abdominal distention Dehydration Pseudomembrane All of the above Use of tolevamer when available commercially Administration of corticosteroids Systemic Fulminant pseudomembranous colitis Systemic complications including sepsis, volume depletion, electrolyte imbalance, hypotension Peritonitis, paralytic ileus, and toxic megacolon (decrease in stool) Hypoalbuminemia and ascites Colonic wall thickening, lumen obliteration, pericolonic fat stranding present on computed tomography scans All of the above Hemodynamic monitoring Blood pressure support Volume replacement Respiratory support Administration of vancomycin enema Immunoglobulin therapy Surgery for megacolon Severity Mild Risk Factors A number of risk factors for CDAD, including the use of antimicrobials, particularly fluoroquinolones, have been identified6 (Table 1). Patients who are elderly, have severe underlying disease, have nasogastric tubes in place, have long hospital stays, or are taking proton pump inhibitors and histamine receptor antagonists are at particular risk.9 Clinical Manifestations CDAD can be mild, severe, or systemic (Table 2). Mild disease is characterized by nonbloody diarrhea, occasionally accompanied by http://ccn.aacnjournals.org CRITICALCARENURSE Vol 28, No. 1, FEBRUARY 2008 29 plaques may be visualized during sigmoidoscopy.5,10 Composed of neutrophils, fibrin, mucin, and cellular debris, these pseudomembranes appear on inflamed colonic mucosa as raised nodules, usually 2 to 10 mm in diameter.22 Complications such as sepsis, volume depletion, electrolyte imbalance, hypotension, peritonitis, paralytic ileus, and toxic megacolon may be present in systemic CDAD.5 Hypoalbuminemia and ascites may also be evident.23 A decrease in diarrhea may occur in systemic disease as a result of toxic megacolon or paralytic ileus.5,10 Computed tomography scans may show thickening of the colon wall or obliteration of the lumen.23 Patients with systemic disease associated with megacolon may require surgery.5,10 Diagnosis Diagnosis of CDAD is based on signs and symptoms, verification of the presence of toxins A and B in stool cultures, and, in many instances, detection of pseudomembranous colitis. Pseudomembranous colitis is verified via colonoscopy. Because of the risk of perforation and the cost of this test (mean, $1656 per test),24 experts suggest that colonoscopy be used with caution, and only for patients with severe colitis of unclear origin.10,23 Stool cultures are highly specific and sensitive for detection of toxin B; however, they are time intensive and are not often used.22,23 The enzyme-linked immunosorbent assay test for toxin A or toxins A and B has excellent specificity, and results are usually available in about 2 hours.22,23 The sensitivity, however, is only 75% to 85%. Therefore, cultures of serial stool samples collected on different days are suggested, especially in suspicious cases in which the initial samples are negative for C difficile.23 The large quantity of stool produced in CDAD allows ample opportunity for specimen collection. Of note, the toxins themselves are unstable at room temperature; therefore, false-negative results may occur in samples that are not tested within 2 hours of collection.25 For that reason, ensuring that stool samples are quickly sent for testing once obtained is prudent. Because the stools themselves harbor C difficile spores, great care must be taken to avoid contaminating surfaces with the specimens. Pimetel23 suggests that specimens be sent and tested before antibiotic therapy is started and that contact isolation be initiated on the basis of signs and symptoms, rather than waiting for culture results. Sunenshine and McDonald5 suggest that only watery or liquid stools be tested. A falsepositive result could indicate that C difficile colonization is present. Infection is not likely in persons who do not have diarrhea.5 Preventing CDAD Patients treated with antibiotics must be closely monitored for possible infection with C difficile. Patients who are elderly, have severe underlying illness, are immunocompromised, or have undergone surgery of the gastrointestinal tract also require heightened vigilance. Prevention of CDAD, however, entails multidisciplinary efforts to stem the disease for all patients. Three elements are required for prevention of CDAD: proper hand 30 CRITICALCARENURSE Vol 28, No. 1, FEBRUARY 2008 washing, contact isolation, and environmental measures. Hand Hygiene Hands must be washed with an antimicrobial soap for at least 15 seconds. Although generally beneficial, alcohol-based hand rubs may not be effective against C difficile spores.2 A paper towel should be used to turn off the faucet. Hands should be washed before and after contact with a patient and after glove removal. This technique must be taught to all of the patient’s family members as well as the patient. Reminders to healthcare workers are also important. In one study,26 effective staff education programs resulted in a significant reduction in infection rates. Recommendations include clustering of nursing care, hand hygiene education, and ongoing audit and surveillance programs.26 Contact Isolation Guidelines of the Centers for Disease Control and Prevention mandate contact isolation for all patients with CDAD. Private rooms are recommended if available; however, if necessary, 2 patients with CDAD can be placed together. All persons entering the patient’s room, including the patient’s family members, must use protective gowns and gloves. Use of dedicated equipment such as thermometers and stethoscopes is also recommended.2 Such imposed isolation requires compassionate yet firm teaching and support for patients and their family members. All hospital employees, including physicians, therapists, clergy, and technicians, must abide by isolation guidelines, no matter how brief their visit. http://ccn.aacnjournals.org Environmental Measures Spores of C difficile tend to thrive on hospital surfaces. For that reason, stringent daily cleaning of all hospital surfaces likely to be contaminated with feces is essential. A hypochlorite-based disinfectant that has been registered with the Environmental Protection Agency or a 1:10 bleach solution is recommended.2 Frequently touched surfaces such as doorknobs, light switches, call lights, television remote control devices, soap dispensers, faucets, bed rails, and telephones also require thorough daily cleaning. Hospital policies regarding dedicated equipment, dishes, linens, waste, and patient transport should be in place and enforced. Nondisposable equipment such as glucose meters, cardiac monitors and electrocardiography and x-ray machines should be disinfected according to manufacturers’ guidelines. Nurse managers at a hospital in England attribute a significant decrease in C difficile infection to changes in environmental policies and replacement of outdated commodes and mattresses. A decrease in length of stay and cost savings were also realized as a result of these changes.27 Treatment The various treatments suggested for CDAD and their efficacy are matters of much debate. A review of basic and more recent innovative treatments follows (Table 3). As Bartlett14(p429) notes “It can be safely concluded that all of these treatments work some of the time, none work all of the time.” This comment reflects the confounding nature of CDAD and the necessity of impeccable nursing practices. http://ccn.aacnjournals.org Table 3 Treatment options for Clostridium difficile–associated disease (CDAD)14-20,28 Treatment Metronidazole Dosing Comments 500 mg by mouth 3 Oral route preferred times a day or 500 Less expensive than vancomycin mg intravenously every 6 hours Vancomycin 125 mg by mouth 4 times a day Nitazoxanide 500 mg by mouth twice a day Tolevamer 3-6 g/d by mouth Oral route preferred, may also be given via enema or nasogastric tube Intravenous route not effective for CDAD May lead to vancomycin resistance Blocks anaerobic metabolism Inhibits growth of C difficile in vitro Nonantibiotic polymer Not yet available commercially For mild to moderate CDAD May cause hypokalemia Immunoglobulin 300-500 mg/kg 1-6 doses given Proposed for intractable and severe CDAD Probiotics Given orally Variable dosing Further studies recommended before generalization into practice Donor stool 25 mL given via nasogastric tube Meant to replace normal bowel flora Specific donor criteria Further studies suggested Antibiotics The first treatment for CDAD is cessation of the suspected causative antibiotic.23 Although stopping the antibiotic may be effective, the reason the antibiotic was prescribed in the first place should be considered, and monitoring for recurrence or worsening of the underlying infection is essential. Oral metronidazole, 250 to 500 mg 4 times a day for 7 to 14 days, is generally recommended as an initial treatment.29 Metronidazole can also be given intravenously.30 Administered by either route, the same dosage provides bactericidal levels of the drug in the bowel lumen. Although equally effective as metronidazole when given orally,30 vancomycin, standard dosage 1 g/d for 10 days, is more expensive, and is therefore reserved for patients who can not tolerate metronidazole, are pregnant or breastfeeding, or have severe cases of CDAD.23,29,30 Alternative vancomycin dosing strategies may be effective for treatment of recurrent CDAD.31 A pulsed dosing regimen, intermittent delivery of between 125 and 500 mg every 3 days, and tapered dosing, administering the antibiotic over long periods at decreasing doses, may in some instances effectively eradicate vegetative C difficile cells.31 In addition to its greater cost, a disadvantage of vancomycin is the occurrence of vancomycin-resistant strains.23 Intraluminal concentrations of vancomycin cannot be achieved by intravenous infusion as they can with metronidazole.30 However, vancomycin can be given via a nasogastric tube or as an enema.30 Instilling vancomycin as an enema can be challenging, particularly when a patient is experiencing diarrhea. This route is suggested as an adjunct for patients with persistent CRITICALCARENURSE Vol 28, No. 1, FEBRUARY 2008 31 or severe CDAD, severe ileus, or fulminant colitis.15 The medication can be given at dosing intervals of 4 to 12 hours, with doses of 2 to 3 g/d, by using an 18F Foley catheter or a soft 6F pigtail catheter. The risk of bowel perforation, inherent any time an enema is given, mandates particular vigilance for these patients. Ideally, the enema should be retained for 60 minutes. Vancomycin can also be given via colostomy, ileostomy, or during colonoscopy.15 Oral rifampin has been given with metronidazole as an adjunct therapy. A prospective, randomized, single-blind study16 of 39 patients was conducted to compare the efficacy of metronidazole therapy alone with that of metronidazole plus rifampin. The researchers could not demonstrate a therapeutic benefit of this drug combination and halted their study early, citing study futility and urging better treatment protocols.16 More promising results are suggested by a study17 in which oral metronidazole was compared with nitazoxanide. A nitrothiazolide, nitazoxanide works by blocking anaerobic metabolism and is used to treat intestinal infections caused by the protozoa Cryptosporidium and Giardia. Patients receiving nitazoxanide were given 500 mg every 12 hours for 7 or 10 days. Those receiving metronidazole received 250 mg every 6 hours for 10 days. For both groups, the time of resolution of their signs and symptoms, clinical response after 7 days of treatment, and sustained response after 31 days were determined. Initial data suggest similar effectiveness for metronidazole and nitazoxanide. Further studies are being designed to compare this new medication with vancomycin.17 Nonantibiotic Polymer Not yet available commercially, tolevamer can also be considered for treating CDAD. A soluble, highmolecular-weight, anionic polymer, tolevamer works by binding C difficile toxins A and B.18 Suggested for use with mild to moderately severe CDAD, tolevamer is given orally 3 times daily for a total of 3 to 6 g per day. Initial trial results indicted that the polymer was fairly well tolerated, provided resolution of signs and symptoms in 67% of patients, and was associated with a lower incidence of recurrence than was vancomycin.18 Resolution of diarrhea was comparable to that achieved with vancomycin; however, tolevamer is also associated with an increased risk of hypokalemia.18 Immunoglobulin Immunoglobulin has been proposed as a treatment for intractable and severe cases of CDAD. In one study,19 patients were given 1 to 6 doses, ranging between 300 and 500 mg/kg. Of 5 patients with refractory disease, 3 had resolution of signs and symptoms within 11 days. Although this treatment looks promising, immunoglobulin is expensive and in short supply.19 Probiotics Probiotics are live organisms meant to treat particular diseases, including Helicobacter pylori infections, acute gastroenteritis, and antibiotic-associated diarrhea, including CDAD. The most commonly used probiotic agents produce lactic acid and are present in 32 CRITICALCARENURSE Vol 28, No. 1, FEBRUARY 2008 normal microflora. Examples include Saccharomyces boulardii, Lactobacillus acidophilus, and Lactobacillus plantarum.32 Many studies of probiotics have been done. Sullivan and Nord32 suggest that although S boulardii was somewhat effective, particularly in preventing recurrent CDAD, further studies are needed. Dendukuri et al20 similarly determined that evidence was insufficient to recommend the routine clinical use of probiotics to treat CDAD in adults. Corticosteroids Use of corticosteroids in a child with refractory CDAD has been described.33 Typically used for acute flare-ups of inflammatory bowel disease, corticosteroids may also be beneficial in CDAD. Further studies are needed. Donor Stool Transplants A potential means of replacing normal bowel flora is transplanted stool. In one study,28 18 patients were each given 25 mL of donor stool via a nasogastric tube. Stool transplant donors were persons who had not received antimicrobial therapy for 6 months, had intimate contact with the patient (ie, spouse or significant other, family household members), or were otherwise healthy donors. Two patients in the study died of unrelated illness; however, the remaining patients experienced a 94% cure rate, that is, reported return of normal bowel function. Further studies are suggested before donor stool transplants are used routinely.28 Although aesthetic, logistical, and ethical issues may need to be considered, Aas et al28 contend that the http://ccn.aacnjournals.org patients in the study were receptive to the prospect of stool transplant. stools have tremendous needs with respect to skin integrity and comfort. Surgery CDAD that progresses to paralytic ileus, toxic megacolon, or sepsis despite appropriate treatment may require surgical intervention.21 Fulminant pseudomembranous colitis is typically associated with high mortality related to hypotension, acute renal failure, and respiratory failure. Researchers21 in Canada concluded that total abdominal colectomy performed within 72 hours of diagnosis of fulminant pseudomembranous colitis improves survival rates. They21 therefore support early surgical interventions. Prevent Dehydration Prevention of dehydration is essential for patients with CDAD. Patients’ weights, fluid intake and output, and levels of electrolytes, albumin, and protein must be monitored and corrected as needed. Intake of protein, iron, and vitamin C should be encouraged as tolerated.34 Patients should be monitored for clinical manifestations of dehydration, including rapid, thready pulse; decreased blood pressure; diminished peripheral pulses; flat neck veins; increased rate and depth of respiration; fever; decreased level of consciousness; and decreased urine output with increased specific gravity. Patients should also be assessed for the presence of dry flaky skin with poor turgor, thirst, and mouth fissures.34,35 Fluid balance should be restored through intravenous therapy based on frequent assessment of vital signs, urine output, and hemodynamic parameters. When possible, oral rehydration should be encouraged. Mouth care should be provided frequently, and patients should be instructed to avoid the use of lemon-glycerin swabs and commercial mouthwashes.34,35 Fever, nausea, and dehydration due to fulminant disease could result in hypotension, tachycardia, and hypovolemia.21 Because antiperistaltic agents such as diphenoxylate hydrochloride and atropine sulfate may predispose patients with CDAD to toxic megacolon, these drugs are not recommended.5,11,22 Use of narcotics should also be avoided.5 Nursing Care CDAD is a complication encountered by patients hospitalized for other illnesses. Patients, therefore, must be monitored and treated for their underlying illness. In addition, they must be closely monitored for elevated white blood cell counts, fever, abdominal pain, and, most certainly, diarrhea. The goals of care include prevention of CDAD, early recognition and treatment of the disease, promotion of comfort, and prevention of skin breakdown. Priorities of Care All patients with CDAD require monitoring of vital signs and hemodynamic status. In addition to gastrointestinal assessment, monitoring of renal, respiratory, and neurological status is imperative in order to detect and treat systemic manifestations. Aggressive intervention to treat dehydration and abnormalities revealed by laboratory tests is essential. Patients with copious liquid http://ccn.aacnjournals.org Promote Comfort Numerous liquid bowel movements associated with abdominal tenderness, pain, or cramping are certainly cause for misery. Mandated isolation may lead to emotional distress.36 Compassionate measures can minimize these problems. Therefore, it is imperative to monitor for pain, offer analgesia as indicated, provide frequent skin and mouth care, and assess for depression or sadness. Patients’ satisfaction during isolation can be enhanced by measures that include providing ongoing communication, estimating duration of isolation, maintaining access to telephone and television, and promoting the patient’s sense of control.36 Maintain Skin Integrity Prevention of skin breakdown is enormously challenging because of the frequency, amount, and characteristics of stools in patients with CDAD. Excessive moisture, alkaline pH, colonization with microorganisms, and friction contribute to skin breakdown.37 Goals of perineal skin care include regularly removing skin irritants, minimizing exposure to bacteria, and establishing a healing local environment. Cleansers that contain water and surfactants, are near the normal skin pH of 5.5, and provide moisture should be selected. The perineum should be cleansed daily and with each bowel movement. Creams or ointments that serve as moisture barriers should be applied after cleaning.37 A possible complication of fecal incontinence is perineal dermatitis. A recent study38 indicated the need for staff compliance and consistency in the use of products and measures in the prevention of this complication. CRITICALCARENURSE Vol 28, No. 1, FEBRUARY 2008 33 Table 4 Summary of nursing plan of care34-39 Situation Risk for deficient fluid volume related to Clostridium difficile–associated disease Nursing care Monitor vital signs, fluid status, and hemodynamic parameters closely Encourage adequate oral intake as tolerated Replace fluids and electrolytes as indicated Alteration in comfort related to diarrhea and abdominal pain Monitor for pain Provide analgesia and comfort measures as required Provide frequent mouth and skin care Risk for loneliness related to imposed isolation Assess for depression and sadness Help patient identify and express feelings associated with isolation experience Encourage socialization with family and significant others as able Allow patient to maintain access to telephone and television Risk for perineal skin breakdown related to frequent stools Keep skin clean and dry after bowel movements Provide moisture barriers Protect bony prominences Use commercial fecal containment system when indicated; follow manufacturer’s guidelines closely Turn and reposition patient every 2 hours as tolerated Monitor nutrition status, including albumin and protein levels, and provide adequate intake of calories 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. Use of commercial fecal diversion and containment systems may also be considered. Products such as the Flexi-Seal fecal management system (Convatec, Princeton, New Jersey) contain a silicone catheter with a retention balloon and a collection bag.39 The catheter is inserted into the rectum, and when used properly, can contain and divert liquid or semiliquid stool away from the perineum. Manufacturer guidelines should be followed closely, especially with respect to the length of time this treatment may be continued, recommended balloon pressure,39 and before instilling medications. critical care nurses to provide early and thorough assessment of those most at risk. Impeccable nursing care must be provided to those with CDAD (Table 4). In the 1800s, Florence Nightingale wrote, “It may seem a strange principle to enunciate as the very first requirement in a hospital that it should do the sick no harm.” Prevention is the most important treatment. Financial Disclosures None reported. 13. 14. 15. 16. 17. References Conclusion The possibility that CDAD may develop in our patients challenges 34 CRITICALCARENURSE Vol 28, No. 1, FEBRUARY 2008 1. McDonald LC, Owings M, Jerigan DB. Clostridium difficile infection in patients discharged from US short-stay hospitals, 19962003. Emerg Infect Dis. 2006;12(3):409-415. http://www.cdc.gov/ncidod/EID/vol12no03 /05-1064.htm. Accessed November 26, 2007. 2. Centers for Disease Control and Prevention. Clostridium difficile information for healthcare providers: FAQ: CDC infection control. 2005. http://www.cdc.gov/ncidod/dhqp 18. 19. /id_CdiffFAQ_HCP.html. Accessed November 26, 2007. Ohio Department of Health. Clostridium difficile. 2006. http://www.odh.state.oh.us /pdf/idcm/clostdif.pdf#search= %22incidence%20CDAD%20Ohio %20Department%20of%20health%22. Accessed November 26, 2007. Kyne L, Hamel MB, Polavaram R, et al. Health care costs and mortality associated with nosocomial diarrhea due to Clostridium difficile. Clin Infect Dis. 2002;34(3):346-353. Sunenshine RH, McDonald LC. Clostridium difficile-associated disease: new challenges from an established pathogen. Cleve Clin J Med. 2006;73(2):187-197. Pepin J, Saheb N, Coulombe MA, et al. Emergence of floroquinolones as the predominant risk factor for Clostridium difficile-associated diarrhea: a corhort study during an epidemic in Quebec. Clin Infect Dis. 2005;41(9):1254-1260. Loo VG, Libman MD, Miller MA, et al. Clostridium difficile: a formidable foe. CMAJ. 2006;171(1):47-48. Murray PR, Rosenthal KS, Pfaller AM. Medical Microbiology. 5th ed. Philadelphia, PA: Elsevier Mosby; 2005:411-413. Dial S, Alrasadi K, Manoukian C, Huang A, et al. Risk of Clostridium difficile diarrhea among inpatients prescribed proton pump inhibitors: cohort and case-control studies. CMAJ. 2004;171(1):33-38. Poutanen SM, Simor AE. Clostridium difficile-associated diarrhea in adults. CMAJ. 2004;171(1):51-58. Schroeder MS. Clostridium difficile-associated diarrhea. Am Fam Physician. 2005;71(5):921928. http://www.aafp.org/afp/20050301 /921.pdf. Accessed November 26, 2007. Perloff S, Horn D. Community-acquired Clostridium difficile colitis. Emerg Med. 2007;39(7):37-42. http://www.emedmag .com/html/pre/fea/features/039070037.asp. Accessed November 26, 2007. Grainger M. A staff nurse’s perspective of infection control problems. Br J Nurs. 2005; 14(17):912-916. Bartlett JG. New drugs for Clostridium difficile infection. Clin Infect Dis. 2006;43(4): 428-431. Apisarnthanarak A, Mundy LM. Intracolonic vancomycin for adjunctive treatment of severe Clostridium difficile colitis: indications and precautions. J Infect Dis Antimicrob Agents. 2005;22(1):21-26. Lagrotteria D, Holmes S, Smieja M, Smaill F, Lee C. Prospective, randomized inpatient study of oral metronidazole versus oral metronidazole and rifampin for treatment of primary episodes of Clostridium difficileassociated diarrhea. Clin Infect Dis. 2006; 43(5):547-552. Musher DM, Logan N, Hamill RJ, et al. Nitazoxanide for the treatment of Clostridium difficile colitis. Clin Infect Dis. 2006; 43(4):421-427. Louie TJ, Peppe J, Watt CK, et al. Tolevamer, a novel nonantibiotic polymer, compared with vancomycin in the treatment of mild to moderately severe Clostridium difficileassociated diarrhea. Clin Infect Dis. 2006; 43(4):411-420. Wilcox MH. Descriptive study of intravenous immunoglobulin for the treatment of recurrent Clostridium difficile diarrhoea. J Antimicrob Chemother. 2004;53(5):882-884. http://ccn.aacnjournals.org 20. Dendukuri N, Costa V, McGregor M, et al. Probiotic therapy for the prevention and treatment of Clostridium difficile diarrhea: a systematic review. CMAJ. 2005;173(2): 167-170. 21. Boutros M, Ladouceur M, Rahme E, Lamoureux E, Vasilevsky CA. Timing of total abdominal colectomy and risk factors predictive of mortality for fulminant Clostridium difficile colitis [abstract]. Can J Surg. 2006; 49(suppl):24. 22. Fordtran JS. Colitis due to Clostridium difficile toxins: underdiagnosed, highly virulent, and nosocomial. Proc (Bayl Univ Med Cent). 2006;19(1):3-12. 23. Pimentel RR. Antibiotic-associated diarrhea. The Cleveland Clinic: Medicine Index. 2003. http://www.clevelandclinicmeded.com /diseasemanagement/gastro/antibioticdiarrhea /antibioticdiarrhea.htm. Accessed November 26, 2007. 24. Fisher JA, Fikry C, Troxel AB. Cutting cost and increasing access to colorectal cancer screening: another approach to following the guidelines. Cancer Epidemiol Biomarkers Prev. 2006;15(1):108-113. 25. Todor K. Todor’s Online Book of Bacteriology. 2006. http://textbookofbacteriology.net/clostridia.html. Accessed November 26, 2007. 26. Lam BC, Lee J, Lau YL. Hand hygiene practices in a neonatal intensive care unit: a multimodal intervention and impact on nosocomial infection. Pediatrics. 2004;114(5):e565-e571. 27. Parish C. New commodes and mattresses lead to dramatic fall in infections. Nurs Stand. 2007;21(41):11. 28. Aas J, Gessert CE, Bakken JS. Recurrent Clostridium difficile colitis: case series involving 18 patients treated with donor stool administered via a nasogastric tube. Clin Infect Dis. 2003;36(5):580-585. 29. Ohl ME, Stevermer JJ, Meadows S. What are the effective therapies for Clostridium difficile-associated diarrhea? J Fam Pract. 2005;54(2):176-178. 30. Chico GF, Chico MA. Clostridium difficile colitis. Emerg Med. 2005;37(1): 27-32. http://www.emedmag.com/html/pre/gic/consults/011505.asp. Accessed November 26, 2007. 31. McFarland LV. Alternative treatments for Clostridium difficile disease: what really works? J Med Microbiol. 2005;54(pt 2):101-111. 32. Sullivan A, Nord CE. Probiotics and gastrointestinal disease. J Intern Med. 2005;257(1): 78-92. 33. Cavagnaro C, Berezin S, Medow MS. Corticosteroid treatment of severe, non-responsive Clostridium difficile induced colitis. Arch Dis Child. 2003; 88(4):342-344. 34. Ignatavicius D, Workman M. Medical-Surgical Nursing: Critical Thinking for Collaborative Care. St Louis, MO: Elsevier Saunders; 2006:1429, 217-219. 35. Ackley BJ, Ladwig, GB. Nursing Diagnosis Handbook. 7th ed. St. Louis, MO: Mosby Elsevier; 2006:1125-1131. 36. Rees J, Davies H, Birchall C, Price J. Psychological effects of source isolation nursing, 2: patient satisfaction. Nurs Stand. 2000; 14(29):32-36. 37. George-Gay B, Chernecky CC. Clinical Medical-Surgical Nursing: A Decision-Making Reference. Philadelphia, PA: WB Saunders Co; 2002:519-524. 38. Driver DS. Perineal dermatitis in critical care. Crit Care Nurse. 2007;27(4):42-46. 39. Convatec, A Brystol-Meyer Squibb Company. Healthcare professionals: Flexi-Seal Fecal Management System. 2007. http://www.convatec.com/index.html. Accessed November 26, 2007. http://ccn.aacnjournals.org CRITICALCARENURSE Vol 28, No. 1, FEBRUARY 2008 35 CE Test Test ID C0813: Clostridium dif f icile–Associated Disease: Diagnosis, Prevention, Treatment, and Nursing Care Learning objectives: 1. Discuss the incidence of Clostridium difficile-associated disease (CDAD) in the critical care setting 2. Identify key preventive measures for decreasing CDAD 3. Describe nursing care of patients with CDAD in the critical care setting 1. The incidence of Clostridium difficile–associated disease (CDAD) is higher in which age group? a. 45 to 55 years b. 30 to 65 years c. < 30 years and immune compromised d. > 65 years 2. Which of the following states have mandated reporting of C difficile? a. New Hampshire b. Ohio c. Florida d. Arizona 3. Recent increases in CDAD have been associated with the emergence of which new strain? a. North American virulent mucoid strain b. Northern Canadian pulse field-electrophoresis type I c. North American pulse-field gel electrophoresis type I d. North American pulse-field 4. Which of the following is an identified risk factor for C difficile? a. Retention urinary catheters b. Short hospital stays c. Surgical procedures d. Use of proton pump inhibitors and histamine receptor antagonists 7. Which of the following best describes 3 elements for preventing CDAD? a. Wearing personal protective equipment, spraying sanitizer on surfaces, and proper hand washing b. Using alcohol-based hand sanitizers, reverse isolation, and wearing proper personal protective equipment c. Cooking meat to proper temperature, proper hand washing, and limiting use of histamine receptor antagonist d. Proper hand washing, contact isolation, and environmental measures 8. All persons entering a room with CDAD, no matter the duration of their visit, must wear which of the following? a. Gloves, booties, and mask b. Gloves and mask c. Full isolation suit d. Protective gown and gloves 9. What cleaning solution is recommended for disinfecting surfaced likely to be contaminated with C difficile? a. 1:5 bleach solution b. 1:20 bleach solution c. 1:10 bleach solution d. None of the above 10. Which antibiotic is recommended as the initial treatment for CDAD? a. Metronidazole, 250 to 500 mg 4 times daily for 7 to 14 days b. Fluconazole, 200 to 400 mg daily for 7 days c. Ketoconazole, 200 to 400 mg daily for 7 days d. Loperamide, 2 mg after each loose stool 5. Which of the following is not a systemic complication of CDAD? a. Hyperbilirubinemia b. Sepsis c. Hypovolemia d. Peritonitis 6. False negative results for C difficile may occur if samples are not tested within how many hours of collection? a. 8 hours b. 6 hours c. 2 hours d. 12 hours 11. Which of the following best describes nursing care of patients diagnosed with CDAD? a. Monitoring vital signs b. Monitoring renal status c. Aggressive interventions to prevent dehydration d. All of the above 12. Measures to enhance patient satisfaction for those in mandatory isolation include all except which of the following? a. Limiting visitations from family and friends b. Providing ongoing communica tion c. Estimating duration of isolation d. Maintaining access telephone and television Test answers: Mark only one box for your answer to each question. You may photocopy this form. 1. K a Kb Kc Kd 2. K a Kb Kc Kd 3. K a Kb Kc Kd 4. K a Kb Kc Kd 5. K a Kb Kc Kd 6. K a Kb Kc Kd 7. K a Kb Kc Kd 8. K a Kb Kc Kd 9. K a Kb Kc Kd 11. K a Kb Kc Kd 10. K a Kb Kc Kd 12. K a Kb Kc Kd Test ID: C0813 Form expires: February 1, 2010 Contact hours: 1.0 Fee: AACN members, $0; nonmembers, $10 Passing score: 9 correct (75%) Category: A, Synergy CERP A Test writer: Todd M. Grivetti, RN, BSN, CCRN Program evaluation Name Yes K K K For faster processing, take this CE test online at http://ccn.aacnjournals.org (“CE Articles in this issue”) or mail this entire page to: AACN, 101 Columbia Aliso Viejo, CA 92656. Objective 1 was met Objective 2 was met Objective 3 was met Content was relevant to my nursing practice K My expectations were met K This method of CE is effective for this content K The level of difficulty of this test was: K easy K medium K difficult To complete this program, it took me hours/minutes. No K K K K K K Member # Address City State Country ZIP Phone E-mail RN Lic. 1/St Payment by: Card # RN Lic. 2/St K Visa K M/C K AMEX K Discover K Check Expiration Date Signature The American Association of Critical-Care Nurses is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation. AACN has been approved as a provider of continuing education in nursing by the State Boards of Nursing of Alabama (#ABNP0062), California (#01036), and Louisiana (#ABN12). AACN programming meets the standards for most other states requiring mandatory continuing education credit for relicensure.