Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
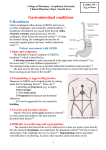
Heartburn and GERD: Primary Care Management Wendy L. Wright, MS, RN, ARNP, FAANP Family Nurse Practitioner Wright & Associates Family Healthcare Amherst, New Hampshire Objectives Upon completion of this lecture, the participant will be able to: 1. Identify the differences between heartburn and GERD 2. Discuss the nonpharmacologic treatment options for the individual with heartburn and GERD 3. Discuss the pharmacologic treatment options for the individual with heartburn and GERD EE 52 year old female presents with anterior chest pain; non-radiating and not associated with any exertion. Occurs daily unless she avoids most foods. Has tried OTC antacids without much effect. Aggravating factors: Foods – fatty meals, spicy meals Alleviating factors: None Medications: Lexapro 5 mg one daily EE (Continued) PMH Anxiety disorder Postmenopausal Overweight L5-S1 L5 S1 disc surgery No previous work-up for symptoms Physical Examination Unremarkable except for 1+ tenderness epigastric region 12-lead ECG: No abnormalities Hemocult: negative What Does EE Have?? Episodic heartburn Frequent heartburn GERD Chest pain of cardiac origin Cholecystitis/Cholethiasis Gastric/duodenal pathology H. pylori induced pathology Heartburn: What is it? Heartburn has many names Indigestion Acid regurgitation Sour stomach Official name: pyrosis Characterized by Burning in the chest Burning in the upper abdomen Rises into the throat Most common symptom of GERD Seems to be ubiquitous in the United States Heartburn Population: Prevalence In the United States, an estimated 65% of the total adult population experiences heartburn1 Frequent heartburn occurs in up to 46% of pp y 50 consumers with heartburn or approximately million people 1-3 Heartburn occurs daily in 7% to 10% of the adult population This is approximately 25 million individuals 4,5 1. National Omnibus Study 2003 #US035247, data in Sponsors file. 2. P&G MRD#US972782, data in Sponsor’s file. Yankelovich 3. Oliveria SA, Christos PJ, Talley NJ, Dannenberg AJ. Heartburn risk factors, knowledge, and prevention strategies: a population-based survey of individuals with heartburn. Arch Int Med. 1999;159:1592–1598. 4. P&G MRD#US983190, data in Sponsor’s file. 5. Nebel OT, Fornes MF, Castell DO. Symptomatic gastroesophageal reflux: incidence and precipitating factors. Dig Dis. 1976; 21(11):953–956. The Frequent Heartburn Population: Demographics Slightly more women (58%) than men report frequent heartburn 1,2 The mean age for FHB sufferers is 45 to 50 years1,9 Geographic location, marital status, family status (children), educational level, job type and level, and socioeconomic status all play a role in the tendency to develop heartburn 10 1. Oliveria SM, Christos PJ, Talley NJ, Dannenberg AJ. Heartburn risk factors, knowledge, and prevention strategies: a population-based survey of individuals with heartburn. Arch Int Med. 1999; 159: 1592-1598 2. Yankelovich Partners n= 507 FBH. Data in sponsor’s file 3. P&G MRD #US983190, data in Sponsor’s file Yankelovich 4. P&G MRD #US972782, data in Sponsor’s file 5. P&G MRD #US996633, data in Sponsor’s file 6. P&G MRD #US004463, data in Sponsor’s file 7. NHBA Mail Survey Feb-Mar 2000, data in Sponsor’s file 8. P&G MRD #US011624, data in Sponsor’s file 9. American Gastroenterological Association and the Gallup Organization, Inc. A Gallup survey on heartburn across America, Princeton, NJ: 1988, 2000 10. AC Nielson/SmithKline Beecham Survey. Prog Groc. 1995;74(9):98-99 Heartburn: Frequency Frequency of Heartburn in the US Population (1997)1 (Days per Week) 1. P&G MRD #US972782. Data in Sponsor’s file. What is Episodic Heartburn? Heartburn that occurs < 2 times weekly What Is Frequent Heartburn? Frequent heartburn (FHB) is described as “heartburn occurring 2 or more days per week.” What is GERD? Heartburn is one symptom of GERD This is characterized by: Reflux of food and acid from stomach into esophagus Often associated with esophageal inflammation May be associated with mucosal injury or even cancer • Erosive esophagitis and/or Barrett’s Frequency of Heartburn Frequency and severity of heartburn does not necessarily correlate with development of esophageal damage or erosions Individuals with severe and frequent heartburn may have no esophageal damage whereas individuals with little heartburn may have significant damage Therefore…response to standard OTC medications by the patient is likely to be a predictor of more serious or less serious pathology Symptoms of GERD Burning, substernal pain Radiates up into the throat Acid taste in mouth Chest pain Nausea Hoarseness of voice Wheezing Cough Dysphagia EE (Continued) Most likely diagnosis is: GERD Consider cardiac etiology given age; Negative nuclear stress test Etiology of Heartburn and GERD Heartburn and GERD occurs when: The lower esophageal sphincter (LES) temporarily relaxes Allows reflux of stomach acid into the esophagus Normally, gravity and peristalsis clear material from the esophagus and the saliva that we swallow neutralizes the remaining esophageal acid Heartburn occurs when any one of these mechanisms are impaired Draft 17 Primary Cause of Heartburn and GERD ACID SIGNALS STOMACH LINING Cause of Lower Esophageal Sphincter Relaxation Relaxation or weakening of the LES can be caused by: • Eating certain foods Onions, garlic, black pepper • Pressure on the stomach because of an individual’s weight • Frequent bending and lifting, lifting particularly after eating • Vigorous exercise Cause of Lower Esophageal Sphincter Relaxation Relaxation or weakening of the LES can be caused by: • Pregnancy Progesterone relaxes LES; slows peristalsis and increases retention of partially digested food and acid • Medications also can decrease LES pressure p CCB’s, hormone replacement therapy, muscle relaxants, beta blockers Alpha-blockers Nitrates • Pathophysiologic mechanisms Hiatal hernia and gastric acid hypersecretion Zenker’s diverticulum Etiology Several other defects thought to contribute to heartburn and GERD Abnormal esophageal epithelial resistance Abnormalities of gastric emptying Gastric G t i distention di t ti Abnormal acid production Causes of Heartburn and GERD www.heartburnalliance.com Aggravating Conditions/Factors Large meals Stress Lying down after eating Caffeine Acidic foods/juices Alcohol Tight clothing Mint/chocolate Exercise after eating Obesity Helicobacter pylori (controversial) Physical Examination Findings None Asthma Wheezing Cough Hoarseness of voice Epigastric/sub-xyphoid tenderness Diagnosis of Heartburn Diagnosis of heartburn is usually made with history and physical examination Usually, Usually this is all that is needed Many clinicians will try routine treatments first and assess for response prior to ordering a variety of tests Diagnosis Multiple tests available to make this diagnosis Often times, patient is treated with medication 1st to see how he/she responds If inadequate i d t response, testing t ti performed f d or…ifif any worrisome signs present • UGI: easiest, least expensive test Hiatal hernia: present in 40-60% of population Mild reflux seen in 30% of general population Looking for esophageal irregularities, ulcers Normal barium swallow may be seen in 40-60% of all individuals with GERD Endoscopy Endoscopy (Esophagoscopy) Best study for the evaluation and treatment of GERD Allows for direct visualization of the mucosa of the esophagus and the lining of the stomach Essential when suspecting Barrett’s esophagitis If abnormalities are seen, biopsy is conducted Intraesophageal Acid Perfusion Also called Bernstein test This is a test where the patients symptoms are reproduced or eliminated with this procedure NG ttube be placed 30 30-35 35 cm from the tip of the nares into the esophagus Saline is infused followed by HCL Looking for reproduction of symptoms with HCL and relief of symptoms with saline infusion 24-hour pH Monitoring 2 mm flexible probe is placed transnasally to about 5 cm above the LES Probe is connected to a box similar to a Holter monitor Patient then returns home and eats a normal diet Monitoring of pH is conducted in addition to the patients symptoms Esophageal Motility Studies Conducted to measure the pressure of the LES Thin, pressure sensitive tube is passed through mouth or nose and into stomach Once in place, the tube is pulled back slowly into the esophagus while the patient is asked to swallow The pressure of the muscle contractions is then measured along several sections of the tube H. Pylori Role of H. pylori in heartburn is subject of frequent debate H. pylori – water supplies First identified in countries where water supply is poor p Transmitted via saliva Bacteria may help erode protective layer of esophagus H. pylori breath test – most accurate test to be performed in primary care Biopsy – gold standard H. Pylori Breath Test Sensitivity: 96.5% Specificity: 96% Consequences of GERD Most cases managed in primary care setting 10% - 15% of individuals with GERD will develop complications Barrett’s esophagitis Carcinoma of the esophagus Hemorrhage Achalasia: absence of esophageal peristalsis and failure of lower esophageal sphincter (dysphagia) Esophageal constrictions Asthma Pulmonary Fibrosis Barrett’s Esophagitis Occurs in < 1% of heartburn sufferers Occurs when the esophageal lining is replaced by tissue normally found in the intestines (metaplasia) Increased risk of adenocarcinoma of the esophagus 30 – 125 times higher in the patient with Barrett’s The Good News IS… 53 – 71% of all heartburn sufferers have endoscopically normal esophageal mucosa Treatments Lifestyle Modification Elimination of medications Antacids If no improvement p in 2 weeks,, move to next group g p of medications H2 Antagonists If no improvement in 4-8 weeks, move to next group of medications PPI (Proton pump inhibitors) Surgery Red Flags Weight loss accompanied by heartburn Failure to respond to traditional treatment regimens Black or bloody stools Anemia Difficulty swallowing/choking after eating Hoarse voice Chest pain with radiation or accompanying sob and diaphoresis EE History and physical examination were consistent with GERD No additional testing performed Cardiac C di pathology th l ruled-out l d t No additional red flags Patient started on lifestyle modification and a proton pump inhibitor given frequency and severity of symptoms Treatment Options Goals for Treatment Because stomach acid is the main cause of heartburn and GERD, the goal is to mitigate its effects by: 1. Preventing the relaxation of the LES that allows stomach acid to reflux and/or 2. Reducing production of stomach acid, and/or 3. Neutralizing the acid AND…eliminating the patient’s symptoms Nonpharmacologic Treatment Options Dietary Modification Bland diet Smaller meals Less acidic foods Avoidance of chocolate/mint Nonpharmacologic Treatment Options Dietary Modification Avoidance of alcohol Decrease fat in diet Weight loss Lifestyle changes • Elevate head of bed M di ti Medications Medication Habits and Practices of the Frequent Heartburn Population More than 86% of frequent heartburn sufferers report using over-the-counter (OTC) medications 1 80% use antacids 48% use OTC H2 receptor antagonists 47% medicate > 2 days in a row 55% take medication for heartburn prevention 58% have spoken with a healthcare provider about heartburn 34% use a prescription medication to manage heartburn 1. P&G MRD#US972782. Data in Sponsor’s file 2. P&G MRD Number US 011624. Data in Sponsor’s file. Medication Habits and Practices of the Frequent Heartburn Population Volume of OTC Heartburn Product Use by Frequency of Heartburn (All OTC Users Past 12 Months) Consumers who experience frequent heartburn account for the majority of OTC heartburn product usage. Yet… 81% of heartburn sufferers are not completely satisfied with heartburn medication and the relief it affords them6 6. P&G MRD#US004463 Antacids Antacids Examples: Maalox • Aluminum hydroxide, magnesium hydroxide Mylanta • Same as above Rolaids • Calcium carbonate, magnesium hydroxide Surpass • Calcium carbonate Tums • Calcium carbonate Antacids Although antacids have long been thought to work in the gastric lumen to decrease gastric acidity, they actually work in the esophageal lumen Rapidly R idl increase i esophageal h l pH H Neutralize esophageal acid for 90 minutes after dosing Little change in gastric pH Indication: intermittent or episodic heartburn Antacids Advantages Multiple products available Many different preparations: liquid, swallowable tablets, chewable tablets, effervescent solutions and gum Gum and chewed tablet antacids seem to be more effective (per patients) than liquid products Fast onset of action Ease of dosing – take when patient has symptoms Disadvantages of Antacids Frequent dosing required Short duration of action Few studies done with antacids No role with prevention H2RA’s H2RA’ H2RA’s Axid 75 mg nizatidine Pepcid AC 10 mg famotidine Maximum Strength Pepcid AC 20 mg famotidine Pepcid Complete 10 mg famotidine, 800 mg of CaCO3 (Tums) and 165 mg of MG (OH)2 Tagamet HB 200 mg cimetidine Zantac 75/150 75 mg ranitidine Mechanism of Action Drugs bind to histamine-2 receptors on parietal cells to decrease gastric acid secretion Begin to work by decreasing gastric acid secretion within 1 – 2 hours of dosing Seem to work best on nocturnal acid secretion vs. daytime (i.e. after meal secretion) Antacids vs. H2RA Antacids: Onset: 30 minutes, Last: 60 minutes H2RA: Onset: 90 minutes, Last: 9 hours H2RA’s Numerous studies conducted at both OTC and prescription strength dosages Clearly surpass placebo in onset of action and sustained efficacy H2RA’s Indication: episodic heartburn All products can be taken daily Not indicated for frequent heartburn Combination of Antacid and H2RA Low Dose H2RA and Antacid H2RA and antacid combination Speed of an antacid + duration of H2RA Indication: I di ti intermittent i t itt t or episodic i di heartburn Not cost effective or indicated for individuals with frequent heartburn Proton Pump Inhibitors Mechanism of Action PPIs Suppress gastric acid production by blocking parietal cell hydrogen/potassium ion adenosine triphosphatase Known as the proton pump This is the final pathway involved in acid secretion Remember…PPI’s affect only those pumps which are active • Not all pumps are active at the same time 25% of new proton pumps are synthesized daily Draft 60 Mechanism of Action: Proton Pump Inhibitor Proton Pump Inhibitors Omeprazole (Prilosec) Lansoprazole (Prevacid) Esomeprazole (Nexium) Rabeprazole (AcipHex) Pantoprazole (Protonix) Indications Prilosec OTC Frequent heartburn Prescription PPI’s GERD Reduce risk of NSAID induced gastric ulceration Erosive Esophagitis Hypersecretory conditions • Zollinger-Ellison Syndrome Proton Pump Inhibitors Recent studies have shown an increased risk of: Osteoporosis • Should take calcium citrate NOT carbonate • Carbonate – i.e. Tums needs an acidic environment Pneumonia • Diminished acid protection Combination Therapy Zegerid Capsules Omeprazole Sodium bicarbonate Indications I di ti • Gastric and duodenal ulcer • Erosive esophagitis • Symptomatic GERD Surgical Options Nissen fundoplication The upper curve of the stomach (the fundus) is wrapped around the esophagus and sewn into place so that the lower portion of the esophagus passes through a small tunnel of stomach muscle This surgery strengthens the LES between the esophagus and stomach In one study, 62% of people who had surgery were still taking medications to control GERD symptoms. • However, they were less likely to need to take medications regularly; and, when they did not take medications, their remaining symptoms were likely to be less severe. Additional Surgical Option EsophyX Transoral Incisionless Fundoplication Treatment of GERD • Reconstruction of the antireflux barrier • Restores GE junction back to normal anatomy • Same concept as the Nissen without incisions • Now FDA approved and cleared for US market EE Patient returns 1 month after initiating treatment with a PPI; no improvement in symptoms Referred for endoscopy given lack of response to traditional methods Endoscopy shows mild esophagitis; negative biopsy PPI – increased by GI to 2 daily No improvement at 1 month What Now?? 24 hour pH probe Esophageal motility studies Bernstein test EE 24 hour probe shows NO significant correlation between pH and symptoms Esophageal motility studies showed decreased motility Started on metoclopramide (reglan) 5 mg 1 po tid – 30 minutes prior to meals with significant improvement in symptoms Web Site Resources www.heartburnalliance.org www.myheartburn.org Thank You! I Would Be Happy to Entertain Any Questions Wendy L. Wright, MS, RN, ARNP, FNP 2 Rolling Woods Drive Bedford New Hampshire Bedford, Cell: 603-490-0154 email: [email protected]