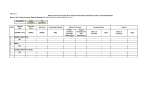
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
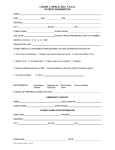
New Patient Details Dr Charlotte Mooring abides by the Privacy Act 1988. Information supplied by you is kept strictly private and confidential and will assist in providing the best possible care. Please complete ALL sections. Your Details: ! Last Name: _____________________ First Names: ____________________________! Preferred Name: __________________________! Title: _______ Maiden Name: _______________________ Address: _____________________________________________________________________________________________ DOB: ____________________________! Home Phone: _________________________ Mobile: ____________________________! Work Phone: _________________________ Email: ____________________________! Occupation: __________________________ Partner’s Name: ____________________________! Partner’s Mobile: __________________________ Emergency Contact: (Name & Number) ______________________________________________________________________________________ Health Insurance Details: Medicare: _____________________ Ref _______! Expiry: __________________________ Private Health Fund: __________________________! Membership No: __________________ Referring Doctor Details: Referring Doctor: _____________________________! How did you hear about our Practice? ! Your Medical Details: Usual GP: _______________________ _________________________________________________________ (Please complete ALL sections. Ask for help if required.) Please list any medical problems or conditions (NIL)! Please list all Medications you are taking (NIL) ___________________________________________! _____________________________________ ___________________________________________! _____________________________________ Please list all past Surgery (NIL)! ! ___________________________________________! Are you allergic to any medication (YES/NO) If YES please specify _____________________________________ ___________________________________________! _____________________________________ Please list all past pregnancies (NIL)! ! ___________________________________________! Do you smoke cigarettes? (YES/NO) Do you drink alcohol? (YES/NO) ___________________________________________! When was your last Pap Smear? ________________ Tests: Have you had blood tests relevant to your condition?! (YES/NO) QML S&N Other ____________________________________________________________________________ Have you had scans relevant to your condition? (YES/NO) Where? _____________________________________________ Family History: In your family is there any history of: Is there any history of congenital abnormalities in either your family or your partner’s family?! Bleeding or Clotting Disorders? (YES/NO)! (YES/NO) Anaesthetic Complications? (YES/NO) I understand that payment of my account, in full, is my responsibility and that my health fund might not cover the total amount invoiced. I am responsible for any further costs that might be incurred resulting from my not paying my account, in full by the due date. Signature: ––––––––––––––––––––––––––––––! Date: __________________ Consent for the collection and release of medical information: In order to provide optimal care, it may be necessary at times to discuss your case with other health professionals. Your privacy will be respected at all times. By signing below you are giving consent for the collection of any relevant information pertaining to your care. Patient Name: _____________________________________________ ! Signature: _____________________________________________! Date of Birth: ______________ Date: ______________