Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
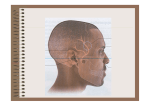
Letter t o E d i t o r Acute parotid gland swelling after endoscopy: An unusual complication Sir, The scope of diagnosing and treating many gastrointestinal (GI) diseases has widened significantly due advances in endoscopic procedures. Upper GI endoscopy is a safe procedure in the present gastroenterology practice. In most of the countries it is performed under topical anesthesia. In the past, the procedure was normally done under parenteral use of sedation and antispasmodic in addition to local lignocaine. There were a few complications related to the procedure and medications, which need to be observed carefully even in the present era of practice of endoscopy. Swelling of the salivary glands is a rare complication reported in the literature. The sudden appearance of swelling will cause anxiety for both the patient and doctor; however, it is generally benign condition which is transient and painless, and requires no specific treatment.[1] We report here a case of acute parotid gland swelling developed immediately after upper GI endoscopy. CASE REPORT A 56‑year‑old female was referred for upper GI endoscopy to evaluate esophageal varices. She was suffering from portal hypertension with hypersplenism for last 1 year. One year ago she had variceal band ligation for acute bleeding from varices. She lost to follow up subsequently and reported after a few months and found to be severely anemic (Hb 4.8 g/L). The other hematology work ups suggested hypersplenism without any coagulation defect. Upper GI endoscopy was performed in left lateral position using topical pharyngeal anesthesia with 10% lidocaine spray before the procedure. Esophageal varices (grade 4) were seen with four columns extending from mid esophagus to lower esophageal sphincter. There was no evidence of active or recent bleeding in the esophagus or stomach on endoscopic examination. The grade 2 gastro‑esophageal varices were detected at the cardia. The stomach mucosa resembled “water melon” appearance suggestive of portal gastropathy. The patient had frequent bouts of coughing and retching during the procedure. After the completion of diagnostic procedure, scope was withdrawn. Band ligation and sclerotherapy was advised. However, the patient complained of a painful swelling [Figure 1] on the right jaw in front of the ear. The swelling had developed immediately after the procedure. It was 2 cm in size, globular shape, and tender with firm feel. There was no redness of the skin over the swelling or any exudate. Opening of mouth was limited due to mild stiffness of the right temporomandibular (TM) joint and pain. The possible injury to any of structures involving TM joint, buccal mucosa, or salivary duct with subsequent parotid swelling was under consideration. 23 The patient did not have chest pain, dyspnea, fever, or cyanosis. Examination of oral cavity including teeth was normal. X ray of TM joint was normal and ultrasound of the swelling showed mild parotid enlargement. The swelling gradually decreased over next 1 hour and had completely subsided by evening, though mild pain still remained. The patient was treated with paracetamol for pain relief in addition to medication for portal hypertension and anemia. DISCUSSION This is a rare complication of flexible upper GI endoscopy,[1] bronchoscopy[2] and endotracheal intubation for anesthesia. The case reports are published in the past[3,4] and almost all of them except one from Turkey and Saudi Arabia[5,6] have been reported before 1990. Parotid and or submandibular glands are generally affected (unilateral or bilateral.) Several possible mechanisms have been proposed in the etiopathogenesis, since the exact mechanism is unknown. Some authors have concluded that it may be due to an adverse drug reaction such as to atropine, morphine, or suxamethonium;[3,7] however, there was no drug in common in all of the reported cases. Matsuki et al.[4] and Attas et al.[7] proposed that coughing and straining may lead to venous congestion of the salivary glands and mild swelling of salivary glands. Couper[8] reported that manipulation of the head during endoscopy may lead to obstruction of the thoracic inlet venous drainage with subsequent congestion of the parotid glands. Finally, Bonchek[3] and Strowbridge[9] considered the most likely explanation to be that instrumentation of the upper airway or esophagus stimulates a reflex arc, with the afferent stimulus coming from the tongue, mouth, Figure 1: Right-sided parotid swelling Oncology, Gastroenterology and Hepatology Reports| Jan-Jun 2014 | Vol 3 | Issue 1 Letter to Editor or pharynx, and intense parasympathetic stimulation resulting in vasodilatation and transient enlargement of the glands. The retrograde flow of air through the Stenon’s orifice during straining and coughing under anesthesia, retention of secretions causing occlusion of the salivary ducts, in addition to use of pre‑procedure drugs and systemic dehydration are the most commonly accused factors.[10] SUMMARY This rare complication of upper GI endoscopy should be kept in mind during and after the procedure. It is imperative that both endoscopist and physician should be aware of this benign and transient complication of the procedure. A patient needs to be reassured after ruling out serious complications of procedure. No specific intervention is required, since it is a self‑limiting condition Arvind Bamanikar, Arjun Lal Kakrani, Rajdeep More Department of Medicine, Padmshree Dr. D. Y. Patil Medical College, Hospital and Centre, Pimpri, Pune, Maharashtra, India REFERENCES 1. Ziccardi V, Molloy PJ. Parotid swelling after endoscopy. Gastrointest Endosc 1992;38:520. 2. Blackford RW. Recurrent swelling of parotid and submaxillary gland following bronchoscopy. Ann Otol Rhinol Laryngol 1974;53:54‑64. 3. Bonchek LI. Salivary gland enlargement during induction of anaesthesia. JAMA 1969;209:1716‑8. 4. Matsuki A, Wakayama S, Oyama T. Acute transient swelling of the salivary glands during and following endotracheal anaesthesia. Anaesthesist 1975;24:125‑8. 5. Işler M, Akin M, Senol A, Yariktaş M. Acute bilateral parotid gland swelling after endoscopy. Turk J Gastroenterol 2011;22:351‑62. 6. Postaci A, Aytac I, Oztekin CV, Dikmen B. Acute unilateral parotid gland swelling after lateral decubitus position under general anesthesia. Saudi J Anaesth 2012;6:295‑7. 7. Attas M, Sabawala PB, Keats AS. Acute transient sialadenopathy during induction of anaesthesia. Anaesthesiology 1968;29:1050‑2. 8. Couper JL. Benign transient enlargement of the parotid glands associated with anaesthesia. S Afr Med J 1973;47:316‑8. 9. Strowbridge NF. Acute salivary gland enlargement following instrumentation of the upper airway. J R Army Med Corps 1987; 133:163‑5. 10. Narang D, Trikha A, Chandralekha C. Anethesia mumps and Morbit obesity. Acta Anaesthesiol Belg 2010; 6:83‑5. Access this article online Quick Response Code: Website: www.oghr.org Address for the Correspondence: Dr. A. A. Bamanikar, Padmshree Dr. D. Y. Patil Medical College, Hospital and Centre, Sant Tukaram Nagar, Pimpri, Pune - 411 018, India. E‑mail: [email protected] DOI: 10.4103/2348-3113.126646 Staying in touch with the journal 1) Table of Contents (TOC) email alert Receive an email alert containing the TOC when a new complete issue of the journal is made available online. To register for TOC alerts go to www.oghr.org/signup.asp. 2) RSS feeds Really Simple Syndication (RSS) helps you to get alerts on new publication right on your desktop without going to the journal’s website. You need a software (e.g. RSSReader, Feed Demon, FeedReader, My Yahoo!, NewsGator and NewzCrawler) to get advantage of this tool. RSS feeds can also be read through FireFox or Microsoft Outlook 2007. Once any of these small (and mostly free) software is installed, add www.oghr.org/rssfeed.asp as one of the feeds. Oncology, Gastroenterology and Hepatology Reports| Jan-Jun 2014 | Vol 3 | Issue 1 24