Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
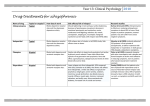
UP Health System – Marquette Pharmacy and Therapeutics Committee Medication Guideline Drug Classification: 28:16.08.04 Atypical Antipsychotics Agent: Formulary X Aripiprazole (Abilify®) Asenapine (Saphris®) X Clozapine (Clozaril®) Iloperidone (Fanapt®) X Lurasidone (Latuda®) X Olanzapine (Zyprexa®) Olanzapine pamoate (Zyprexa® Relprevv®) X Paliperidone (Invega®) Paliperidone palmitate (Invega® Sustenna®) X Quetiapine (Seroquel®) X Risperidone (Risperdal®) X Risperidone injection (Risperdal® Consta®) X Ziprasidone (Geodon®) Nonformulary Restricted X X Nonstock X X X X X X X X X X X X X X X Pharmacy and Therapeutics Committee-approved Indications for Inpatient Use: Each of the atypical antipsychotics have unique pharmacological properties that may be considered in certain situations as follows: aripiprazole, ziprasidone, or lurasidone may be preferred in patients who are over-weight or obese; quetiapine may be preferred in patients who experience intolerable extrapyramidal symptoms on risperidone. Lower initial dosages should be considered for elderly patients. Atypical antipsychotic agents should be reserved for patients unable to tolerate or who have failed traditional antipsychotic agents (i.e., haloperidol, perphenazine). Additionally, generic versions of the atypical antipsychotic agents should be considered whenever possible. Intramuscular therapy: Olanzapine/ziprasidone (short-acting only): o o Treatment of acute agitation in patients with schizophrenia or bipolar mania unable to receive oral therapy. These atypical antipsychotic injections will be made available in the Emergency Department and Psychiatric care areas only, use outside of these areas must be approved by Psychiatry. Risperidone injection: o o Risperidone long-acting injection is available for continuation of chronic, stable outpatient therapy. Therapy initiated in hospitalized patients requires the following criteria to be met: A history of non-adherence to oral medications has been documented and behavioral and other adherence interventions have been aggressively attempted and failed. Risperidone long-acting injection will be continued as an outpatient. Patient has a documented history of tolerability to oral risperidone. Carbamazepine is discontinued prior to initiating risperidone long-acting injection. Patient is 18 years of age or older. Formulary depot first-generation antipsychotics have been attempted at a clinically significant dosage and duration without response, with the development of intolerable side effects, or are documented to be clinically inappropriate. Oral therapy: Continuation of chronic, stable outpatient therapy. Clozapine: see special procedures for clozapine utilization starting on page 4. Low-dose therapy (i.e., quetiapine <100 mg daily) for the treatment of symptoms associated with dementia (psychosis, agitation) must be approved by Psychiatry. Unless used for conditions stated above, requests for all oral atypical antipsychotic agents must be approved by Psychiatry. Note: Atypical antipsychotics should not be used as sleep aids. Document created: 04/12. Revised: 03/16. Cross Reference: None UP Health System – Marquette A Duke LifePoint Hospital Marquette, MI 49855 This is a confidential professional/peer review and quality assessment document of Marquette General Health System of Marquette, MI. It is protected from disclosure pursuant to the provisions of MCL 333.20175, MCL 333.21513, MCL 21515, MCL 331.531, MCL 331.533, MCL 330.1143a, and other state and federal laws. Unauthorized disclosure or duplication is absolutely prohibited. UP Health System – Marquette Pharmacy and Therapeutics Committee Medication Guideline Usual Dosage: See table below for dosing information. Monitoring / Outcomes: Therapeutic Response: Reduction in symptoms including positive symptoms (i.e., hallucinations, irritability, delusions, incoherent speech, suspiciousness) and negative symptoms (i.e., blunted affect, emotional or social withdrawal, poverty of speech content, lack of initiative). Adverse Effects: Extrapyramidal symptoms (i.e., continuous pacing, restlessness, fine tremor, abnormal posturing, spasticity, hypertonus), tardive dyskinesia, neuroleptic malignant syndrome, prolongation of the QT interval, orthostatic hypotension, somnolence, impaired judgment or motor skills, weight gain, hyperlipidemia, hyperglycemia. Special Handling Procedures: Atypical antipsychotics are not considered hazardous drugs. Atypical antipsychotics are not considered high-alert drugs. Document created: 04/12. Revised: 03/16. Cross Reference: None UP Health System – Marquette A Duke LifePoint Hospital Marquette, MI 49855 This is a confidential professional/peer review and quality assessment document of Marquette General Health System of Marquette, MI. It is protected from disclosure pursuant to the provisions of MCL 333.20175, MCL 333.21513, MCL 21515, MCL 331.531, MCL 331.533, MCL 330.1143a, and other state and federal laws. Unauthorized disclosure or duplication is absolutely prohibited. UP Health System – Marquette Pharmacy and Therapeutics Committee Medication Guideline Table: Available Atypical Antipsychotic Agents Dosage Comparison. Agent Maximum Daily Dose Dose Adjustment in Renal/Hepatic Impairment? 10-30 mg (once daily) 30 mg No dosage adjustment required for renal or hepatic impairment 12.5 mg once or twice daily (titration is required, see detailed information below for clozapine) 300-450 mg (divided twice daily) 900 mg No dosage adjustment required for renal or hepatic impairment 40 mg once daily Give with food. 40-80 mg (once daily) 80 mg 5-10 mg daily (titrate by 5 mg/day at intervals of at least several days) 5-20 mg (once daily) 20 mg 5-10 mg IM as required (may repeat 10 mg every 2 hours) N/A 30 mg 3 mg once or twice daily (titrate by 3 mg/day at intervals of at least 5 days) 6-12 mg (divided 2 times daily) 12 mg Starting Dose Maintenance Dosage 10-15 mg once daily (titrate at intervals of least two weeks) Clozapine Lurasidone Aripiprazole Olanzapine Paliperidone Quetiapine Risperidone Ziprasidone 25-50 mg twice daily (titrate by 50 mg at intervals of at least 2 days) Renal Do not exceed 40 mg/day for moderate to severe impairment Hepatic Do not exceed 40 mg/day for moderate to severe impairment No dosage adjustment required for renal or hepatic impairment 200-800 mg (divided 1-2 times daily) 800 mg Renal 50-80 ml/min: 6 mg/day max 10-50 ml/min: 3 mg/day max Hepatic Limited data available at this time; however, paliperidone undergoes limited hepatic metabolism Renal No dosage adjustment required Hepatic Initiate therapy at 25 mg/day 300 mg once daily (titrate at intervals of at least 1 day) 300-800 mg (once daily) 1 mg twice daily (titrate by 1 mg twice daily on days 2 and 3, as tolerated) 2-8 mg (divided 1-2 times daily) 8 mg Recommended initial dose in severe renal or hepatic impairment is 0.5 mg twice daily (titrate by 0.5 mg twice daily to max of 3 mg/day) 25-50 mg every 2 weeks 50 mg every 2 weeks 25 mg every 2 weeks (max) 120-160 mg (divided 2 times daily) 160 mg 12.5-25 mg every 2 weeks (titrate at intervals of at least 4 weeks)* 20 mg twice daily (titrate at intervals of at least 2 days) Give with food. No dosage adjustment required for renal or hepatic impairment 10 to 20 mg IM as required (may repeat 10 mg every two N/A 40 mg hours or 20 mg every four hours) † * Oral risperidone or another antipsychotic medication should be given with the initial injection and should be continued for 3 weeks and then discontinued. † Intramuscular administration of ziprasidone for more than three consecutive days has not been studied. Document created: 04/12. Revised: 03/16. Cross Reference: None UP Health System – Marquette A Duke LifePoint Hospital Marquette, MI 49855 This is a confidential professional/peer review and quality assessment document of Marquette General Health System of Marquette, MI. It is protected from disclosure pursuant to the provisions of MCL 333.20175, MCL 333.21513, MCL 21515, MCL 331.531, MCL 331.533, MCL 330.1143a, and other state and federal laws. Unauthorized disclosure or duplication is absolutely prohibited. UP Health System – Marquette Pharmacy and Therapeutics Committee Medication Guideline Pharmacy and Therapeutics Committee-approved Indications for Inpatient Use of Clozapine: Management of treatment-resistant schizophrenia in severely ill patients who fail to respond adequately to other antipsychotic therapy and/or in whom such therapy produces intolerable adverse effects. Reduction in risk of recurrent suicidal behavior in patients with schizophrenia or schizoaffective disorder who are judged to be at chronic risk for re-experiencing suicidal behavior. NOTE: Due to the significant risk of agranulocytosis, clozapine is only available to MGH through a restricted distribution system and may only be dispensed following confirmation of patient and physician registration with the Clozapine REMS (Risk Evaluation and Mitigation Strategy) Program. This registry ensures appropriate monitoring of absolute neutrophil counts (ANC) throughout the course of therapy. Patients may not receive the medication at MGH without verification of registration. In addition, physicians ordering clozapine must be registered via the Clozapine REMS Program and this information confirmed by pharmacy prior to order verification. Failure to comply with these registration requirements will jeopardize the ability of MGH to maintain and dispense clozapine. Prescribers or their designees can enroll patients at the Clozapine REMS Program website located at www.clozapinerems.com. The pharmacist can then verify prescriber certification and patient eligibility at the Clozapine REMS website. Dosage & Administration: Treatment Initiation & Maintenance: Begin with 12.5 mg (one-half of a 25 mg tablet) twice daily. If well tolerated, increase dose according to the CLOZARIL (CLOZAPINE) TITRATION order. In general, doses should be increased by 25 to 50 mg daily over a 2-week period until a target dose of 300 to 450 mg daily is achieved. Subsequent dosage increments should not exceed 100 mg and should be made no more than once or twice-weekly. Dosing should not exceed 900 mg/day and should be administered in divided doses (i.e., 2 to 3 times daily) to minimize the risk of certain adverse effects. Patients should be maintained on the lowest effective dose of clozapine. Prior to initiation of clozapine, it should be confirmed that the patient is not taking any medications that have the potential to cause agranulocytosis or otherwise suppress bone marrow function (e.g., carbamazepine). Discontinuation of treatment: Gradually reducing the dose over a 1- to 2-week period is recommended; however, abrupt discontinuation may be warranted if the patient develops leukopenia, granulocytopenia, or agranulocytosis. Re-Initiation of treatment: If treatment is interrupted for ≥48 hours, dosing must be reinitiated at 12.5 to 25 mg/day. Therapy can NOT be reinitiated in patients in whom therapy was discontinued due to an absolute neutrophil count (ANC) <1,000/µL in the general population. Pharmacy Dispensing Procedures Dispensing of clozapine is contingent upon confirmation of patient and physician registration and ANC results. Dose How available 12.5 mg dose will be dispensed as half of a 25 mg tablet 37.5 mg dose will be dispensed as a one 12.5 mg (half of 25 mg tab) + one 25 mg tablet 50 mg dose will be dispensed as a one 50 mg tablet Doses >50 mg variable with 25 mg, 50 mg, and 100 mg tablets I. New/Continuing Therapy 1. Providers and/or their designees registered in the Clozapine REMS Program must initially enroll patients on the Clozapine REMS Program website The pharmacist should then collect the following Document created: 04/12. Revised: 03/16. Cross Reference: None UP Health System – Marquette A Duke LifePoint Hospital Marquette, MI 49855 This is a confidential professional/peer review and quality assessment document of Marquette General Health System of Marquette, MI. It is protected from disclosure pursuant to the provisions of MCL 333.20175, MCL 333.21513, MCL 21515, MCL 331.531, MCL 331.533, MCL 330.1143a, and other state and federal laws. Unauthorized disclosure or duplication is absolutely prohibited. UP Health System – Marquette Pharmacy and Therapeutics Committee Medication Guideline 2. 3. 4. 5. patient demographic information and most recent (≤7 days) ANC for entry into the Clozapine REMS Program Website in order to verify patient eligibility: 1) patient first and last name, 2) date of birth, and 3) prescribing physician name and DEA number. The pharmacist will then verify that the patient ANC result is current and acceptable as well as verify prescriber certification and patient enrollment in the registry. For patient and physician registration verification in the Clozapine REMS program, the pharmacist may sign into the website at www.clozapinerems.com or by calling the Clozapine REMS Program contact center at 1-844-267-8678. The patient’s status in the registry will state “The below patient is eligible to receive clozapine” once the above information is entered into the website. Once approval is noted during the patient eligibility check from the Clozapine REMS Program, the pharmacist may verify the order in the electronic medical record (EMR). The pharmacist should communicate with the prescribing physician that an “ANC” needs to be ordered weekly while the patient is receiving treatment. Pharmacist will record the ANC data throughout hospitalization as required in the Monitoring/Outcomes section of these guidelines. This information must be entered in the patients file on the Clozapine REMS program website. Monitoring / Outcomes: Laboratory: WBC and ANC*, fasting blood glucose, liver function tests. *ANC = Total WBC count x total percentage of neutrophils obtained from the differential Example (WBC = 4.3 & Neutrophils = 50%): ANC=4300 x 0.5 = 2,150 (2.15) First 6 months: ANC must be obtained at baseline and weekly. Month 6-12: If counts remained acceptable (ANC ≥1500/µL) during the first 6 weeks, monitoring may be decreased to every 2 weeks for the next 6 months. Month 13-18: If ANC continues to remain within these acceptable limits after the second 6 months of therapy, monitoring can be decreased to every 4 weeks.. After discontinuation of clozapine for neutropenia: If therapy is interrupted due to moderate neutropenia (ANC of 500-999/µL) or severe neutropenia (ANC < 500/µL) in the general population ,the ANC must be reported daily until the ANC is ≥ 1000/µL and then three times weekly until the ANC is ≥ 1500/µL. Patients diagnosed with Benign Ethnic Neutropenia (BEN) have different overall recommendations for monitoring recommendations when neutropenia is noted (ANC < 1000/µL) and specific recommendations for monitoring can be found at the Clozapine REMS website. Specifically, clozapine therapy should be interrupted in the BEN population only in severe neutropenia (ANC < 500/µL) and then must reported daily until the ANC is ≥ 500/µL and then three times weekly until the ANC is ≥ patient’s established baseline ANC values. Therapeutic Response: Improvement of psychotic symptomatology (e.g., improved communication, decreased hallucinations and delusions, improved socialization, decreased paranoia) Adverse Effects: Leukopenia, granulocytopenia, agranulocytosis, tachycardia, hypotension, ECG changes, sedation/drowsiness, dizziness/vertigo, sialorrhea, seizures, fever, constipation. Document created: 04/12. Revised: 03/16. Cross Reference: None UP Health System – Marquette A Duke LifePoint Hospital Marquette, MI 49855 This is a confidential professional/peer review and quality assessment document of Marquette General Health System of Marquette, MI. It is protected from disclosure pursuant to the provisions of MCL 333.20175, MCL 333.21513, MCL 21515, MCL 331.531, MCL 331.533, MCL 330.1143a, and other state and federal laws. Unauthorized disclosure or duplication is absolutely prohibited.