Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
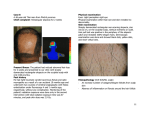
CASE REPORT Radiation- and Chemotherapy-Induced Permanent Alopecia: Case Series Mansoor Haider, Issam Hamadah, and Abdulmonem Almutawa Background: Radiation- and chemotherapy-induced alopecia is mostly temporary. However, permanent scalp alopecia is reported, albeit infrequently. Objective: The objective of this observational case series was to determine the kind and doses of chemotherapeutic agents and radiation in inducing permanent alopecia of the scalp. Methods and Results: Eleven patients referred to our department over a period of 3 years for permanent alopecia after chemotherapy/radiotherapy or combination therapy were included. A detailed medical and therapeutic history was obtained from each patient and from medical records. Photography was done, and the scalp biopsies were taken. Patients were divided into three groups according to the type of therapy. The first group received conditioning chemotherapy prior to bone marrow transplantation. The second group had radiation for brain tumors, and the third group received both. Conclusion: A comprehensive multicenter and multidisciplinary study is required to determine the definite causative agents, doses, and other cofactors that induce permanent alopecia following chemotherapy/radiotherapy, as well as the means to avoid this distressing outcome in surviving patients. Contexte: L'alopécie causée par la chimiothérapie et la radiothérapie est, la plupart du temps, temporaire, mais il arrive, dans de rares cas, que le traitement donne lieu à une calvitie permanente. Objectif: La présente série de cas d'observation visait à déterminer le type et la posologie des agents chimiothérapeutiques ainsi que le type et les doses de rayonnement, incriminés dans la calvitie permanente. Méthode et résultats: Ont participé à l'étude 11 patients dirigés vers notre service, sur une période de 3 ans, pour une calvitie permanente, consécutive à la chimiothérapie ou à la radiothérapie, administrées seules ou en association. Une anamnèse détaillée sur les antécédents médicaux et les interventions thérapeutiques a été fournie par chacun des patients et tirée des dossiers médicaux. Des photographies ont été prises, et nous avons effectué des biopsies du cuir chevelu. Les sujets ont été divisés en trois groupes selon le type de traitement reçu: (1) la chimiothérapie préparatoire à la greffe de moelle osseuse; (21 la radiothérapie pour des tumeurs cérébrales; et (3) la chimiothérapie et la radiothérapie en association. Conclusions: II est nécessaire de mener une étude approfondie, multicentrique, et pluridisciplinaire afin, d'une part, de déterminer précisément les agents, les doses, et d'autres cofacteurs incriminés dans la calvitie permanente, consécutive à la chimiothérapie ou à la radiothérapie, et, d'autre part, de trouver des moyens d'éviter cet effet indésirable pénible chez les patients ayant survécu à la maladie. T EMPORARY ALOPECIA resulting from chemotherapy/radiotherapy is a well-known side effect. However, permanent loss of scalp hair may also result from radiotherapy for brain tumors or metastasis as well as certain chemotherapeutic agents, in particular those used for conditioning prior to bone marrow transplantation From the Departments of Dermatology and Pathology and Laboratory Medicine, King Faisal Specialist Hospital and Research Centre, Riyadh, Saudi Arabia. Address reprint requests to: Mansoor Haider, MBBS, FCPS(Dermatology), Department of Dermatology, King Faisal Specialist Hospital and Research Centre, MBC 46-1, PO Box 3354, Riyadh 11211, Saudi Arabia; e-mail: [email protected]. DOI 10.2310/7750.2012.12033 C: 2013 Canadian Dermatology Association (BMT). In the medical literature, such reports are no longer rare, but why some patients develop permanent loss of hair and others do not and what the common mechanism is between chemotherapy and radiotherapy that results in this condition need to be investigated thoroughly. The following case series consisted of 11 patients who reported to the Department of Dermatology at the King Faisal Specialist Hospital and Research Centre in Riyadh, Saudi Arabia, for permanent loss of scalp hair following either radiotherapy or chemotherapy alone or in combination. Methods and Results This observational study includes 11 patients referred to us over a period of 3 years for permanent loss of scalp hair after radiotherapy, chemotherapy, or both. The female to male DECKEI^ journal of Cutaneous Medicine and Surgery, Vol 17, No I (January/February), 2013: pp 55-61 55 56 Haider et al Table 1. Chemotherapy-Induced Alopecia Patient No. Sex Age When Received Therapy Diagnosis 1 F 2yr Congenital amegakaryocytic thrombocytopenia 2 F 14 yr Acute myeloid leukemia 3 M 17 yr Chronic myeloid leukemia 4 F 2yr Chronic granulomatous disease Conditioning Regimen Busulfan 4 mg/kg daily X 4 d Cyclophosphamide IV 590 mg daily X 4 d Busulfan 4 mg/kg daily X 4 d Cyclophosphamide IV 2,400 mg daily X 2 d Busulfan 4 mg/kg daily X 4 d Cyclophosphamide IV 60 mg/kg daily X 4 d Busulfan 4 mg/kg daily X 4 d Cyclophosphamide IV 60 mg/kg daily X 4 d Other Medications in Addition to Conditioning Regimen Pattern and Site of Alopecia After BMT: MTX, cyclosporine, acyclovir. fluconazole, piperacillintazobactam, gentamicin Frontal and parietal Induction chemotherapy before BMT: idarubicin. cytarabine, etoposide Diffuse Treatment before conditioning: hydroxyurea 1-2.0 g daily X 8 mo; allopurinol After BMT: MTX, cyclosporine, trimethoprimsulfamethoxazole. fluconazole, acyclovir After BMT: MTX, cyclosporine, trimethoprimsulfamethoxazole Moth eaten Diffuse BMT = bone marrow transplantation; MTX = methotrexate. ratio was 10:1. The patients' ages at the time of presentation to the dermatology clinic ranged from 6 to 30 years, but the age at which they received treatment ranged from 2 to 20 years. Four patients received chemotherapy alone (group 1), three patients received radiotherapy (group 2), and four patients received both (group 3). All patients were photographed at the time of presentation, and scalp biopsies were taken in nine patients (two declined). Table 2. Radiotherapy-Induced Alopecia Sex Age When Received Therapy 5 F 15 yr 6 F 20 yr 7 F 12 yr Patient No. Diagnosis Ganglioglioma (post erior cranial fossa) Pineal ependymoma (secondary tumors in brain from spinal tumor) MeduUoblastoma (post erior cranial fossa) Radiation Type Beam Energy Total Dose No. of Fractions Site of Alopecia X-rays 6MV 5,040 cGy 28 X-rays 6 MV right lateral 6 MV left lateral whole brain 6 MV dorsal spine 6 MV for craniospinal axis 18 MV for post erior cranial fossa boost 3,000 cGy 10 Occipitoparietal region Frontoparietal and bitemporal region 30 20 Vertex and occipital region X-rays 3,000 cGy 5,400 cGy i 3,600 (craniospinal) + 1,800 (post erior cranial fossa) -1- 10 57 Radiation- and Chemotherapy-Induced Permanent Alopecia I O o o. ex E *a 3 o o a „ o 2 .a g. T3 u G u « :3 O + c + > ° > > § > E cd CN g ri 00 ^ O > D. O O 'S t °°' C TO " L> ._ « ^ '^.. ^ E s tu J3 .-^ c ^ OJ 0 '¡—! CO O 0 •5 'S °°' > O 0 E E -- J. ° ^ (n ^ -r E " 2 incr cycl E al CL. vin -ist + «I + Ö0 -o ° s cd 00 " E g- oj - .a ~ 00 8 J3 2 Ln o CN OJ c O -C eu E 'E 00 o "^ U5 n ^ .ï3 -S "J .Í2 > Ln V E ^2 o o .2 •§ ^ o. cd E >^ . ^ 3 Ë g s (^ I^ Cl. r^ rt ï2 .E" Lo . . c d '-' O - a x> g .2 " a| '^ s tu (N -tí u t o o o -O C < s: o 3 Q. _O cd =3 -fi ;>_^ ' o o .t:: L-cd OJ =3 Q^ 3o C «J c O X X M •a I •y} (d O c o 00 u 3 (D E U p.. <U o s Ë "0 3 0 0 ^0 BSS Diae u Cd SiSO moth rapy- 3 -O C s * I I 2 :i b astom 1 f!^ > edu •2 ^ O <u > ^ z s > -^ 'S ramai CL) ! c 'cd cd _û .E '^ -B 00 > -a c rai c "SS ^ 1 .s« a E 3 «S ^ ^ ^ •B • !" g I ^ eu G s :s o ^H a 5 in '•S H ° S cQ t; o o o o (N pi :3 "t- 'u c aï" - — o .E g 58 Haider et al Croup 1 received busulfan and cyclophosphamide as a conditioning regimen before BMT. The age at the time of receiving therapy ranged from 2 to 17 years. In addition to conditioning therapy, other medications were given either before or affer transplantation. Three different patterns of alopecia were observed (Table 1). Croup 2, aged 12 to 20 years at the time of therapy, received radiation for brain tumors. Total doses given ranged from 3,000 to 5,400 cCy in 10 to 30 ffactions (Table 2). One patient (7) received radiation affer resection of the tumor. In the other two patients, resection could not be performed due to location. In the foUowing 2 to 6 months, progressive hair loss was noticed at the sites of radiation in all patients. Croup 3 comprised four patients suffering ffom meduUoblastoma, astrocytoma, and neuroblastoma. The first three received radiation foUowed by chemotherapy over a period of 10 to 12 months (Table 3). In patients 8 and 9, partial resection of the tumor was performed due to involvement of the floor of the fourth ventricle. In patient 10, the tumor was unresectable due to location. Patient 11 first underwent induction chemotherapy for neuroblastoma grade IV (four cycles in 3 months) foUowed by surgical removal and total body irradiation and then conditioning with carboplatin, etoposide, and melphalan prior to autologous BMT (see Table 3). AU patients developed alopecia during radiotherapy, with only partial recovery in subsequent months. Scalp biopsies were transversely sectioned in seven cases and vertically in two cases. SimUar changes were observed in all nine biopsies. There was a reduction in foUicular densities and some degree of variation in foUicular size, as well as significant miniaturization (Figure 1). None of the biopsies revealed scarring, peribulbar infiammation, interface dermatitis, or graff-versus-host disease (CVHD). Our patients were foUowed up for 2 years. Topical minoxidil 2 to 5% was prescribed. Some patients used it for 3 months to 1 year but then discontinued due to a lack of response. Discussion Hair loss, temporary or permanent, is one of the most stressful side effects for patients undergoing oncologic treatment. The true prevalence of permanent alopecia by chemotherapy or radiation may be underestimated as many patients do not complain and accept it as the price of treatment. Postchemotherapy Alopecia In general, alopecia affer chemotherapy is temporary, with regrowth expected within 4 to 6 weeks. However, irreversible alopecia has been reported in the last two decades with various therapeutic agents, in particular, busulfan-cyclophosphamide combination therapy (BUCY), as a conditioning regimen prior to BMT.'"^ Permanent alopecia is defined as complete loss of growth or partial regrowth at least 6 months affer chemotherapy.* Increased risk factors for permanent alopecia in transplant patients are treatment with busulfan, chronic CVHD, and previous cranial irradiation.'' Civen that scalp hairs are one of the most rapidly growing hairs in the body, they are the most commonly affected. However, other body sites may also be involved, including eyebrows, eyelashes, and axillary and pubic hair. The exact mechanism of chemotherapy-induced permanent alopecia (CIPAL) is stiU unknown. Possible explanations are stem ceU destruction or acute damage of matrix keratinocytes that die in the hypodermis instead of entering the catagen phase' or permanent toxic damage to the hair foUicle stem ceUs in their bulge (at the insertion of arrector pili muscle).^ The p53 protein is found to be essential for this chemotherapy-induced alopecia as it mediates apoptosis and growth arrest in TP53-negeiúve cancers.^ However, not aU patients receiving chemotherapy develop CIPAL. In a retrospective study by Machado and coUeagues, only 6 of 760 patients developed irreversible hair loss affer high-dose chemotherapy.* Baker and coUeagues described 6 Figure 1. A, Transverse section at the level of the upper dermis (isthmus) showing reduced foUicular density and some variation in foUicular size (hematoxylin-eosin stain; X40 original magnification). B, Miniaturized follicles (hematoxylin-eosin stain; X200 original magnification). Radiation- and Chemotherapy-Induced Permanent Alopecia patients with incomplete regrowth of varying severity among 22 who had undergone allogenic or autologous BMT and had BUGY conditioning.' Similarly, Ljungman and colleagues studied 65 patients who received busulfan prior to BMT and found some degree of permanent alopecia in 31 cases.^ Why some patients develop permanent rather than temporary alopecia following chemotherapy is still unanswered. Serum busulfan concentration can be a factor. Pharmacokinetic variability as a result of the bioavailability of oral busulfan may be contributing to this.*^ In their study, Ljungman and colleagues found extensive permanent alopecia in patients with high busulfan concentration." Although there is no current effective therapy for GIPAL, one possible solution is to reduce the dose. However, a mean plasma concentration below the median level during conditioning can significantly increase the risk of relapse.'* Other suggested options include scalp hypothermia"" and topical anti-p53 treatment." Drugs other than busulfan reported to cause permanent hair loss are docetaxel,'*'^^ carboplatin, thiotepa,'' and tamoxifen.''' All four patients in group 1 received BUGY conditioning therapy in standard doses before BMT. None of them suffered from acute or chronic GVHD. All developed permanent hair loss but with variable patterns (Figure 2), the explanation of which may be that cytotoxic drugs damage actively proliferating foUicular cells in an apoptosisrelated manner, rendering the hair follicle cells vulnerable depending on their state of proliferation.'^ Postradiotherapy Alopecia Permanent alopecia is a well-known side effect of radiation. Although the principal change following an acute dose of radiation is apoptosis,'' radiation damage 59 can occur due to a combination of changes such as a reduction in matrix cell reproduction, the effect on protein synthesis/plasma membrane permeability of matrix cells, and alteration in perifollicular blood flow.'^ Temporary alopecia following radiotherapy occurs in 2 to 3 weeks and resolves within 2 to 3 months afier completion of radiotherapy. Doses as low as 2 Gy in a single fraction can cause temporary anagen alopecia.'^ Telogen alopecia takes more time to occur compared to anagen alopecia and needs higher doses than anagen (two to three times) but stores radiation damage for long periods.'^ The doses reported to cause permanent hair loss vary widely. A study conducted by Shakespeare and colleagues documented that at a dose of 36 Gy the estimated median risk of permanent alopecia was 5% and that a dose of 45 Gy resulted in a risk of 15%.''^ FoUicular dose (the dose of radiation at the level of hair follicle in a particular radiation field) is the only significant factor in determining the degree of permanent alopecia.'^''* Most anagen follicles are at a depth of 4 to 4.5 mm from the skin surface. If the radiation superficial to this depth is kept under a lethal dose, the incidence of radiation-induced alopecia can be markedly reduced.'" The D50, the follicular dose at which 50% of patients develop permanent alopecia, is estimated to be 43 Gy.'^ Follicular dose in turn depends on beam energy, field position and size, and method of radiation. For patients treated with opposed lateralfields,the follicular dose is usually the highest at the anterior-superior and/or posterior region of the skuU where two lateral fields overlap. Use of stereotactic arcs minimizes the foUicular dose as arcs typicaUy do not overlap. Similarly, higher beam energies have skin-sparing properties.'** Other methods or materials used in animal models/humans for radiation protection include nitroxide^' and prostaglandin E2.^^ In our three patients who received Figure 2. Patterns of chemotherapyinduced permanent alopecia. 60 Haider et al Figure 3. Patterns of radiationinduced permanent alopecia. radiotherapy alone for the brain tumors, the total dose ranged from 30 to 54 Gy in 10 to 30fractions(see Table 2). The sites of alopecia varied according to the field of radiation (Figure 3). Post-Chemotherapy/Radiotherapy Alopecia The third group comprised patients who received combined radiotherapy and chemotherapy. Three patients (8, 9, 10) were treated with lateral opposed fields, whereas patient 11 had total body irradiation. The total dose ranged from 12 to 54 Gy. Among chemotherapeutic agents, vincristine, cyclophosphamide, carmustine, and carboplatin were given over a period of 9 to 12 months in the first three patients. In patients 8 and 9, weekly intravenous vincristine was administered during radiation and adjuvant chemotherapy for children with the medulloblastoma protocol was started 1 month after stopping radiotherapy. Inpatient 10, chemotherapy was also started 1 month after stopping radiotherapy. Patient 11 received induction chemotherapy prior to surgical resection of tumor, followed by radiotherapy and conditioning with carboplatin, etoposide, and melphalan (see Table 3). Loss of hair was noticed soon after radiotherapy in all patients, and hair was only partially replaced in the following months (Figure 4). VLncristine has no documented association with alopecia. Cyclophosphamide causes only temporary alopecia. Carboplatin and cyclophosphamide, the only drugs that enhance radiosensitization,"*'"^ were administered after completion of radiation in the first three cases and thus were Figure 4. Patterns of combined radiotherapy/chemotiierapy-induced permanent alopecia. Radiation- and Chemotherapy-Induced Permanent Alopecia unlikely to be a contributing factor in inducing permanent alopecia. Even in the study done by Lawenda and colleagues, no statistically significant difference was found in D50 among patients who received radiosensitization chemotherapy agents and those who received agents without this property.'^ In a review article by Malkinson and Keane, the authors explained that the adjuvant effects of chemotherapy/drugs are related to the interval between the drug administered and radiation given.'* This enhancing effect was observed when radiation was given hours after chemotherapy, which in turn depends on the phase of cell cycle in which activity was arrested. Moreover, no changes were observed when the sequence of radiation and drug was reversed and metabolic activity failed to influence radiation changes at higher doses. In patient 11, cyclophosphamide was administered before radiotherapy, but the intei"val between them was over weeks rather than hours. So in this group, radiotherapy was considered to be the cause of permanent loss of hair, and chemotherapy was most likely not involved. Conclusion Ghemotherapy/radiotherapy-induced permanent alopecia is a distressing condition that must be addressed at multicenter levels to determine the exact prevalence among populations undergoing these types of therapies and possible ways and means to minimize its occurrence. Acknowledgments We thank Marieta P. Ricardo for typing and uploading the manuscript. Financial disclosure of authors and reviewers: None reported. References 1. Tosti A, Piraccini BM, Vincenzi C, Misciali C. Permanent alopecia after busulfan chemotherapy. Br J Dermatol 2005;152:1056-8, doi: 10.11 ll/).1365-2133.2005.06469.x. 2. Tran D, Sinclair RD, Schwarer AP, Chow CW. Permanent alopecia following chemotherapy and bone marrow transplantation. Australas J Dermatol 2000;41:106-8, doi:10.1046/i.l440-0960.2000.00405.x. 3. Ljungman P, Hassan M, Bekassy AN, et al. Busulphan concentration in relation to permanent alopecia in recipients of bone marrow transplants. Bone Marrow Transplant 1995; 15:869-71. 4. Slattery JT, Clift RA, Buckner CD, et al. Marrow transplantation for chronic myeloid leukemia: the influence of plasma busulfan levels on the outcome of transplantation. Blood 1997;89:3055-60. 5. Baker BW, Wilson CL, Davis AL, et al Bustolphan/cyclophosphamide conditioning for bone marrow transplantation may lead to failure of hair regrowth. Bone Marrow Transplant 1991;7:43-7. 61 6. Machado M, Moreb JS, Khan SA. Six cases of permanent alopecia after various conditioning regimens commonly used in hematopoietic stem cell transplantation. Bone Marrow Transplant 2007; 40:979-82, doi: 10.1038/sj.bmt. 1705817. 7. Vowels M, Chan LL, Giri N, et al. Factors affecting hair regrovrth after bone marrow transplantation. Bone Marrow Transplant 1993; 12:347-50. 8. Botchkarev VA, Komarova EA, Siebenhaar F, et al. p53 is essential for chemotherapy induced hair loss. Gancer Res 2000;60:5002-6. 9. Hassan M, Ljungman P, Bolme P, et al. Busulfan bioavailability. Blood 1994;84:2144-50. 10. Breed WPM, Vanden Hurk GJG, Peerbooms M. Presentation, impact and prevention of chemotherapy-induced hair loss: scalp cooling potentials and limitations. Exper Rev Dermatol 2011;6: 109-25, doi:10.1586/edm.l0.76. 11. Talion B, Blanchard E, Goldberg LJ. Permanent chemotherapyinduced alopecia: case report and review of the literature. J Am Acad Dermatol 2010;63:333-6, doi:10.1016/¡.iaad.2009.06.063. 12. Prevezas C, Matard B, Prinquier L, Reygagne P. Irreversible and severe alopecia following docetaxel or paclitaxel cytotoxic therapy for breast cancer. Br J Dermatol 2009; 160:883-5, doi:10.1111/ ¡.1365-2133.2009.09043.X. 13. de Jong ME, Mathot RAA, Dalesio O, et al. Relationship between irreversible alopecia and exposure to cyclophosphamide, thiotepa and carboplatin (CTC) in high-dose chemotherapy. Bone Marrow Transplant 2002;30:593-7, doi:10.1038/si.bmt.l703695. 14. Puglisi F, Aprile G, Sobrero A. Tamoxifen- induced total alopecia. Ann Intern Med 2001;134:1154-5. 15. Hamüton CS, Potten CS, Denham JW, et al. Response of human hair cortical cells to ftactionated radiotherapy. Radiother Oncol 1997;43:289-92, doi:10.1016/S0167-8140(97)00059-5. 16. Malkinson FD, Keane JT. Radiobiology of the skin: review of some effects on epidermis and hair. J Invest Dermatol 1981;77:133-8, doi:10.1111/1523-1747.epl2479347. 17. Shakespeare TP, Dwyer M, Mukherjee R, et al. Estimating risks of radiotherapy complications as part of informed consent: the high degree of variability between radiation oncologists may be related to experience. Int J Radiât Oncol Biol Phys 2002;54:647-53, doi:10.1016/S0360-3016(02)02996-6. 18. Lawenda BD, Gagne HM, Gierga DP, et al. Permanent alopecia after cranial irradiation: dose-response relationship. Int J Radiât Oncol Biol Phys 2004;60:879-87, doi:10.1016/i.ijrobp.2004.04.031. 19. Ginot A, Doyen J, Hannoun-Levi JM, Courdi A. Normal tissue tolerance to external beam radiation therapy: skin. Gancer Radiother 2010;14:379-85, doi:10.1016/j.canrad.2010.03.015. 20. Severs GA, Griffen T, Werner-Wasik M. Gicatricial alopecia secondary to radiation therapy: case report and review of the literature. Gutis 2008;81:147-53. 21. Metz JM, Smith D, Mick R, et al. A phase 1 study of topical Tempol for the prevention of alopecia induced by whole brain radiotherapy. Glin Gancer Res 2004;10:6411-7, doi: 10.1158/1078-0432.CGR-04-0658. 22. Malkinson FD, Geng L, Hanson WR. Prostaglandins protect against murine hair injury produced by ionizing radiation or doxorubicin. J Invest Dermatol 1993;101(l Suppl):135S-7S, doi: 10.111 l/1523-1747.epl2363200. 23. Susser WS, Whitaker-Worth DL, Grant-Kels JM. Mucocutaneous reactions to chemotherapy. J Am Acad Dermatol 1999;40:367^00, doi:10.1016/S0190-9622(99)70488-3. Copyright of Journal of Cutaneous Medicine & Surgery is the property of Decker Publishing and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.