Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
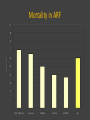
Acute Renal Failure (AKI) Abrupt onset of reduction in kidney function (6-12 weeks) • usually detected by laboratory evaluation serum creatinine rise >0.5 g/dl, GFR reduction >50% • associated with – oliguria (<400 ml urine/day) – significant morbidity and mortality • Incidence – 2-5% of hospitalised pts – 2- 25% of ICU pts RIFLE Criteria for Acute Renal Dysfunction Risk GFR creatinine x 1.5 or GFR > 25% Urine Output UO < 0.5ml/kg/h x 6 hr Mortality risk 2.4 Injury creatinine x2 or GFR > 50% UO < 0.5ml/kg/h x 12 hr 4.1 Failure creatinine x3 or GFR > 75% UO < 0.3ml/kg/h x 24 hr or Anuria x 12 hrs 6.3 Acute Kidney Injury Network criteria • abrupt (within 48 hours) increase in the serum creatinine of ≥ 0.3 mg/dL • percentage increase in the serum creatinine concentration of ≥ 50% • oliguria of less than 0.5 mL/kg per hour for more than six hours Medical and surgical admissions to ICU and factors contributing to AKI Mortality in ARF Risk factors for dying in patients with AKI 0.4 0.5 age (+10 yrs increment ) mechanical ventilation vasopressors/inotropes septic shock hematologic vs cardiovasc medical group 0.6 0.7 0.8 0.9 1 1.2 1.4 1.6 1.8 2.0 2.2 2.4 2.6 2.8 5,5 Risk factors Uchino, S. et al. JAMA 2005;294:813-818 Prerenal ARF- pathophysiology Ischemic stimulus: decreased glomerular filtration pressure – afferent vessel dilation – efferent vessel constriction – net effect = increase filtration rate Autoregulatory mechanisms of kidney vasculature operate between systolic blood pressure 170 - 70 mm Hg Ischemia–reperfusion results in reversible or irreversible injury to the proximal tubular cell Male recipient –female kidney Resolving ATN Male recipient – Female kidney with ATN Female patient with minimal change - control Male recipient –male donor + control Extrarenal cells participate in the regeneration of renal injury in human ARF Gupta S, Verfaille C et al, Kidney Int 62 (4), 1285-1290, 2002. Clinical and cellular phases in ischemic ARF •BBM loss •Exfoliation •Tubular obstruction Cell injury hypoxia Microvascular injury •Obstruction •Inflammation •Coagulation Maintenance •Dedifferentiation •Migration •Proliferation •Redifferentiation •Repolarization Sutton et al Kidney Int 62:1539-1549,2002 Intrinsic renal disease 40-50% of all ARF involving one or more of 4 major anatomic parts of the kidney vasculature, interstitium, glomeruli, tubules most common cause: Acute Tubular Necrosis ischemia nephrotixic agents Renal function 5 yrs after AKI good Cause of AKI Henoch Schonlein purpura Tubulointerstinal nephritis Post-infectious nephritis ATN Diffuse proliferative lupus GN MPGN HUS/TTP bad Extracapillary GN Acute cortical necrosis Postrenal ARF Obstruction of urinary tract at any level occurs in: 5-10% of all ARF obstructive lesion in urinary bladder or below in patients with solitary functioning kidney - early stage filtration continues increasing ureteral and tubular pressure - prolonged obstruction vasoconstriction in afferent arterioles results in diminished blood flow, filtration, interstitial oedema Acute renal failure differentiation - urinalysis Intrinsic renal Prerenal Postrenal Dipstic Blood - - Dipstic Protein - - RBC - - WBC - - Casts - - Other Hyaline casts - Vasculitis, GN Interstitial ATN +++ +++ + + - +++ + + +++ - RBC and WBC casts WBC casts - Eosinophils Tubular cells Brown casts - Microscopy - ARF - clinical course Prerenal or postrenal azotemia Prompt diagnosis and treatment – fully reversible Intrinsic renal failure – prolonged course Most common - ATN - initial phase (usually not noticed) - maintenance phase (2-3 weeks) - recovery 50% of patients oliguric, 5-10% anuric mortality 50-60% of non-renal causes: sepsis, cardiovascular complications ARF – clinical manifestation Cardiovascular complications hypertension, oedema, pulmonary congestion, pericarditis Hematologic manifestations • anaemia – decreased production of erythropoetin, excessive blood loses, haemolysis, shortened RBC half-life • bleeding diathesis - impaired platelets aggregation, adhesion • impaired immunity- lymphopenia, chemotaxis defect, cellular immunity defect Neurologic symptoms disorientation, asterixis, seizures, coma, peripheral neuropathy GI tract symptoms: hiccups, nausea, vomiting, anorexia, ileus, bleeding Treatment of ARF eliminate or control underlying primary disease restore effective renal blood low eliminate obstruction of urine flow eliminate nephrotoxic agents Supportive treatment Renal replacement treatment Indications for dialysis in ARF • • • • • • Hyperkalemia Fluid overload Acidosis Uremic symptoms Pericarditis Poisoning with toxins eliminated by dialysis (methanol ethylene glycol) • Blood urea >140-200 mg/dl Supportive treatment, early beginning ATN prophylaxis • Careful evaluation of fluid status, cardiac output, nephrotoxins elimination • Special attention to patients with compromised renal blood flow or kidney function – – – – – – elderly heart failure kidney disease liver disease renal artery stenosis diabetes mellitus Prevention or reversal of ATN High dose furosemide, low dose dopamine, mannitol –data controversial –effective in maintaining diuresis –mortality unchanged Experimental therapies –ANF, EGF, antibodies to adhesion molecules –Free radicals scavengers –Calcium channel blockers Contrast nephropathy risk factors intra-arterial contrats administration Age >75 years Baseline creatinine cleareance <60ml/min/1.73m2 Coronary catheterization in an emergency setting Diabetes mellitus Congestive heart failure Peripheral vascular disease and Volume of administered contrast > 300 ml Prevention of Contrast Nephropathy The major preventive actions • Identification of high risk patients • Withdraw nephrotixic medications prior to planned procedure • Hydration with 0.45%/ 0.9% saline administered at a rate of 100 ml/hr beginning 12 hours before and continued 12 hours after angiography use LOCM or IOCM aditionally • oral acetylcysteine, 1200 mg twice daily the day before and on the day of administration of contrast ACR Committee on Drugs and Contrast Media 2010 ATN secondary to rhabdomyolysis • • • • • crush syndrome caused by medication (statins, zidovudine, ephedrine) alcohol abuse seizures insect bite baseline serum creatinine (≥1.7mg/dl and ≥1.5mg/dl) maximum CPK value predictive for AKI and sustained kidney failure AKI in oncology Prerenal , Post renal Renal ATN due to medication (cisplatin, ifosfamide, interleukin-2) or sepsis TTP/HUS after stem cell transplantation Infiltration of the renal parenchyma from cancer cells (leukemia, lymphoma, myeloma) Intratubular obstruction (cast nephropathy-multiple myeloma, tumor lysis syndrome, methotrexate) Tumor lysis syndrome high rate of tumor cell turnover tumor lysis syndrome uric acid nephropathy prevention • establishing a urine output > 3 to 5 L/24 hr • allopurinol • rasburicase* *recombinant urate oxidase, a nonhuman proteolytic enzyme oxidizing uric acid to allantoin AKI after cardiac surgery Risk factors • CKD, diabetes mellitus, congestive heart failure, age >70 years, cardiopulmonary bypass (with artificial perfusion) >3 hours Prevention • clonidine improved creatinine clearance and was associated with greater hemodynamic stability • atrial natriuretic peptide (ΑΝΡ) reduces the need for dialysis or the risk of death compared to placebo • furosemide increases urine output but it decreases GFR and the filtration fraction • dopamine doesn’t prevent AKI Potential consequences of late refferal to nefrologist • Missing potentially reversible non-ATN cause of AKI (example: RPGN) • Delayed diagnosis increased • Deayed treatment mortality • Increased risk of complications • Increased risk of ESRD Which is the best`method for RRT in the AKI setting? ARF simple 1 organ failure Alternate day dialysis ARF severe ARF MOF 2 organs failure 3 or more organs failure Kidney + shock or other organ Kidney + shock + other organ Daily dialysis Continuous dialysis Slow Extended Dialysis Which is the best method for RRT in the AKI setting? Hemodialysis CRRT PD Advantages effective (K/h) Commonly used Easy to use Short duration Very effective (K/w) Hemodynamic stability Restores acid-base balance continuosly allows iv fluids administration Does not increase IP Hemodynamic stability Low cost No anticoagulation No vascular access Does not increase IP Disadvantages -Coagulation -Risk of increase d IP -Hypotension episodes - Limited fluid removal - Continuous coagulation - Loses from the dialyser - High cost - Reduced dialysis dose - Infection risk - Affects respiration