Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
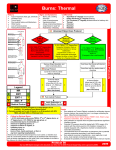
National Burn Service Referral Form Burn patient arrives – complete trauma ABC (if required) – complete first aid cooling (if not done) Referral Criteria for Regional Burn Unit (RBU) (Middlemore; Waikato; Hutt and Christchurch) • • • • • • • • If patient meets the criteria for National Burn Centre: Fax referral to 09 276 0114 and Contact call burn coordinator on 09 2503800 • • Burns greater than 10% total body surface area (TBSA) or 5% in a child Burns of special areas, eg. the face, hands, feet, genitalia, perineum, and major joints Full thickness burns greater than 5% TBSA Electrical burns (including lightning injury) Chemical burns Burn injury with inhalation injury Circumferential burns of the limbs or chest Burns at the extremes of age, ie. young children and the elderly Burn injury in patients with pre-existing medical disorders that could complicate management, prolong recovery, or affect mortality Any patient with burns and concomitant trauma (e.g. fractures) in which the burn injury poses the greater immediate risk of morbidity or mortality Referral Criteria for National Burn Centre Burns greater than 30% total body surface area Full thickness burns to face,hands,feet,genitalia,perineum Burn injury with significant inhalation injury High voltage electrical burns Significant chemical burns FAX & PHONE REFERRAL TO: NATIONAL BURN CENTRE Ph: Fax: Email Photos : 09 2503800 ( on call burn coordinator) 09 2760114 [email protected] Fax From: Designation: Date: Number of pages: 3 Objective ID: A7330 Version: 3 Department: National Burn Centre Last Updated: 25/11/2013 Document Owner: Burns Clinical Nurse Specialist Next Review Date: 25/11/2014 Approved By: NBC Policies, Procedures and Guidelines Group Date First Issued: 29/11/2006 Counties Manukau District Health Board National Burn Service Referral Form Initial Treating Consultant: _______________________ Ph: ______________________ Patient label Department: ____________________________________ Fax: ______________________ Referring Hospital: _____________________________________________________ Injury Details: Time/Date of Injury: ______________________ ACC 45 No. _______________________ Arrival Date/Time at Hospital: _________________________________________________ Next of Kin or Accompanying Person: Ph:______________________ __________________________________ How Accident Happened: ____________________________________________________ Initial Assessment: _________________________________________________________________________ Airway: ______________________________________________________ _________________________________________________________________________ Breathing: ___________________________________________________ State of consciousness when found: ____________________________________________ Circulation: ___________________________________________________ Other Injuries: _____________________________________________________________ - adequate supply to limbs? Yes / No (please circle) _________________________________________________________________________ Cervical injury: ________________________________________________ Burn occurred in confined space? Yes No Was there an explosion? Yes No 10-19 mins 20+ mins Cooled at scene? 0-9 mins Tetanus toxoid: Current? Yes / No / Don’t Know (please circle) Analgesics Given: _____________________________________________ Escharotomies? Yes No Where? _______________________________________________ Past Medical History: ________________________________________________________ Transfer Checklist: _________________________________________________________________________ Daily Alcohol Intake: ________________________________________________________ Current Medications: ________________________________________________________ Allergies: Yes/No __________________________________________________________ Suicide attempt or deliberate self harm? Yes No Unsure Known Psychiatric History: ___________________________________________________ Yes Intubated Tetanus toxoid given Naso-gastric tube Oxygen Escharotomies Uretheral catheter Venous access Blood gases Urea: electrolytes, full blood count Urinalysis Jewellery removed Baseline data attached Fluid Balance Chart attached Burns Chart attached (Lund & Browder) X-rays and notes (copies) sent No n/a National Burn Service Referral Form Patient Weight: ___________ kg Lund & Browder Burn Chart Fluid Replacement Guide Areas Burned First 24 Hours - Crystalloid (eg. Plasmalyte, Lactated Ringers) Do not include simple erythema. 1 – 2 ml/kg/hr) – use Dextrose Saline: Up to 10kg: + from 10-20kg: + each kg >20kg: 4 ml/kg/hr 2ml/kg/hr 1 ml/kg/hr NB: This formula is a guideline only and does not replace clinical judgement. ADJUSTMENT WILL be necessary to maintain urine output. Wound Management If circumferential consider escharotomies Area Please consult with Regional Burn Unit for advice prior to applying any wound care product. Every Emergency Department has a Burn Cache with dressing products, Escharotomy and Initial management guidelines. > > Age 0 1 5 10 15 Adult A=½ of head 9½ 8½ 6½ 5½ 4½ 3½ B=½ of one thigh 2¾ 3¼ 4 4¼ 4½ 4¾ C=½ of one leg 2½ 2½ 2¾ 3 3¼ 3½ 0.5 ml/kg/hr 1 ml/kg/hr (haemoglobinuria / myoglobinuria For Children ADD maintenance fluids Size of Burn (% body surface area): ___________ Urine output Adults: Children: 3-4 ml x kg x % burn Give approximately half in first 8 hours from time of burn, half in next 16 hours Partial Thickness Full Thickness Monitoring NB:This formula is a guideline only and does not replace clinical judgement. Adjustment may be necessary to maintain urine output. Time (hourly) Rate Fluid in / hr Urine Out / hr National Burn Service Referral Form