Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Pharmaceutical marketing wikipedia , lookup
Prescription costs wikipedia , lookup
Compounding wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Theralizumab wikipedia , lookup
Medical prescription wikipedia , lookup
Pharmacogenomics wikipedia , lookup
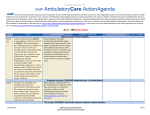
ISMP Educating the Healthcare Community About Safe Medication Practices Medication Safety Alert! Community/Ambulatory Care Edition ¿Comprende? Not Necessarily Many people who are acutely ill or require ongoing therapy for a chronic condition have trouble adhering to a prescribed plan of care. Some limits occur as a result of emotional distress, clinical condition, or socioeconomic factors. But pharmacists should also consider the possibility that poor health literacy—the ability to read, understand, and act on healthcare information—is a barrier to adherence for many patients. Older patients, people with chronic diseases, recent immigrants, and patients who do not speak English as their primary language, or at all, are especially likely to exhibit low health literacy. ISMP recently received a report from a community pharmacist who works in a setting where 90% of her patients are Spanish-speaking. An elderly man, who did not speak or read English, returned to the pharmacy for more information after having taken a portion of a methylprednisolone dose pack. He had not received appropriate instructions about how to administer this complicated dosing regimen, and he was not taking the medication correctly. Fortunately, the gentleman was not harmed, but he didn’t receive the full intended benefits of the drug either. ® E-mail: [email protected] Hotline: 1 800 FAIL SAF(E) Volume 7, Issue 1 January 2008 Safety Briefs A 2004 study among Spanish-speaking Latino parents with limited English proficiency who where given prescription Anonymous patches. Nurses and pharmacists have reported that CATAPRES (clonidine) patches present problems because the manufacturer does not print the name or strength of the drug on the patch itself. The patches are available in a variety of strengths and are worn for a week at a time. Problems are often reported, especially if the dose of a drug delivered via patch is changed, or if the patient requires multiple patches. Long-term care settings seem to be particularly vulnerable to problems using this product. Because the Catapres patch does not contain the name of the drug, caregivers can determine only that something is on the skin. They cannot determine the drug, the dose, or, in some cases, even distinguish it from adhesive bandages and specialty dressings. This can lead to errors. For example, a nurse could receive a new order for a clonidine patch or an oral dose of clonidine, and Figure 1. The BI 33 code on proceed to administer this Catapres TTS 3 patch additional medication not indicates it contains 0.3 mg. realizing that the patient already has a clonidine patch affixed. Or, if the patient has a clonidine patch along with another unlabeled drug patch (e.g., LIDODERM [lidocaine]), the wrong patch can be removed and replaced with the same patch that remains on the patient. Thus, the patient would receive a double dose of one medication and none of the other. Another error-prone feature is the ability of Catapres’ cover to be mistaken for the actual drug patch and applied to the skin. We contacted the manufacturer, Boehringer Ingelheim, about this longstanding problem and learned that they have no immediate plans to print the drug name and dose on the patch. We were also advised that the patch should not be written on because it is not known if volatile chemicals contained in ink might affect delivery of the drug. However, the manufacturer did note that the patch cover could be labeled and placed over the drug patch to protect it. There’s also a code on each patch cont’d on page 2 cont’d on page 2 Studies have shown that 36% of Americans function at the basic health literacy level or lower.1 It is even more significant (66%) for Americans of Hispanic race/ethnicity. Another study from a national managed care organization described the literacy of 54% of Spanish-speaking Medicare enrollees to be inadequate or marginal.2 Pharmacists should not assume that Spanish-speaking patients who seem comfortable speaking English will understand a prescription label written in English. It is also wrong to assume that patients who speak Spanish can understand medication instructions written in Spanish. This fact has not gone unnoticed by the pharmacist who reported the error described above. She has observed that in the Hispanic community she serves, of which she is a member, it is common for patients to indicate they understand what a healthcare provider has said, even when they don’t fully understand the instructions or how to access the information independently. ISMP Medication Safety Alert!® January 2008 page 2 ¿Comprende? (cont’d from page 1) labels in English and corresponding medication information leaflets in Spanish exemplified this.3 The parents were asked to read the medication label and the information sheet and then answer questions regarding the medication and proper dosing. Of the 100 participants in the study, only 22% would have given a correct dose of medication to their child and only 29% were able to answer questions regarding the medicine dosage and proper use as a result of having access to written information in Spanish. Also noteworthy in the study was the fact that even among subjects who selfdescribed themselves as being comfortable speaking English, only 50% were able to demonstrate knowledge that would allow them to accurately prepare a dose of their child’s medication. SAFE PRACTICE RECOMMENDATIONS: In order to help members of this patient population use medications safely, a number of interventions must be employed. Here are some suggestions that can make your patient education sessions more successful. Assess a patient’s level of comprehension. A new screening tool, which takes a few minutes to administer, has been developed to assess comprehension levels of common medical terms amongst Spanish-speaking people. The Short Assessment of Health Literacy for Spanish-speaking Adults (SAHLSA) identifies Spanish-speaking adults with low health literacy.4 Notations should be made in these patients’ profiles and charts to alert practitioners and foster supplemental education for these patients at each follow-up visit. You may obtain the SAHLSA by emailing University of North Carolina at Chapel Hill’s professor Dr. Shoou-Yih D. Lee at [email protected]. Offer supplemental counseling. Low health literacy patients can receive supplemental patient education that is tailored to meet their needs. When pharmacists understand the special healthcare needs of Spanish-speaking people with low health literacy and consistently offer customized patient education, medication errors due to dosage and indication confusion can be prevented. Supply language-appropriate patient information. Consider placing Spanish-speaking pharmacists in areas with a high percentage of Spanish-speaking patients. In practices with fewer Spanish-speaking patients, forge a working relationship with a pharmacist who is fluent in Spanish to assist in patient counseling. One of our reviewers cont’d on page 3 Safety Briefs (cont’d from page 1) (see figure 1) that can be used to identify the strength: BI 33 designates a 0.3 mg patch, BI 32 is 0.2 mg, and BI 31 is a 0.1 mg patch. Share these codes when dispensing these patches. Educate patients about this issue. Inform them of the need to keep an accurate, upto-date list of their medications, including the date each patch was applied. Long-term care pharmacies and facilities should consider attaching a notation about the code designation along with the inventory item so that dosing information appears on computer-generated medication administration records. “4 QD”, a sure thing for a daily overdose. A psychiatrist wrote a prescription (see figure 2) for lithium carbonate, used to manage bipolar disorder, as “LiCO3 300 mg 4 QD.” The pharmacy technician interpreted it as take 4 capsules once daily and entered it into the computer as such. When the pharmacist reviewed the prescription, Figure 2. she made the same interpretation but then questioned the daily dosing of the immediate-release product. The pharmacist checked the patient’s profile and noted the patient was previously taking 300 mg three times daily. The pharmacist called the prescriber’s office, and the nurse verified the prescription was written as “4 QD,” which in their practice meant “take 1 capsule four times a day.” Given the potential for confusion and risk for patient harm, healthcare practitioners should stop using the abbreviation “QD” in all forms of communication. In the case above, not only was “QD” used but it was used incorrectly. Instead, use the word “daily” in place of “QD.” When expressing the directions “four times a day,” it is best to use the complete English words, although the abbreviation “QID” is acceptable. OTC cough and cold medicines. FDA recommends that over-the-counter (OTC) cough and cold drugs not be used to treat children less than 2 years of age because serious and potentially life-threatening side effects can occur. FDA has not completed its review of information about the safety of OTC cough and cold medicines in children 2 through 11 years of age. For more information visit: www.fda.gov/medwatch/safety/ 2008/safety08.htm#cough. ISMP Medication Safety Alert!® January 2008 page 3 ¿Comprende?(cont’d from page 2) has been able to do this in his ambulatory care practice with good success. Also, the National Library of Medicine and the National Institutes of Health have produced easy-to-read medication information leaflets in both English and Spanish. They are available on-line at: www.nlm.nih.gov. Provide small amounts of verbal information at one time. First, in simple everyday language, tell patients what they truly need to know to take their medications safely and to identify important side effects. Emphasize desired behavior, not the medical facts. Leave extensive overviews of interactions and side effects for later encounters. Avoid using medical terminology and jargon. Use multi-media visuals. Another strategy to consider for patients with low health literacy is the use of multi-media visuals aids, such as video, audiotapes, and CDs, preferably in the patient’s primary language. Supplementing written instruction sheets with drawings and simple pictograms can also help patients understand how to take their medication. Many simple black and white pictograms are available from the U.S. Pharmacopeia at: www.usp.org/audiences/ consumers/pictograms. Verify the patient’s understanding. Use the Teach-Back Method to counsel patients. Avoid asking “yes” or “no” questions. Instead, ask patients to show you and tell you how they would take their medicine so that you can correct knowledge gaps. Pharmacy personnel can assess comprehension by having patients repeat instructions in their own words. Listen for accuracy. The preferred way to assess knowledge, though, is to have the patient or caregiver actually demonstrate how they will measure the dose and administer the drug using the actual product, drug delivery devices, or a sample product. The Institute for Safe Medication Practices is an independent nonprofit agency. ISMP accepts no advertising. The contents of this newsletter are copyrighted. ©2008 Institute for Safe Medication Practices. Law strictly prohibits redistribution, reproduction, or republication by recipients through any means, including print, e-mail, or fax, without written permission by ISMP. Contact ISMP for subscription rates. For more information regarding low health literacy and resources to promote effective learning among low health literacy clients, please visit www.npsf.org/askme3 or www.ohiopatientsafety.org. Please note that Medication Safety Brochures written at the 2nd-3rd grade level are available at the latter website in both English and Spanish. References: 1.) Kutner M., et al. The Health Literacy of America’s Adults: Results From the 2003 National Assessment of Adult Literacy (NCES 2006–483). U.S. Department of Education.Washington, DC: National Center for Education Statistics. 2006. Available on the Internet at: http://nces.ed.gov/ pubsearch/pubsinfo.asp?pubid=2006483; 2.) Gazmararian JA, et al. Health literacy among Medicare enrollees in a managed care organization. JAMA. 1999; 281:545-551. Available on the Internet at: http://jama.ama-assn.org/cgi/content/ ful/281/6/545; 3.) Leyva M, Sharif I, Ozuah PO. Health literacy among Spanish-speaking Latino parents with limited English proficiency. Ambulatory Pediatrics. 2005;5:56-59; 4.) Lee SY, et al. Development of an easy-to-use Spanish health literacy test. Health Services Research. 2006;41(4p1): 1392–1412. Announcements Now accepting applications for the 2008-2009 ISMP Safe Medication Management Fellowship! The Fellowship, sponsored by Cardinal Health Foundation, offers an experienced healthcare provider an unparalleled opportunity to learn from and work with some of the nation’s experts in medication safety. The 12-month Fellowship commences in Summer 2008 at the suburban Philadelphia office of ISMP. Please join us on February 18, 2008, at 1:00 p.m. ET for a special, live conference call about the Fellowship. Current and past Fellows will describe their experiences during their Fellowship as well as discuss their post-Fellowship careers. They will also be available to answer any questions about the Fellowship. To join the call, please email Barbara Olson, the current ISMP Fellow, at: [email protected]. Subscription Information Individual subscription rates are $48 per year for 12 monthly issues. Discounts are available for organizations with multiple sites or multiple users. For more information, contact ISMP at 215-947-7797 or e-mail to [email protected]. ISMP Medication Safety Alert! Community/Ambulatory Care Edition (ISSN 1550-6290) ©2008 Institute for Safe Medication Practices (ISMP). ISMP® is an FDA MEDWATCH partner. Call 1-800-FAIL-SAF(E) to report medication errors to the USP-ISMP Medication Errors Reporting Program (MERP) or report on-line at www.ismp.org or www.usp.org. Unless noted, published errors were received through the MERP. ISMP guarantees confidentiality and security of information received and respects reporters’ wishes as to the level of detail included in publications. Editors: Michael J. Gaunt, PharmD; Michael R. Cohen, RPh, MS, ScD; Judy Smetzer, RN, BSN. Reviewers: ISMP staff and Tabitha Carreon, PharmD, RPh; Eddie Dunn, PharmD; Richard A. Feifer, MD; Charlotte Huber, RN, MSN; Stan Illich, RPh, MHA; Crystal Lennartz, PharmD, MBA; Patrick McDonnell, PharmD; Andrew Seger, PharmD; Kelly J. Stanforth, PharmD, FISMP; Hermine Stein, DO; Kimberly Tallian, PharmD, FCSHP, FASHP; Chuck Young, RPh, CFE. Institute for Safe Medication Practices, 1800 Byberry Road, Suite 810, Huntingdon Valley, PA 19006. Tel. 215-947-7797; Fax 215-9141492; E-MAIL: [email protected]. This is a peer-reviewed publication. Copyright © 2008 ISMP. Duplication is permitted only for internal distribution at your practice site. Duplication by any means for distribution outside your site is strictly prohibited. ©2008 ISMP ActionAgenda The numbers visible in the dose indicator window in Pulmicort Flexhaler (budesonide inhalation powder) provide confusing information to patients. The dial is labeled in increments of 20, and actual movement of the dose-counter may not be discernable. Patients may have difficulty telling if a dose has been received. 10 January 2008 Confusion regularly occurs when patients must convert SYMLIN (pramlintide acetate)—dosed in micrograms—into units in order to administer Symlin using a manufacturer-recommended U-100 insulin syringe. Recently, a patient nearly administered a 6-fold overdose of Symlin before consulting his community pharmacist for dose confirmation. Failure to validate patient learning contributed to the near miss. A labeling mistake that would have resulted in a significant under-dose of VICODIN (hydrocodone and acetaminophen) was discovered during a patient counseling session. Poor penmanship on the part of the prescriber contributed to “q6h” being interpreted as “qd.” Problem 7 7 Issue No. Organization Assessment ISMP MedicationSafetyAlert! ® Community/Ambulatory Care Edition Patients who use Pulmicort Flexhaler should receive explicit instructions about how to actuate the device, the slow-moving design of the dose counter, and how to tell when the device is empty. The manufacturer will provide tear sheets and updated information on the Pulmicort Flexhaler website once patient instruction revisions are approved by FDA. Dose countdown misleading When complex dose conversion is necessary, patients must receive thorough instructions and provide healthcare providers with a “teach back.” Symlin teaching should include: the prescribed dose; information about how and when to adjust Symlin doses; converting a dose from mcg to units; how to use an insulin syringe to draw up the correct dose; administration times; how to administer a dose; when to measure blood glucose levels; and blood glucose values to report to the prescriber. The newly approved Symlin peninjector device may eliminate this problem. Is this how I administer my Symlin? Use patient counseling sessions as a final check of prescription accuracy. Knowledge of typical Vicodin dosing and the practice of patient counseling using the original prescription allowed a second pharmacist to discern this error and take corrective action before the prescription was dispensed. Patient counseling with original Rx Recommendation Action Required/Assignment QAA 1 Date Completed One of the most important ways to prevent medication errors is to learn about problems that have occurred in other organizations and to use that information to prevent similar problems at your practice site. To promote such a process, the following selected agenda items have been prepared for you and your staff to stimulate discussion and collaborative action to reduce the risk of medication errors. These agenda topics appeared in the ISMP Medication Safety Alert! Community/Ambulatory Care Edition between July 2007 and December 2007. Each item includes a brief description of the medication safety problem, recommendations to reduce the risk of errors, and the issue number to locate additional information as desired. ISMP AmbulatoryCare July - December 2007 ©2008 ISMP Two formulations of BYETTA (exenatide) are distributed in pen injectors, one delivering 5 mcg/injection and one delivering 10 mcg/injection. The wrong strength may be dispensed because both pens have similar NDC numbers. Only the final two digits of the NDC numbers are different which may not be read by certain barcode scanning programs. 9 ISMP has received reports that indicate different manufacturers are using identical or very similar product codes (the middle four numbers in the NDC number) for different products. This has resulted in numerous dispensing errors. ISMP receives regular reports of erroneous orders for insulin U-500 instead of the intended U-100. The way insulin products are listed on computerized order-entry screens often causes confusion. Ready access to concentrated insulin increases the likelihood of inadvertent overdose if clinicians are not aware that various concentrations exist. 8 8 January 2008 Organization Assessment Manual double-checks of Byetta products, to include the entire NDC number, are warranted to ensure the correct strength is dispensed, especially in community settings where erroneous dispensing could lead to repeated dosing errors. Scanning inconsistencies Patients who are accustomed to using insulin syringes need to be educated when insulin pen devices are prescribed. Nurses who provide diabetes education, and dispensing pharmacists, should verify the patient understands how to use insulin pen devices and should observe a return demonstration to validate learning. An instructional video describing SoloStar is available at www.ismp.org/sc?k=lantus. Patient confused by insulin pen design Recommendation ActionAgenda Action Required/Assignment ISMP MedicationSafetyAlert! ® Community/Ambulatory Care Edition Evaluate how insulin is listed on order entry and product selection screens. Partner with your software vendor to determine the best way to distinguish insulin products (adding “CONCENTRATED” to U-500 insulin entries has been proposed to major vendors). Consider adding a hard stop on U-500 insulin orders and require prescriber and pharmacist verification before proceeding. Segregate insulin products and ensure that front-line staff knows about the potential for mix-up. Humulin R Concentrate U-500 Pharmacies should: ensure the complete NDC number is used when product selection is verified and include NDC numbers as part of a pre-purchase failure modes and effects analysis when adding new products to stock. NDC Product Codes: The same “middle four” does not mean equal A patient received a three-fold overdose of insulin (which resulted in an emergency department visit) when he misunderstood how to use the SoloStar insulin delivery device. Pen devices may not have features—such as the ability to see the plunger moving—that patients rely on to tell if a dose has been given. Problem 11 Issue No. ISMP AmbulatoryCare July-December 2007 ACAA 2 Date Completed ©2008 ISMP During a patient counseling session, a pharmacist realized that he had nearly dispensed PROGRAF (tacrolimus) instead of PROZAC (fluoxetine). Sound-alike drug names communicated over the telephone contributed to the near-miss. 12 January 2008 A tragic case was reported in the news in which MATULANE (procarbazine), used to treat Hodgkin’s disease, was dispensed to a pregnant woman instead of the ordered prenatal vitamin, MATERNA. Matulane is the only brand name drug in the U.S. that begins with “MAT” so confusion may arise whenever Materna queries are entered into pharmacy systems. HUMIRA PEN (adalimumab) is an existing product used to treat immune-system disorders. A sound-alike product, HUMAPEN, used to administer Lilly’s insulin HUMALOG (lispro injection [rDNA origin]), has been introduced recently. 9 10 A patient reported an error in which he inadvertently administered rapid-acting APIDRA (insulin glulisine [rDNA origin]) instead of the intended long-acting LANTUS (insulin glargine [rDNA origin]). The similar appearance of the vials contributed to the error. Problem 8 Issue No. Organization Assessment ActionAgenda ISMP MedicationSafetyAlert! ® Community/Ambulatory Care Edition Repeating and verifying drug information communicated by telephone may help prevent this type of error. Patient counseling sessions that include reviewing the indication for therapy and the prescribed medication give pharmacists the opportunity to catch errors before harm occurs. Sound-alike names Materna is no longer available in the U.S., but pharmacy personnel should be alert for prescriptions written for this product as it may be considered a generic term for prenatal vitamins. Consider requiring the full drug name (“Matulane”) to be typed into the system before this choice is displayed. Check the indication for new prescriptions with the patient profile or the patient and maximize patient counseling when high-alert drugs are dispensed. Materna – Matulane mix-up Communicate these potentially confused, sound-alike products to frontline pharmacy staff. Before dispensing these drugs and devices, personnel should match the indication for use with the patient’s condition as a double check. Humira Pen and HumaPen ISMP notified sanofi-aventis, the manufacturer of these products, and asked them to investigate ways to better differentiate these insulin products. In the meantime, patients should consider applying a distinctive mark— such a bold black line—to one bottle of similarly packaged insulin products or purchase one product of a look-alike pair from a different manufacturer. Lantus – Apidra Mix-up Recommendation ISMP AmbulatoryCare July-December 2007 Action Required/Assignment ACAA 3 Date Completed ©2008 ISMP A patient reported being very dissatisfied with the way his community pharmacist responded when a dispensing error resulted in nearly 30 days of erroneous therapy. Unfortunately, this pharmacist’s sense of infallibility contributed to the original error, and the perception that she was uncaring impeded an appropriate apology and service recovery actions when the error was discovered. Use of electronically-generated prescriptions may lead to unintended consequences that impair prescribing safety. Problems with misspelled drug names, the use of error-prone abbreviations, and pre-programmed “sigs” that conflict with manually entered special instructions must be addressed. FENTORA (fentanyl transmucosal buccal tablets) use has been linked to serious adverse outcomes when prescribed for patients who are not already opiate-tolerant. Patients must be selected carefully and prescribed doses customized to ensure safe use. 8 12 9 January 2008 An error that could have resulted in a significant harm-causing opioid overdose was reported. The use of “IR” ( to mean immediate release) was added to OPANA (oxymorphone). The pharmacist interpreted the “IR” to be “ER,” the common suffix used to indicate the extended-release product. Problem 7 Issue No. Organization Assessment ActionAgenda Action Required/Assignment ISMP MedicationSafetyAlert! ® Community/Ambulatory Care Edition Prescribers, and pharmacists who double check dosages, are cautioned that mcg-tomcg conversions are not appropriate when converting patients from other fentanyl products, including ACTIQ (fentanyl transmucosal lozenges). FDA and Cephalon issue warnings about FENTORA Pharmacists should communicate deficits— such as trailing zeros, Latin abbreviations, and confusing information—found in electronically-generated prescriptions with prescribers, vendors, and ISMP so we can inform others and advocate for change by vendors. Seeing prescription problems that arise through real-time use of the system allows prescribers to adapt how they use the system and can drive software changes. Electronically-generated prescriptions: An Rx for E-rror? Investigate patient concerns when prescriptions are picked up; use patient counseling sessions as a final check of prescription accuracy. Schools and employers should provide education to pharmacists to ensure they possess requisite knowledge and skills to respond when errors occur. Conveying sympathy, preserving relationships, and fostering trust should be seen as appropriate professional actions in the aftermath of an error. We can do better Prescribers should use a suffix to differentiate a product only when this designation is linked to a specific product and represents the FDA-approved name for the prescribed agent. When confronted with a non-standard or unrecognizable suffix, pharmacists should verify the intended product and dose with the prescriber. Using suffixes where suffixes don’t exist Recommendation ISMP AmbulatoryCare July-December 2007 ACAA 4 Date Completed