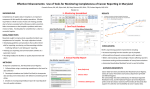
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
17 Western Maryland Parkway, Suite 100 Hagerstown, MD 21740 755 Norland Avenue, Suite 102 Chambersburg, PA 17201 Phone: 301-797-9240 Fax: 301-797-0008 Toll Free: 1-800-797-3666 www.pnsi.org Dear Patient: Your appointment with Dr. at is scheduled for . Please bring the following items with you the day of your appointment, if applicable: • • • • • • • Your insurance card(s) Your driver's license (or other photo identification) Any radiology films (MRI, CT, X-rays, etc . . .) You may bring the actual films or a CD. Also a copy of the report. If you do not have your films/CD, your appointment will be rescheduled. Any test results related to your problem. The enclosed Patient Information and Patient History forms filled out completely. A referral from your primary care physician if you belong to an HMO or managed care plan. Your insurance company will not allow our physician to see you without your referral. If you are claiming an injury from an auto accident or workmen's compensation accident, please bring complete billing information with you: the name, address and phone number of the insurance company, the claim number, and the authorization for your consultation. If you do not bring all the above information, your appointment will be rescheduled. We accept many insurance plans, HMO's, and Medicare. We will submit these claims to your insurance company. We do ask that you be prepared to pay any applicable co-payment at the time of service. If you have any questions prior to your appointment, please call our office at 301-797-9240 or 1-800-797-3666 between 8:30 am and 4:15pm. Thank you. OFFICE LOCATIONS Parkway Neuroscience & Spine Institute is located just West of Hagerstown off Route 40 at 17 Western Maryland Parkway, Suite 100. It is just several blocks from the Centre at Hagerstown Shopping Center and down the street from First Data Corporation. A satellite office is located at the Keystone Pavilion in Chambersburg. Please see the reverse side of this page for detailed directions. 1 #2 NPP Rev 5/11 DIRECTIONS: HAGERSTOWN, MARYLAND 17 WESTERN MARYLAND PARKWAY, SUITE 100 From the North (Chambersburg, Carlisle and Harrisburg) • • • Follow I-81 South to Maryland Exit 6 (Route 40) Travel East towards Hagerstown and take the first right onto Western Maryland Parkway. The Institute is located on your right just past First Data Corporation. From the North (Waynesboro) • • • Follow Route 66 (Leitersburg Pike) South to Maryland Route 40 (Franklin Street) Travel West towards I-81 and the Centre at Hagerstown Shopping Center and turn left onto Western Maryland Parkway The Institute is located on your right just past First Data Corporation From the South (Martinsburg, Winchester) • • • Follow I-81 North to Maryland Exit 6 (Route 40) Travel East towards Hagerstown and take the first right onto Western Maryland Parkway. The Institute is located on your right just past First Data Corporation. From the West (Cumberland) • • • Take I-70 East to I-81 and travel North to Maryland Exit 6 (Route 40) Travel East towards Hagerstown and take the first right onto Western Maryland Parkway. The Institute is located on your right just past First Data Corporation. From the East (Frederick, Shady Grove, Germantown) • • • Take I-70 West to I-81 and travel North to Maryland Exit 6 (Route 40) Travel East towards Hagerstown and take the first right onto Western Maryland Parkway. The Institute is located on your right just past First Data Corporation. CHAMBERSBURG, PENNSYLVANIA 755 NORLAND AVENUE, SUITE 102 From the North (Carlisle, Harrisburg) • • • • • 81 South to Chambersburg Exit 17 Right onto Walker Road Right onto Norland Avenue Right into Summit Health Campus First building on the left - Summit Keystone Pavilion From the South (Maryland, West Virginia) • • • • • 81 North to Chambersburg Exit 17 Left onto Walker Road Right onto Norland Avenue Right into Summit Health Campus First building on the left - Summit Keystone Pavilion 2 #2 NPP Rev 5/11 Date____________________ PATIENT INFORMATION Last Name______________________________First__________________________Middle_____________ Address________________________________City__________________________State_____Zip_______ Home Phone# (____)_______________ Cell# (____)_______________ Work# (____)_________________ Date of Birth _____/_____/_____ Age_____ Social Security #___________________Sex (circle) M F Marital Status (circle) Married Single Widow(er) Divorced Separated Primary Care Physician _________________Address____________________________________________ Office Phone # (must be completed)(_____)_______________________ Referring Physician_____________________Address___________________________________________ Office Phone # (must be completed) (_____)_______________________ Employer ____________________________Address____________________________________________ Occupation __________________________Work Phone # (_____)___________________________ Spouse or Parent’s Name______________________ Date of Birth _____/_____/_____ Spouse or Parent’s Occupation_________________ Employer____________________________________ Employer’s Address__________________________________ Employer’s Phone # (_____)_____________ EMERGENCY CONTACT Name___________________________Relationship____________________Phone #(_____)____________ INSURANCE INFORMATION PPO/HMO/Commercial__________________________________________________________________ Name of Insurance Co. Policy Number Address Do you have Medicare? (circle) Yes No If yes, Medicare #________________ Effective date_______ Do you have Medicaid? (circle) Yes No If yes, Medicaid #________________Effective date________ Is Medicare your primary or secondary insurance? (circle) Primary Secondary Is Medicaid your primary or secondary insurance? (circle) Primary Secondary Medicare Supplemental Insurance:________________________________________________________ Name Address Policy Number Does your insurance require a second surgical opinion? Yes No Does your insurance require precertification? Yes No If yes, please supply your insurance’s phone number (_____)_________________________ Is this a work related injury? Yes No If yes, date of accident _____/_____/_____ Claim#____________________ Compensation Insurance______________________________________ Carrier’s Address __________________________________Phone# (_____)______________________ Claim’s Representative______________________________ Employer’s Name____________________ Is this injury related to a motor vehicle accident? Yes No If yes, date of accident_____/____/_____ Auto Insurance Carrier_______________________________ Policy #____________________________ Auto Insurance Address _____________________________Phone # (____)_______________________ ________________________________________ Date________________ Signature of patient or legal guardian (Required for Medicare, Medicaid, and Commercial Insurances) 3 #2 #2 NPP Rev 5/11 Please read carefully and sign the section(s) that apply to you: Non-Medicare patients: • • • • • • All charges are due at the time professional services are rendered. The patient is responsible for all fees. The fee ticket may be used to file insurance claims. For guardian of a minor: I understand that I am fully responsible for this minor’s medical charges and agree to pay all charges for services rendered by Parkway Neuroscience & Spine Institute. I hereby authorize Parkway Neuroscience & Spine Institute to furnish information to any insurance company or authorized agency specified regarding information concerning my medical care. For those services provided and submitted to my insurance company, I hereby authorize payment of medical benefits to Parkway Neuroscience & Spine Institute. Signature:_________________________________ Date:________________________ Medicare Patients Only: I authorize any holder of medical or other information about me to release to the Social Security Administration and Health Care Financing Administration or its intermediaries or Carriers any information needed for this or related Medicare claim. I permit a copy of this authorization to be used in place of the original and request payment of medical insurance benefits to the party who accepts assignment. Regulations pertaining to Medicare assignment of benefits apply. I also understand that I am responsible for the deductible, coinsurance, and any non-covered services as determined by Medicare. Signature:_________________________________ Date:________________________ Medicare Supplemental Insurers’ MEDIGAP Assignment of Benefits: Section 4081 of the Omnibus Budget Reconciliation Act of 1987 provides an additional participation incentive for participating physicians by providing payment directly for assigned Medicare supplemental (MEDIGAP) insurance benefits. I understand my signature gives authorization for my physician to bill claims directly to my recognized MEDIGAP insurance carrier and for payments to be received directly. This allows for medical information to be forwarded to the insurance carrier as necessary. The Explanation of Medicare Benefits received from Medicare will display the following message to notify you that a claim has been submitted to your MEDIGAP carrier: “Because you are assigned MEDIGAP benefits, information regarding your claim will be sent to your private insurer within 30 days.” I also understand that any deductibles, coinsurances, and non-covered services will be my responsibility. Signature:_________________________________ 4 Date:______________________ #2 NPP Rev 5/11 Patient Name:_____________________________________ Date of Birth:_________________________________ Marital Status: □ Single □ Married □ Divorced □ Widowed Height:_____________________________________Weight:_____________________________________________ Referring Doctor:____________________________Primary Care Dr.:_____________________________________ Preferred Pharmacy: (name/address)__________________________________________________________________ ALLERGIES: Do you have any drug allergies? □ Yes □ No If yes, please describe the allergy and the reaction:_____________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ Do you have any other allergies we should know about? □ Yes □ No If yes, please describe the allergy and the reaction:_____________________________________________________ _____________________________________________________________________________________________ FAMILY HISTORY: Family Member Mother Father Sister/Brother (please circle) Sister/Brother (please circle) Sister/Brother (please circle) Alive/Deceased A D A D A D A D A D Age Medical Problems Are there diseases which are common in your family? (If yes, please list.)___________________________________ _____________________________________________________________________________________________ Has any family member had a history of surgery for their back or neck, or had problems with their back or neck?___ _____________________________________________________________________________________________ _____________________________________________________________________________________________ 5 NPP Rev 5/11 PAST MEDICAL HISTORY: Please circle yes or no. Y N Use of Blood Thinners Y N Anxiety Disorder Y N Aortic Aneurysm Y N Arthritis Y N Asthma Y N Bipolar Disorder Y N Cancer _____________________________ Y N Congestive Heart Failure Y N COPD (Chronic Obstructive Pulmonary Disease) Coronary Artery Disease Y N Y N Stroke (CVA) Y N Degenerative Joint Disease Y N Depression Y N Diabetes Y N Fibromyalgia Y N Glaucoma Y N Y N Y N Y N Y N Y N Y N Y N Y N Y N Y N Y N Y N Y N Y N Head Injury, with skull fracture Head Injury, without skull fracture HIV High Cholesterol High Blood Pressure Heart Attack Infectious Diseases (i.e. MRSA, TB) Osteoarthritis Osteoporosis Rheumatoid Arthritis Seizure Disorder Sleep Apnea Thyroid Disease Tuberculosis Vertebral Artery Stenosis Complications from any surgery? □ Yes □ No Please explain:_________________________________________ _____________________________________________________________________________________________ Do you take antibiotics before procedures? □ Yes □ No Why:_________________________________________ _____________________________________________________________________________________________ PAST SURGICAL HISTORY: Please list all previous surgical procedures and date your surgery was performed. □ Carpal Tunnel_____________________________ □ Spinal Cord Injury____________________________ □ Craniotomy_______________________________ □ Spinal Cord Stimulator_________________________ □ Disectomy________________________________ □ Spinal Fusion-Cervical_________________________ □ Endarterectomy____________________________ □ Spinal Fusion-Lumbar_________________________ □ Intrathecal Pump___________________________ □ Spinal Fusion-Thoracic________________________ □ Kyphoplasty______________________________ □ Ulnar Nerve Release___________________________ □ Laminectomy-Cervical______________________ □ Vertebroplasty________________________________ □ Laminectomy-Lumbar______________________ □ Other_______________________________________________________________________________________ □ Appendectomy____________________________ □ Hysterectomy________________________________ □ C-Section________________________________ □ Sinus Surgery________________________________ □ Gall Bladder Removal______________________ □ Pancreatic Surgery____________________________ □ Dental___________________________________ □ Prostatectomy________________________________ □ D&C____________________________________ □ Large Bowel Resection_________________________ □ Eye Surgery_______________________________ □ Small Bowel Resection_________________________ □ Fracture Repair____________________________ □ Stomach Resection____________________________ □ Heart Surgery_____________________________ □ Rotator Cuff Repair___________________________ □ Angioplasty____________________________ □ Thyroidectomy_______________________________ □ Bypass________________________________ □ Subtotal__________________________________ □ Stent__________________________________ □ Total____________________________________ □ Valve Replacement______________________ □ Tonsillectomy________________________________ □ Other_________________________________ □ Tubal Ligation_______________________________ □ Hernia Repair_____________________________ □ Vasectomy___________________________________ □ Other_______________________________________________________________________________________ 6 NPP Rev 5/11 SOCIAL HISTORY: Occupation:____________________________________________________________________________________ A: Physically, do you consider your job: □ Heavy □ Moderate □ Light B: If retired, what was your prior occupation?___________________________________________________ Is someone available to care for you in your home if the need arises? □ Yes □ No Do you live in a: □ House □ Apartment □ Other:_____________# of stories: 1 2 3 Do you exercise regularly? □ Yes □ No Describe:__________________________________________________ Do you have a history of drug abuse or drug addiction? □ Yes □ No Alcohol Use: I use alcohol: □ Never □ Occasional □ Moderate □ Heavy I have a history of heavy alcohol use: □ Yes □ No Tobacco Use: Do you smoke? □ Yes □ No I currently smoke___packs per day and have for___years. I smoked in the past___packs per day for___years. Are you at risk for AIDS (e.g. sexual history, drug use, previous transfusion)? □ Yes □ No CURRENT MEDICATIONS: Please list all. Medication 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Dose 7 Frequency NPP Rev 5/11 REASON FOR VISIT: Describe your current problem and how it began. Please list all symptoms leading to today’s visit:_______________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ Date symptoms began:___________________________________________________________________________ Is your current problem a result of: □ Car Accident □ Work Accident □ Other/Unknown Date of injury/accident:___________________________________________________________________________ Are you currently off work because of your problems? □ Yes □ No Is a lawyer involved in your case? □ Yes □ No If yes, name of lawyer:__________________________________ PAIN HISTORY: (if not applicable, skip to next section) What makes your symptoms better?_________________________________________________________________ What makes your symptoms worse?_________________________________________________________________ What specific activities are you having difficulty with that you hope to change as a result of treatment?___________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ In order to get better, you will be expected to participate in your treatment. This may include doing exercises or avoiding certain activities. How committed are you to participating in your treatment? □ Very committed □ Somewhat committed □ Not very committed Is there anything that will limit your ability to participate in therapies? □ Yes □ No Explain:_______________________________________________________________________________________ _____________________________________________________________________________________________ What tests have you had done for your problem? □ X-rays □ CT scan □ MRI □ Blood tests □ Other:______________________________________________________________________________________ What treatments have you had for your problem? □ Medications □ Physical Therapy □ Chiropractic □ Injections □ Surgery □ Other________________________________________________________________________ Please describe their effect:_______________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ Would you consider surgery if it were recommended? □ Yes □ No 8 NPP Rev 5/11 REVIEW OF SYSTEMS: Please circle yes or no. General: Y Y Y N N N Weight Gain greater than 10 lbs. Weight Loss greater than 10 lbs. Obesity N Bruising Skin: Y HEENT: Y Y Y Y Y Y Y Y Y N N N N N N N N N Blurred Vision Head Injury Double Vision Visual Disturbances Visual Loss Hearing Loss Ringing in the Ears Seasonal Allergies Hoarseness N N Neck Mass Swollen Glands Neck: Y Y Respiratory: Y Y N N Chronic Cough Difficulty Breathing Breast: Y N Nipple Discharge Cardiovascular: Y N Chest Pain Y N Irregular Heart Beat Y N Elevated Blood Pressure Y N Rapid Heart Rate Y N Shortness of Breath Y N Swelling of the Feet Gastrointestinal: Y N Change in Bowel Habits Y N Indigestion Y N Jaundice Y N Nausea Y N Vomiting Genitourinary: Y N Change in Bladder Habits Y N Frequency Y N Hesitancy Y N Incontinence Musculoskeletal: Y N Back Pain Y N Muscle Cramps Y N Arm Weakness Y N Arm Pain Y N Leg Weakness Y N Leg Pain Y N Neck Pain Y N Neck Stiffness Neurological: Y Y Y Y Y Y Y Y Y Y Y N N N N N N N N N N N Decreased Memory Difficulty Speaking Dizziness Fainting Headaches Incoordination Loss of Consciousness Seizures Stroke Weakness in Extremities Leg Pain with Walking Psychiatric: Y Y Y N N N Anxiety Depression Inability to Concentrate Endocrine: Y N Thyroid Problems Hematology: Y Y Y N N N Abnormal Bleeding Anemia Blood Clots Other:________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ 9 NPP Rev 5/11 THE ABOVE INFORMATION IS ACCURATE TO THE BEST OF MY KNOWLEDGE _____________________________________________ Patient signature _____________________________________________ Date I HAVE REVIEWED THE ABOVE INFORMATION (PARKWAY OFFICE USE ONLY) _____________________________________________ Physician Signature _____________________________________________ Date _____________________________________________ Physician Name (printed) _____________________________________________ Date reviewed & initials _____________________________________________ Date reviewed & initials _____________________________________________ Date reviewed & initials _____________________________________________ Date reviewed & initials _____________________________________________ Date reviewed & initials Revised 8/2010 10 Parkway Neuroscience and Spine Institute NPP Rev 5/11