Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
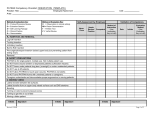
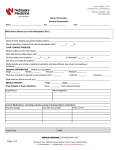
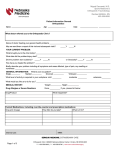
Name: DOB: Chart: Date of Visit JEWETT ORTHOPAEDIC CLINIC Medical History - Page 1 Age: Height: Weight: Primary Physician: Please note, items left blank indicate a negative response. PAST MEDICAL HISTORY Bleeding disorders Blood clots/DVT Stroke Seizures Sleep apnea Asthma/Emphysema High blood pressure Heart Disease Arrhythmia Anemia Diabetes Thyroid disorders SURGICAL PROCEDURES: Tonsils Appendix Thyroid Indicate all medical conditions you have experienced. None Uterus Breast Vascular Prostate Hernia Other (list in space below) Indicate all medical conditions experienced by any parent, sibling, or child None Cancer Stroke Seizures Osteoporosis Rheumatoid arthritis Gout Fibromyalgia Birth defects Other (list in space below) Indicate all surgical procedures (include approximate dates). None Heart Colon Gallbladder FAMILY HISTORY: Liver disorder Stomach ulcers Kidney problems Prostate enlargement Cancer Glaucoma High blood pressure Heart disease Diabetes Kidney problems Bleeding disorders Blood clots/DVT Osteoporosis Birth defects Anesthesia complications SOCIAL HISTORY: Occupation: Marital status: Living alone: Tobacco use: Cigarettes Other: Alcohol use: Beer Single Married Yes No Never Previous packs per day: None Wine REVIEW OF SYSTEMS: Fevers/Night sweats Shaking/Chills Recent weight loss Bleeding gums Frequent nosebleeds Visual problems Hearing problems Dizziness/Fainting Occasionally Liquor None Student Retired Widowed Divorced with spouse with family Currently every day number of yrs: number of yrs: Weekly Daily Disabled (when): with other: Currently some days Quit when: Quit when: Quit when: Indicate all symptoms that you are presently experiencing. Frequent headaches Morning cough Shortness of breath Coughing up blood Hoarseness Chest pain Abnormal heartbeat Ankle swelling Nausea/Vomiting Stomach pain Blood in stools Loose stools Loss of appetite Difficulty with urination Pain/Burning on urination Blood in urine Rashes Severe itching Bruising/Bleeding easily Calf cramps Joint pain Joint swelling Loss of height Irregular periods Name: DOB: Chart: Date of Visit JEWETT ORTHOPAEDIC CLINIC Medical History - Page 2 MEDICATIONS: None List all prescription and non-prescription medications and supplements. Name of medication ALLERGIES: None Strength/Dose Frequency Indicate all allergies you have to medications and foods. Include reaction, i.e. nausea, vomiting, itching, rash, swelling, difficulty breathing Penicillin Sulfa Aspirin Codeine Morphine Iodine Latex Milk Other - List below Print name of patient (or authorized representative) Signature of patient (or authorized representative) Date Name of Provider Provider Signature Date Name: DOB: Chart: Date of Visit JEWETT ORTHOPAEDIC CLINIC Medical History - Page 3 SUPERCONFIDENTIAL INFORMATION: Indicate all conditions for which you have received treatment. None Mental health conditions (depression, anxiety, etc.) Substance abuse (alcohol, narcotics, etc.) Illegal drug use HIV / AIDS Sexually transmitted diseases (STD's) Minor pregnancies (pregnancy under the age of 18) If you have indicated any of the conditions above, please initial the corresponding categories listed below which will authorize Jewett Orthopaedic Clinic to disclose that information to third parties for treatment or payment purposes in the event that it is requested by said third parties or required by law Initials: Mental health information Initials: HIV/AIDS information Initials: Substance abuse information Initials: STD information Initials: Illegal drug use information Initials: Minor pregnancy information Are you pregnant or could you be pregnant? No Yes If yes, due date: I HAVE READ AND UNDERSTAND THE INFORMATION IN THIS CONSENT. I AM THE PATIENT OR AUTHORIZED TO ACT ON BEHALF OF THE PATIENT TO SIGN THIS DOCUMENT VERIFYING CONSENT TO THE ABOVE TERMS. Print name of patient (or authorized representative) Signature of patient (or authorized representative) Date Reason patient is unable to sign and representative's relationship to patient or authority to sign on behalf of patient Name of Provider Provider Signature Date