Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
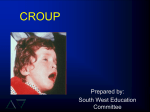
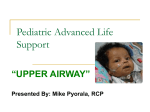
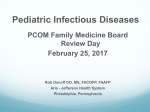
...&more COMBATING INFECTION Viral croup in children By Janelle Gardner, RN,C, PhD IT’S A COLD winter night when 12month-old Jacob and his exhausted parents arrive at the ED. Jacob has had signs of a head cold and a low-grade fever for 2 days. He’s developed a distinctive barking cough, hoarseness, and inspiratory stridor. His respiratory rate is 50 breaths/minute, and the pulse oximeter reading is 92%. Jacob’s signs and symptoms suggest croup. What are the appropriate nursing interventions for Jacob? What is croup? Croup is a generic term applied to a group of common respiratory illnesses— mostly seen in children—that result from edema of the larynx, trachea, and bronchi. Croup can be categorized as viral or bacterial. In this article, I’ll focus on viral croup, which is the more common type. Viral croup is also the most common form of airway obstruction in children ages 6 months to 6 years and is one of the leading causes of hospitalization in children under age 4.1 What causes viral croup? Viral croup is a viral invasion of the upper airway that extends throughout the larynx, trachea, and bronchi. Caused by various viruses, most commonly parainfluenza viruses types 1, 2, and 3, it affects more boys than girls. The peak season in the United States is late fall, but it can occur at any time of year. In most cases, viral croup is mild to moderate in severity, but it can progress to respiratory failure (see Assessing croup severity). The invading virus causes inflammation and edema in the child’s trachea and www.nursing2008.com Inflamed laryngeal area Inflamed subglottic tissue Usually worse at night, signs and symptoms generally peak on the second or third night.2 The child may prefer to sit up or be held upright because he can breathe more easily in this position. Signs and symptoms may be more severe in children 3 years of age and younger. Assessing the patient A diagnosis of viral croup usually rests on patient history and presenting clinical signs and symptoms. However, posterior-anterior Narrowed and lateral X-rays of the neck may trachea be taken if the diagnosis is in question. Another reason for taking X-rays is to rule out foreign body airway obstruction. About Viral croup causes inflammation and edema of the 50% of children with viral croup upper respiratory tract. show a tapered symmetric subglottic narrowing (a “steeple larynx. The resulting airway obstruction sign”) on plain neck radiography.1 causes a characteristic barking cough, Try to keep a child with viral croup hoarseness, inspiratory stridor, and varycalm because crying and agitation can ing degrees of respiratory distress.1 exacerbate signs and symptoms. Focus Respiratory distress is exacerbated by your physical assessment on the respilarge amounts of thick, tenacious secreratory system. tions that further obstruct the airway. Acute airway inflammation in children Maintain, manage, and medicate When caring for a child with croup, is dangerous because a child’s larynx is focus on maintaining his airway. Invery narrow, so even small amounts of terventions include humidification, mucus and edema can obstruct it. medications, and supplemental oxygen. Inspired humidified air that’s cooler Identifying viral croup develops than body temperature cools and A child with viral croup first soothes airway mucosa and triggers upper respiratory signs and symptoms vasoconstriction, decreasing edema in (runny nose, sore throat, low-grade the respiratory tract. Cool moist air also fever). Over the next few days, signs moistens and thins secretions. Conand symptoms progress to those of trolled delivery of 40% humidity (low croup. April | Nursing2008 | 57 ...& more COMBATING INFECTION humidity) or humidity by blow-by is the most effective technique3 because it lowers anxiety in children who don’t want to cooperate with oxygen therapy. Croup tents are seldom used because they frighten children and make observation more difficult. For decades, nebulized racemic epinephrine has been the standard medication for children with moderate to severe croup. Mixed with 0.9% sodium chloride solution and delivered with humidified oxygen, it reduces inspiratory stridor and intercostal retractions within 30 minutes of treatment. The medication’s effectiveness lasts about 2 hours.1 Common adverse reactions include tachycardia and hypertension. Oral or intramuscular dexamethasone may be ordered to reduce airway inflammation and edema. It has a long half-life (24 to 48 hours). Adverse reactions are rare. A child with mild croup who responds well to treatment may be sent home from the ED after 3 or 4 hours of observation. If signs and symptoms of respiratory distress persist after initial treatment, he’ll be admitted to the hospital for further observation and management. Keeping an eye on croup When a child has been diagnosed with croup, monitor him closely and quickly identify any alterations in airway patency. Follow these guidelines. • Monitor him for tachypnea and tachycardia, which signal the child’s increasing respiratory effort. • Assess his breath sounds and monitor for retractions, nasal flaring, stridor, and cyanosis. • Use a cardiac monitor and pulse oximeter for continuous monitoring. • Position the child for comfort and remember that a need to move to a more upright position may indicate increased respiratory distress. 58 | Nursing2008 | April ASSESSING CROUP SEVERITY Level of severity Characteristics Mild • Occasional barking cough • Limited or no stridor at rest • Mild or no suprasternal or intercostal retractions • Frequent barking cough • Easily audible stridor at rest • Suprasternal and sternal wall retractions at rest • Little to no distress or agitation • Frequent barking cough • Prominent inspiratory and occasionally expiratory stridor • Marked sternal wall retractions • Significant distress and agitation • Barking cough (often not prominent) • Audible stridor at rest (occasionally hard to hear) • Sternal wall retractions (may not be marked) • Lethargy or decreased level of consciousness • Often dusky complexion without supplemental oxygen Moderate Severe Impending respiratory failure Adapted from Bjornson CL, Johnson DW, Croup—treatment update, Pediatric Emergency Care, December 2005. What parents need to know Viral croup usually runs its course in 3 to 7 days. Give parents the following advice to keep their child comfortable at home. • Hold your child in an upright position, which can help him breathe more easily. Hold him in your lap or place him in a favorite chair or infant seat. • Moist air seems to help. Run hot water in the bathtub with the door closed and hold your child while he breathes in the humidified air. • A walk in cool nighttime air can help too. Dress your child warmly and take a short walk with him. • Try to keep your child calm and relaxed; crying or becoming agitated will make breathing more difficult. • Administer a fever reducer such as ibuprofen or acetaminophen as directed by the health care provider. • If he doesn’t respond to treatments or his signs and symptoms get worse, call your health care provider immediately. How’s Jacob? Jacob was diagnosed with viral croup and admitted to the hospital. Intravenous flu- ids were administered to prevent dehydration, and supplemental oxygen with humidity was administered via a blow-by for hypoxemia. Jacob received oral dexamethasone and humidified racemic epinephrine. He was monitored closely, his signs and symptoms improved, and he was discharged after 48 hours. ‹› REFERENCES 1. Knutson D, Aring A. Viral croup. American Family Physician. 69(3):535-540, February 2004. 2. Dykes J. Managing children with croup in emergency departments. Emergency Nurse. 13(6):14-19, October 2005. 3. Scolnik D, et al. Controlled delivery of high vs. low humidity vs. mist tent for croup in emergency departments: A randomized controlled trial. The Journal of the American Medical Association. 295(11):1274-1280, March 15, 2006. RESOURCES Ball JW, Bindler RC. Child Health Nursing: Partnering with Children and Families. Prentice Hall, 2006. Bjornson CL, Johnson DW. Croup—treatment update. Pediatric Emergency Care. 21(12):863-870, December 2005. Bjornson CL, Johnson DW. Pediatric practice. That characteristic cough: When to treat croup and what to use. Patient Care for the Nurse Practitioner. 7(1):13, January 2004. Mayo Clinic. Croup. http://www.mayoclinic.com/ health/croup/DS00312/DSECTION=1. Nursing2008 Drug Handbook, 28th edition. Lippincott Williams & Wilkins, 2008. Web site last accessed on March 3, 2008. Janelle Gardner is a professor at California State University’s School of Nursing in Chico. www.nursing2008.com