Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
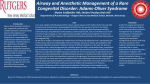
LETTERS TO EDITOR Anesthetic Management of clival chordoma with retropharyngeal extension: Importance of imaging Neha Singh, MD*, Parnandi Bhaskar Rao, MD, PDCC**, Devendra Gupta, MD, PDCC***, Sushil Prakash Ambesh, MD**** *Assistant Professor, Department of Anaesthesiology & Critical Care, P.I.M.S, Pondicherry-605014, India **Assistant Professor, Department of Anaesthesiology, Critical Care and Pain Medicine, AIIMS, Bhibaneshwar, Odisha, India ***Associate Professor, ****Professor Department of Anaesthesiology,Intensive Care and Pain Medicine,SGPGIMS, Lucknow- 226014, (U.P), India Correspondence: Dr. Neha Singh,MD; Assistant Professor, Department of Anaesthesiology & Critical Care, P.I.M.S, Pondicherry-605014, (India); Phone: +91-04132656271; Mobile: 91-8056625735; Fax: 91-0413-2656272; E-mail: [email protected] Dear Editor, Chordomas are rare but usually aggressive tumors originating from embryonic remnants of the primitive notochord which are usually extradural and induce bone destruction.1 Although 35% occur in the skull base, they represent only 0.1% of all skull base tumors.2 infusion 2 mcg/kg/hr. Surgery was performed in prone position followed by supine position and rest of the intraoperative period was uneventful. The duration of surgery was 11 hrs. Patient was shifted to neurosurgical ICU for elective ventilation and decannulated on fourth postoperative day. We emphasize on the importance of as specialized imaging techniques for planning definitive airway management which will lead to better perioperative outcome. A 45 year old,148-cm,52 kg, ASA II lady was presented with history of progressively increasing neck pain for 1 year, which aggravates on neck flexion and bilateral hard of hearing. Preoperative evaluation was satisfactory except for the involvement of XI and XII cranial nerves. As trans-oral approach was planned, we opted for an awake fiberoptic nasal intubation with tracheostomy backup in case of failed intubation. Patient was explained about the procedure and consent obtained. Pre-induction monitoring included electrocardiogram (ECG) lead II and V, noninvasive blood pressure (NIBP), heart rate (HR) and peripheral oxygen saturation (SpO2). Venous access was established by using two 16G cannula. She received intravenous midazolam (1.5 mg), fentanyl (100 µg) and propofol infusion @ 100150 mcg/kg/min. During fibreoptic intubation it was impossible to pass the scope beyond the nasopharynx due to an obstruction, so procedure was abandoned and surgical tracheostomy was performed under monitored anesthesia care. Radiographic review showed that the lesion has filled the nasopharyngeal space, obstructing the passage of a flexible fibreoptic scope (Fig.1). Following tracheostomy, anesthesia was induced with propofol (2.5 mg/kg), vecuronium bromide (0.1 mg/kg) and the circuit was connected to the tracheostomy tube. Anesthesia was maintained with Air:O2 :: 50:50, isoflurane 1-2%, vecuronium infusion 1 mcg/kg/min infusion and fentanyl ANAESTH, PAIN & INTENSIVE CARE; VOL 17(2) MAY-AUG 2013 Figure 1 Ch0rd0na Chordomas account for 1% of intracranial tumors and 4% of all primary bone tumors.2 Although survival from chordomas is generally considered to be poor,2 there has been improvement with modern treatments.3 Barrenechea IJ et al. mentioned the use of fibreoptic technique for intubation in cases of chordoma with cervical instability.4 As our plan of fibreoptic naso-tracheal intubation failed, tracheotomy was performed. In cases of expected difficult airway, it is suggested to consider fibreoptic intubation approach as the initial method of choice as it helps in detailed viewing of the anatomy, making it easy to decide the further plan to secure airway in anticipated difficult airway. Preoperative review of the imaging 211 letters to editor also add to the predicting ability in such cases. Flexible fibreoptic laryngoscopy has been a major advance in the management of difficult intubation.5 Although elective fibreoptic intubation is mostly successful, there are few reports where this technique may fail or not be possible REFERENCES 1. Sundaresan N, Rosen G, Boriani S. Primary malignant tumors of the spine. Orthop Clin North Am. Jan 2009;40:21-36. [PubMed] 2. Dahlin DC, Maccarty CS: Chordoma. Cancer 5 1952;28:1170–78. 3. Crockard HA, Steel T, Plowman N, Sıngh A, Crossman J, Revesz T et al. A multidisciplinary team approach to skull base chordomas. J because of laryngeal pathologies or abnormalities.6 With this experience of failed flexible fibreoptic intubation later managed by doing tracheostomy, we propose assistance of specialized imaging techniques before taking a decision regarding definitive airway management. Neurosurg 2001;95:175-83. [PubMed] Barrenechea IJ, Perin NI, Triana A, Lesser J, Costantino P, Sen C. Surgical management of chordomas of the cervical spine. J Neurosurg Spine. 2007 ; 6:398-406. [PubMed] 5. Ovassapian A, Dykes MHN. The role of the fibre-optic endoscopy in airway management. Seminars in Anaesthesia. 1987;7:93–104. 4. [Online Access] 6. Takenaka I, Aoyama K, Nakamura M, Fukuyama H, Urakami Y, Takenaka Y et al. Oral styletted intubation under video control in a patient with a large mobile glottic tumour and a difficult airway. Can J Anaesth 2002;49:203–6. [PubMed] Takayasu’s arteritis: An anesthetic challenge Nidhi Bhatia, MD, DNB*, Kiran Jangra, MD** *Assistant Professor, **Senior Resident Dept. of Anesthesiology & Intensive Care, Postgraduate Institute of Medical Education & Research, Sector-12, Chandigarh PIN-160 012, (India). Correspondence: Nidhi Bhatia, Assistant Professor, Dept. of Anesthesiology & Intensive Care, Postgraduate Institute of Medical Education & Research Sector-12, Chandigarh PIN-160 012, (India); Ph: +919914207483; Email: [email protected] Dear Editor, Takayasu’s arteritis (TA) is a chronic progressive panendarteritis involving the aorta and its main branches, associated with stenosis of major blood vessels, severe uncontrolled hypertension and end-organ dysfunction, making its perioperative management very challenging for the anesthesiologist. A 28 years old severely preeclamptic, full term parturient with HELLP syndrome and an intrauterine growth retarded (IUGR) baby, was scheduled for elective cesarean section. Twelve years back, she was diagnosed with TA, when she presented with dyspnea on exertion and a history of repeated blackouts. Since then she was regularly taking Tab prednisolone (Wysolone™, Wyeth Ltd.) aspirin and prazocin. On examination, pulsations were found to be absent in her both carotids and left upper limb. She had a feeble pulse in right upper limb but peripheral pulses in both lower limbs were normal. Patient’s baseline blood pressure was 90/60 mmHg in right upper limb and 190/110 mmHg in right lower limb. The patient’s respiratory and neurological examination showed normal results. Preoperative 212 investigations showed three fold elevated liver enzymes and low platelet count of 65,000, which increased to 1,50,000 after transfusion of single donor aphaeretic platelets. Rest of the investigations and fundus examination were within normal limits. Doppler examination confirmed the presence of bilateral carotid and right subclavian artery stenosis with normal renal arteries. Echocardiography showed the presence of normal left ventricular function with an ejection fraction of 50-55%, trivial mitral regurgitation and no regional wall motion abnormality. In the operating room, baseline monitoring and invasive BP through the right dorsalis pedis artery was done. 20G epidural catheter was placed in L3-L4 interspace, followed by subarachnoid block with 6.5 mg hyperbaric bupivacaine (0.5%) and 25 µg fentanyl in the same interspace. There after the patient was placed in supine position, with a left lateral tilt, and oxygen was administered via a face mask. Ephedrine boluses were used for hypotensive episodes. She remained hemodynamically stable in the intraoperative period and had an uneventful postoperative course. Four types of TA have been described in the literature1, with Type I involving the aortic arch and its main branches, ANAESTH, PAIN & INTENSIVE CARE; VOL 17(2) MAY-AUG 2013 letters to editor Type II being restricted to the descending thoracic and abdominal aorta, Type III combining both Types I and II and patients with Type IV showing involvement of even the pulmonary artery. Our patient was categorized as Type I, with involvement of the carotids and the brachiocephalic trunk. Ishikawa2 graded TA based on the presence of four major complications i.e., hypertension, retinopathy, aneurysm formation and aortic regurgitation. Pregnancy does not change the evolution of TA but increases risk of decompensation of hypertension.3 Peripheral vascular resistance normally decreases during pregnancy. As patients with TA have stenotic vessels and a decrease in afterload, blood pressure increases secondary to the increase in the blood volume that accompanies pregnancy4. These patients are known to have end-organ dysfunction as a result of severe uncontrolled hypertension and major arterial stenosis. They may also be receiving chronic steroid treatment and may present with Cushingoid features preoperatively. In such cases, perioperative steroid supplementation is needed to prevent the occurrence of Addisonian hypotensive crises.3,5,6 Invasive pressure monitoring is required in these patients to avoid hypoperfusion of brain and compromised fetus In the past, both regional and general anesthesia has been used successfully in these patients5,6 The choice of anesthetic technique should take into consideration maintenance of blood pressure in the intraoperative and postoperative periods. Regional anesthesia is preferred as level of consciousness and adequacy of cerebral perfusion can be better assessed in an awake patient. Moreover, according to previous reports, patients with preeclampsia are also benefited with regional anesthesia7 However, use of regional anesthesia in patients with TA might cause a precipitous fall in blood pressure due to sympathetic blockade, that may be hazardous in patient with compromised regional circulation because of stenosed arteries.3 So, in our patient, we decided to use low dose spinal anesthesia and supplement it with epidural block. A decrease in blood pressure was prevented with adequate preloading, Tredelenburg position and vasopressors. However, one needs to be very cautious while using vasopressors in patients with preexisting compromised organ perfusion. General anesthesia, on the other hand, is associated with major hemodyanamic fluctuations during induction, intubation and extubation which can increase blood pressure to dangerous levels in patients with severe preeclampsia. Drastic hypotension may be precipitated with drugs such as propofol, thiopentone, and inhalational anesthetic agents. To conclude, in patients with TA complicated by severe preeclampsia and compromised fetus, goal is to maintain or improve intrauterine perfusion while keeping patient’s vital signs stable. We conclude that combined spinal-epidural anesthesia is safer in these patients as no additional neurological monitoring is required and hemodynamics are better controlled. REFERENCES 1. Lupi-Herrera E, Sanchez-Torres G, Marcushamer J, Mispireta J, Horwitz S, Vela JE.et al. Takayasu’s arteritis: clinical study of 107 cases. Am Heart J 1977;93:94–102. [PubMed] 2. Ishikawa K. Natural history and classification of occlusive thromboaortopathy (Takayasu’s disease). Circulation 1978;57:27–35. [PubMed] [Free Full Text] 3. Ishikawa K, Matsuura S. Occlusive thromboaortopathy (Takayasu’s disease) and pregnancy. Clinical course and management of 33 pregnancies and deliveries. Am J Cardiol 1982;50:1293–300. [PubMed] 4. Check TG, Gutsche BB. Maternal physiologic changes during pregnancy. In: Anesthesia for obstetrics. Shnider SM, Levinson G, eds. Baltimore: Williams & Wilkins, 1987:3–13. 5. Kathirvel S, Chavan S, Arya VK, Rehman I, Babu V, Malhotra N, et al. Anesthetic management of patients with Takayasu’s arteritis: a case series and review. Anesth Analg 2001;93:605. [PubMed] [Free Full Text] 6. Sharma BK, Jain S, Vasishta K. Outcome of pregnancy in Takayasu arteritis. Int J Cardiol 2000;75:159-62. [PubMed] 7. Van Bogaert LJ. Spinal block for caesarean section in parturient with PIH. East Afr Med J 1998;75:227–31. [PubMed] ANAESTH, PAIN & INTENSIVE CARE; VOL 17(2) MAY-AUG 2013 213 letters to editor Endotracheal intubation with angiographic catheter after esophageal intubation in emergency department Sukhen Samanta, MD, PDCC*, Sujay Samanta, MD** *Department of Critical Care Medicine, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow-226014 (India) **Department of Anesthesia and Intensive Care, Post Graduate Institute of Medical Education and Research, Channdigarh-160012 (India) Correspondence: Dr. Sukhen Samanta, MD, PDCC(CCM), New PG Hostel, Room No. 218, SGPGI, Lucknow-226014 (India); E-mail: [email protected]; Mobile: 08004967745 Dear Editor, Airway management must ensure uninterrupted oxygenation and ventilation. It is a basic skill learnt during all emergency and critical care training sessions. Endotracheal intubation is a definitive way of securing airway. Unanticipated difficulty in endotracheal intubation can lead to increased morbidity, e.g. brain hypoxia, cardiac arrest and risk of aspiration. We faced an unanticipated difficult airway but successfully intubated the patient with a simple technique with the help of angiographic catheter (AC) in a limited resource situation. We have not found any mention in the literature of such an easy technique with minimum airway gadgets in difficult airway management. A 22 years old male, suffering from hepatic encephalopathy without coagulopathy, presented in our emergency department (ED) with Glasgow Coma Scale (GCS) 7/15 at midnight. Lung auscultation revealed right sided crepitations with SpO2 of 82% (probably due to aspiration). He required intubation for airway protection to prevent further aspiration and maintenance of oxygenation. His airway examination was apparently normal with unknown fasting status. After pre-oxygenation for 3 minutes he was induced with fentanyl and midazolam and preservative free lignocaine. On laryngoscopy, just tip of the epiglottis was barely visible (CL grade 3 b), even after optimum external laryngeal manipulation. An 8 mm endotracheal tube (ETT) with stylet was tried and the cuff inflated with air, but five point auscultation confirmed it to be inside the esophagus. We passed a 14 F nasogastric tube through the esophageal ETT in situ and suctioned his stomach contents. Then shifting the first ETT to left corner of the patient’s mouth, a second laryngoscopy was done. A sterile 9 F AC (Medtronic, Minnesota, USA) with guide wire, lubricated with lignocaine jelly, was passed just below the tip of epiglottis and through the glottis; a tactile sensation was felt by keeping the palm on trachea. A second ETT was now railroaded over the AC (Figure 1). In this way, the first ETT in the esophagus helped in preventing aspiration and guiding AC into trachea. Whole of the procedure was completed within 4 minutes without desaturating the patient (Figure 2). 214 Figure 1: Angiographic catheter with guide wire as airway exchange through ETT Figure 2: Patient with both ETT (esophageal & tracheal) in situ. Incidence of difficult laryngoscopy (defined as tracheal intubation requiring >2 attempts at direct laryngoscopy) is 1.5-8.5% in general anesthesia with failed intubation 0.3%.1 Alternative airway devices like the rigid or flexible fibreoptic bronchoscope, intubating laryngeal mask airway (ILMA), videolaryngoscope, C-Trach, and light wand etc. are very effective in this situation. Airway management in ED is often more challenging than in the operating rooms due to lack of difficult airway gadgets and expert help. In unanticipated difficult airway in pre-hospital emergency setting, people have used gum elastic bougies, ILMA and cricothyroidotomy.2] In the absence of such airway instruments in ED, an our simple technique may be tried. We suggest that if an esophageal intubation has inadvertently been done in a difficult intubation situation, don’t remove ANAESTH, PAIN & INTENSIVE CARE; VOL 17(2) MAY-AUG 2013 letters to editor it, rather keep it inflated to prevent aspiration. Even mask ventilation can be successfully done with the help of a small gauge piece sealing on left angle of the mouth. We used a sterilised AC with atraumatic guide wire with minimum cost. REFERENCES 1. 2. Crosby ET, Cooper RM, Douglas MJ, Doyle DJ, Hung OR, Labrecque P, et al. The unanticipated difficult airway with recommendations for management. Can J Anaesth. 1998;45:757-76. [PubMed] Combes X, Jabre P, Margenet A, Merle JC, Leroux B, Dru M, et al. Unanticipated Difficult Airway Management in the Prehospital AC has been used for nasogastric tube insertion but never used in airway management.3,4 AC can also be resterilised and can be kept inside the resuscitation kit from cardiac catheterization laboratories. Emergency Setting: Prospective Validation of an Algorithm. Anesthesiology. 2011;114:10510. [PubMed] [Free Full Text] 3. Rutala WA, Weber DJ. Healthcare infection control practices advisory committee (HICPAC). Guideline for disinfection and sterilization in healthcare facilities, 2008. Available from: http://www.cdc.gov/hipac/pdf/ guidelines/Disinfection_Nov_2008.pdf. [Online Access]. 4. Ghatak T, Samanta S, Baronia AK . A new technique to insert nasogastric tube in an unconscious intubated patient. North Am J Med Sci. 2013;5:68-70. [PubMed] [Free Full Text] Inadvertent hydrothorax after multi-lumen central venous catheter placement *Sujit Vasudevan Nair, MD*, Khalifa Abdullah Mohammed Al-Ghafri, MRCS**, Aziz Haris, MD, STARCSI*, Rashid Manzoor Khan, MD* and Naresh Kaul, MD* *Department of Anesthesia & ICU ** Department of Orthopedic National Trauma Center, Khoula Hospital, Muscat (Sultanate of Oman) Correspondence: Dr. Naresh Kaul, Sr. Consultant, Department of Anesthesia & ICU, Muscat (Sultanate of Oman); GSM: 00 968 99366241; E-mail: [email protected], A quadric-lumen central venous catheter was placed via the right subclavian route in a 15 year old healthy girl undergoing corrective surgery for scoliosis (D4 – L1) in the prone position under general anaesthesia. The distal most catheter port was kept closed as free flow of blood was absent in this channel. All other ports were working well. As the surgery progressed over next 45 min, central venous pressure and peak airway pressure gradually increased with a concurrent fall in blood pressure. All this was initially attributed to pressure being exerted over the back of the chest by the operating surgeon and a misplaced chest bolster. Also added to the confusion was observation of blood tinged watery fluid in the operative field which was erroneously attributed to be CSF leak from a dural rent. Fluids and other medications continued to be administered via the central line ports. It was only when hypotension was noted to be unresponsive to ephedrine injection via the central line that attention was directed to the possibility of accidental hydrothorax secondary to migration of the distal end of the central line. Immediate postoperative AP view of the chest X-ray confirmed this (Fig 1). Appropriate corrective measures were instituted and patient made an uneventful recovery. Clinical Pearls: 1. Aspirate free flow of relatively dark colored blood via the needle prior to introduction of the J-tip guide wire. 2. Ascertain free flow of blood via all lumens of the catheter prior to its fixation. 3. Re-aspirate blood after administration of 50-100 ml fluid,change of patient position, and whenever in doubt. Fig 1: Immediate postoperative chest x-ray (anteroposterior view) showing malpositioned subclavian central venous catheter. ANAESTH, PAIN & INTENSIVE CARE; VOL 17(2) MAY-AUG 2013 215