Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
PRIDEMARK PARAMEDIC SERVICES
&
DENVER METROPOLITAN
PREHOSPITAL PROTOCOLS
These protocols are effective January 31st, 2008
These protocols are considered property of the Denver Metro EMS Medical Directors and
Pridemark Paramedic Services, LLC. as well as contributors listed below. They may be
utilized and edited by others as long as the Denver Metro EMS Medical Directors and
Pridemark Paramedic Services are credited. We also ask to be notified at: Pridemark
Paramedic Services 6385 W. 52nd Ave. Arvada, CO 80002
Return to Table of Contents
Introduction
At first glance, these protocols appear a bit unusual. They are in that they are a hybrid of
the Denver Metro Protocols that the majority of agencies in our area utilize, Boulder
County Protocols and the Pridemark Protocols.
By allowing the documents to compliment each other, this allows us to practice at the
regional standard as set by the Denver Metro EMS Medical Directors as well as utilize
the protocols that we have developed in house that are specific to the needs of Pridemark.
If you have practiced in the Metro area before coming to Pridemark, much of what you
have utilized still apply, however, you will find some differences in ways that hopefully
will make your job easier.
This document is separated into different sections addressing different items. There are
no page numbers—this is by design to allow easy introduction / retirement of protocols
so the entire book doesn’t need to be printed.
Pridemark specific protocols are noted by a Pridemark Logo in the header area of the
page. In the event of discrepancies or conflicts between the Pridemark and Denver Metro
Protocols, Pridemark protocols are to be followed.
Please remember that it is impossible to write a protocol or guideline to cover every
eventuality. Use good judgment, always act in the patient’s best interest and document
well. Help is only a phone call away.
Return to Table of Contents
PRIDEMARK PREHOSPITAL PROTOCOL MANUAL ACKNOWLEDGEMENT OF
RECEIPT AND PROVIDER PRACTICE EXPECTATIONS
The completed information below verifies that the Pridemark Prehospital Protocol
Manual has been received and that the recipient accepts the responsibility for knowing
and practicing as an EMT and/or paramedic in accordance with these protocols.
______________________________________________________________
Name of Recipient (please print)
Date Received
______________________________________________________________
Signature of Recipient
Date
___________________________________________
Agency
For office and administrative use only:
Protocol Examination Results:
(90% or higher required to pass on all tests)
Mapping and Radios:
______________________________________________________________________
Combination Analgesia:
______________________________________________________________________
Cardiology:
______________________________________________________________________
Operations:
______________________________________________________________________
Final Protocol Test:
______________________________________________________________________
Notes:
_____________________________________________________________________
______________________________________________________________________
______________________________________________________________________
Return to Table of Contents
ACKNOWLEDGEMENTS
This version of the Denver Metro Emergency Medical Services Medical Directors
protocols has been produced based on previous protocols produced by the following.
The Denver Metropolitan Physician Advisor Group
Mark Kozlowski, M.D.
F. Keith Battan, M.D.
Donald Massey, D.O.
Christopher Colwell, M.D.
David McArdle, M.D.
James Cusick, M.D.
Gilbert Pineda, M.D.
Eugene Eby, M.D.
John Riccio, M.D.
James Hogan, M.D.
Ray Rossi, M.D.
Benjamin Honigman, M.D.
W. Peter Vellman, M.D.
Arthur Kanowitz, M.D.
Ron Keller, M.D.
Special thanks and recognition to:
Mike Armacost, MS, EMT-P
Eric Bettinger, EMT-P
Michael Bilo, EMT-P
Marilyn Bourn, RN, MSN, EMT-P
Colleen Bruntz
Thomas Candlin, III, EMT-P
Jami Mari Cavos
Anne Clouatre, MHS, EMT-P
Jim Cloud
Tracy Collins, RN
Ray Coniglio, RN
Brian Daley, EMT-P
David Day, EMT-P
Jean Distretti
Jeff Fletcher, BS, EMT-P
Douglas Frosh, BS, EMT-P
John Glenn, EMT-P
Craig Gravitz, RN, EMT-P
Garet Hickman, EMT-P
Carol Hurdelbrink, RN
Carol Jenks
Jacob Johnson, EMT-P
Kathee Johnson
Timothy Keane, EMT-P
Wilson Lindquist
Rick Lindsey, EMT-P
Robert Marlin, EMT-P
Kathy Mayer, RN, MSN
Bill Mayfield, RN
Ron McCuiston
Lee Meyer, B.S., EMT-P
David Patterson, EMT-P
Randy Pennington, EMT-P
Scott Phillips, EMT-P
Lorna Prutzman
Ron Quaife, RN, EMT-P
Joe Rockwell, EMT-P
David Sanko, BA, EMT-P
Mike Shabkie, EMT-P
Bill Spialek, EMT-P
Tracy Thomas, EMT-P
Thomas Tkach, EMT-P
Ted Hockenberry, EMT-P
Patricia Tritt, RN, MS
Ted Vargas
Sam Walters
Danny Willcox, EMT-P
Jean Zambrano, EMT-P
These protocols have been developed specifically for the Denver metropolitan
community. They represent consensus amongst all of the Denver metropolitan EMS
agency Medical Directors. The protocols express a commitment to a consistent
approach to quality patient care.
Return to Table of Contents
The process that has been initiated in the construction of this revised set of metro-wide
protocols will remain in place. The authors will continue to edit and revise the protocols
Dedicated to Carol J. Shanaberger, Esq., EMT-P. May her memory be eternal.
Acknowledgments
The process behind managing protocols is a daunting one in that the document is truly
living. What may be standard-of-care today could possibly be extinct as early as
tomorrow. Many people have spent hundreds of hours on protocol development and
maintenance. The following people are thanked in the first version of the Pridemark
Protocols:
Christina Crumpecker, EMT-Paramedic
Arthur Kanowitz, MD FACEP
Jeff Flasschoen, EMT-Paramedic
along with the Protocol Development committee:
Tori Ainlay, EMT
Bruce Amdahl, EMT-Paramedic
Chantel Benish, EMT-Paramedic
Matthew Bergland, EMT-Paramedic
Ray Bondi, EMT-Paramedic
Jamie Bosten, EMT-Paramedic
Christopher Carleton, EMT-Paramedic
Alice “Twink” Dalton, RN EMT-Paramedic
Julia Davis, EMT
Eammonn Dolan, EMT-Paramedic
Bryan DeWolfe, EMT-Paramedic
Cameron Duran, EMT-Paramedic
Sarah Duran, EMT
Simon Edwards, PA-C
Pam Evans, EMT-Paramedic
David Fending, EMT-Paramedic
Wes Filener, EMT-Paramedic
Chris Galton, EMT-Paramedic
Faith Goodrich, EMT-Paramedic
Robert Greenlee, EMT-Paramedic
Terry Halford, EMT-Paramedic
Bryan Handwork, EMT-Paramedic
Chris Hendricks, EMT-Paramedic
Hollis Hopkins, EMT-Paramedic
Megan Huffman, EMT-Paramedic
Scott Kittredge, EMT-Paramedic
Steve Koniezny, EMT-Paramedic
Pam Howes, EMT-Paramedic
Paul Johnson, EMT-Paramedic
Brendan Kelly, EMT_Paramedic
William H. Kraft, EMT-Paramedic
Chris Mulberry, EMT-Paramedic
Melissa Lunt, EMT-Paramedic
Return to Table of Contents
Chris Naig, EMT-Paramedic
Thomas F. Pedigo, PA-C
David Pace, EMT-Paramedic
Table of Contents
I.
II.
III.
IV.
V.
Introduction
Confidentiality / HIPAA
Consent
Physician on scene
DNR/ Advanced Directives
Protocol
Number
1000
Protocol Title
Airway
Go to Table of Contents
Last Revision Date
4012
4013
4014
4020
4030
4031
4040
4050
4051
4052
4053
4054
4055
4056
4060
4070
4080
4090
Coma
Seizure
Syncope
Allergies & Anaphylaxis
Abdominal (including GI/GU)
Vomiting
Poisoning & Overdose
Environmental
High Altitude
Drowning/Near Drowning
Cold Emergencies
Heat Emergencies
Bites & Stings/ Snake Bites
Snake Bites
Shock-Medical
Psychiatric/ Behavioral Emergencies
Obstetrics/ Gynecological Emergencies
Excited Delirium
5000
5010
5020
5030
5040
5050
5055
5060
5070
5080
5090
5100
5200
SOP
Trauma
Trauma Arrest
Amputations
Head Trauma
Face & Neck Trauma
Spinal Trauma
Selective Spinal Immobilization
Chest Injury
Abdominal Trauma
Extremity Injuries
Burns
Taser
Boulder Specific Trauma Activation Criteria
Tourniquet Procedure
6000
6010
6020
6030
6040
6050
7000
7010
7020
7030
General Guidelines for Pediatrics
Infant and Child Resuscitation
Sudden Infant Death Syndrome
Pediatric Dehydration
Pediatric Respiratory Distress
Pediatric Seizures
Pharmacology. Medication Administration
Medication Administration
Medication Administration (Parental)
Medications
Adenosine (Adenocard)
Albuterol Sulfate (Proventil, Ventolin)
Amiadorone (Cordarone)
Aspirin
Atropine Sulfate
Diltiazem (Cardizem)
Dextrose
Return to Table of Contents
Located with SOP’s
Diazepam (Valium)
Diphenhydramine (Benadryl)
Dopamine (Intropin)
Epinephrine (Adrenalin)
Epinephrine Auto-Injector (Epi-pen, Epi-pen Jr.)
Fentanyl
Furosemide (Lasix)
Glucagon
Haloperidol (Haldol)
Ipratropium Bromide (Atrovent)
IV Solutions
Lidocaine 2% Solution
Lidocaine Gel (Xylocaine)
Magnesium Sulfate
Mark I Nerve Agent Antidote Kit
Metered Dose Inhaler (MDI)
Methylprednisolone (Solu-Medrol)
Midazolam (Versed)
Morphine Sulfate
Naloxone (Narcan)
Nitroglycerine (Nitrostat, Nitroquick, etc.)
Ondansetron (Zofran)
Oral Glucose (Glutose, Insta-Glucose)
Oxygen
Phenylephrine (Intranasal)
Promethazine (Phenergan)
Racemic Epinephrine (Vaponephrine)
Sodium Bicarbonate
Topical Ophthalmic Anesthetics
Interfacility Transfer
Formulary Protocols
8000
Procedures
Procedures
Procedures
Procedures
Procedures
Procedures
Procedures
Procedures
Procedures
Procedures
Procedures
Procedures
Procedures
Antibiotics
Heparin Drip
Nitro Drip
System Specific Medical Procedures &
Operations Guidelines
Bandaging
Capnography
Cardioversion
Combination Analgesia
Continuous Positive Airway Pressure (CPAP)
Field Drawn Blood Samples
Blood Draw for Law Enforcement
Percutaneous Cricothyrotomy
Pneumatic Anti-Shock Garment (PASG)
Restraints
Splinting: Axial
Splinting: Extremity
Tension Pneumothorax: Needle Decompression
Return to Table of Contents
Procedures
Procedures
Procedures
Procedures
Procedures
Procedures
Transcutaneous Cardiac Pacing
Transport of the Handcuffed Patient
Vascular Access Devices
Venous Access Technique-General Principle
Venous Access Technique-Saline Lock
Vascular Access Technique-External Jugular
Vein
Procedures
Venous Access Technique-Extremity
Procedures
Venous Access Technique-Intraosseous
Infusion
Assessment
Assessment/ MOI
Assessment
History
Assessment
Documentation
Assessment
Commonly Accepted Abbreviations
Operations
Combined Advanced Directives
Operations
Communication
Operations
Destination Policy
Operation
Destination Policy: Divert
Operations
Incident Command System
Operations
START Triage
Operations
Hazardous Materials / WMD
Operations
Infectious Diseases
Operations
Non-Transport of Patients
Operations
Non-Transport of Patients: Refusals
Operations
Non-Transport of Patients: Field
Pronouncements
Miscellaneous Lab Values
Miscellaneous 12-Lead EKG Landmarks & Infarct Patterns
9000
Pridemark Paramedic Services
Clinical SOP’s
SOP
SOP
SOP
SOP
SOP
SOP
SOP
SOP
SOP
SOP
BLS Transport
Certification Requirement
QA/QI Guidelines
Protocol Violations
Narcotic Storage and Administration
FI Process
Paramedic School Sponsorship
Firefighter or Emergency Event Rehab
Pridemark TB Screening Policy/Procedure
Disposition of ETOH Patients
Return to Table of Contents
INTRODUCTION
The following PROTOCOLS define the rules of medical care by EMS Providers. These
protocols delineate the expected practice, actions and procedures of EMS providers in
the field. They have been developed in conjunction with and are sanctioned by the
Denver Metro EMS Medical Directors (DMEMSMD). Deviation from the protocols is
occasionally necessary due to the vast array of complex clinical presentations. It should
always be done with the patient’s best interest in mind and backed with documentable
and defendable clinical reasoning and judgment.
When protocol variance occurs it should be approached in a logical and knowledgeable
manner, done in the best interests of the patient, and well documented. In essence it
should be done “in good faith.” Deviation from standing order protocols should be done
with the support of online medical control and/or reported to the agency’s Medical
Director for offline medical control and review.
The prehospital protocols are categorized in accordance with the National Standard
curriculum and further broken down by sub-categories within a section.
Advanced procedures are those techniques that require physician direction in teaching,
skill maintenance, and use. Some procedures are suitable for a standing order while
others are categorized as a direct order that requires base contact. A number of
treatment, medication, procedure, and operational guidelines protocols require base
contact for specific circumstances. A list of protocols that require base contact can be
found in the appendix.
Please remember that protocols define process; people provide care.
PROTOCOL KEY
The following symbols denote assessments and treatments that are limited to a certain
level of prehospital provider:
IV
P
EMT with IV certification
Paramedic
Advanced Practice Paramedic
The following symbol denotes assessments and treatments that are specific to
prehospital pediatric care.
Pediatric Care
Go to Table of Contents
CONFIDENTIALITY
A. The patient-physician relationship, the patient-registered nurse relationship, and
the patient-EMT relationship are recognized as privileged. This means that the
physician, nurse, or EMT may not testify as to confidential communications
unless:
• the patient consents or
• the disclosure is allowable by law (such as Medical Board or Nursing Board
proceedings, or civil litigation in which the patient's medical condition is in
issue)
B. The patient's medical information must be kept confidential by the prehospital
provider as private information in medical care. The patient likely has an
expectation of privacy and trusts that personal, medical information will not be
disclosed by medical personnel to any person not directly involved in the patient's
medical treatment.
Exceptions
A. The patient is not entitled to confidentiality of information that does not pertain to
the medical treatment, medical condition, or is unnecessary for diagnosis or
treatment.
B. The patient is not entitled to confidentiality for disclosures made publicly.
C. The patient is not entitled to confidentiality with regard to evidence of a crime.
Additional Considerations
A. Any disclosure of medical information should not be made or allowed unless
necessary for the treatment, evaluation or diagnosis of the patient.
B. Any disclosures made by any person, medical personnel, the patient, or law
enforcement should be treated as limited disclosures and not authorizing further
disclosures to any other person.
C. Any discussions of prehospital care by and between the receiving hospital, the
crew members in attendance, or at in-services or audits are done strictly for
educational purposes. Further disclosures are not authorized.
D. Radio communications should not include disclosure of patient names.
E. This procedure does not preclude or supersede your agency’s HIPAA policy and
procedures.
Go to Table of Contents
CONSENT
General Principles: Adults
A. An adult in the State of Colorado is 18 years of age or older.
B. Every adult is presumed capable of making medical treatment decisions. This
includes the right to make "bad" decisions that the prehospital provider believes
are not in the best interests of the patient.
C. A person is deemed to have decision-making capacity if he/she has the ability to
provide informed consent, i.e., the patient:
1. Understands the nature of the illness/injury or risk of injury/illness;
2. Understands the possible consequences of delaying treatment/refusing
transport; and
3. Given the risks and options, the patient voluntarily refuses or accepts
treatment/transport.
D. A call to 9-1-1 itself does not prevent a patient from refusing treatment. A patient
may refuse medical treatment (IVs, oxygen, medications), but you should try to
inform the patient of the need for therapies, offer again, and treat to the extent
possible.
E. The odor of alcohol on a patient’s breath does not, by itself, prevent a patient
from refusing treatment. Refer to letter C above.
F. Implied Consent: An unconscious adult is presumed to consent to treatment for
life-threatening injuries/illnesses.
G. Involuntary Consent: In rare circumstances, consent may be authorized by a
person other than the patient (such as a court order [guardianship], from a peace
officer for prisoners in custody or detention, and persons under a mental health
hold or commitment who are a danger to themselves or others or are gravely
disabled).
Procedure: Adults
A. Consent may be inferred by the patient's actions or by express statements. If
you are not sure that you have consent, clarify with the patient or CONTACT
BASE. This may include consent for treatment decisions or transport/destination
decisions.
B. Determining whether or not a patient has decision-making capacity to consent or
refuse medical treatment in the prehospital setting can be very difficult. Every
effort should be made to determine if the patient has decision-making capacity,
as defined above under C.
C. For patients who do not have decision-making capacity, CONTACT BASE.
D. If the patient lacks decision-making capacity and the patient's life or health is in
danger, and there is no reasonable ability to obtain the patient's consent,
proceed with transport and treatment of life-threatening injuries/illnesses. If you
are not sure how to proceed, CONTACT BASE.
E. For patients who refuse medical treatment.
F. If you are unsure whether or not a situation of involuntary consent applies,
CONTACT BASE.
Go to Table of Contents
General Principles: Minors
A. A parent, including a parent who is a minor, may consent to medical or
emergency treatment of his/her child. There are exceptions:
1. Neither the child nor the parent may refuse medical treatment on religious
grounds if the child is in imminent danger as a result of not receiving
medical treatment, or when the child is in a life-threatening situation, or
when the condition will result in serious handicap or disability.
2. The consent of a parent is not necessary to authorize hospital or
emergency health care when an EMT-P in good faith relies on a minor's
consent, if the minor is at least 15 years of age and emancipated or
married.
3. Minors may seek treatment for abortion, drug addiction, and venereal
disease without consent of parents. Minors > 15 years may seek
treatment for mental health.
B. When in doubt, your actions should be guided by what is in the minor's best
interests and base contact.
Procedure: Minors
A. A parent or legal guardian may provide consent to or refuse treatment in a nonlife-threatening situation.
B. When the parent is not present to consent or refuse:
1. If a minor has an injury or illness, but not a life-threatening medical
emergency, you should attempt to contact the parent(s) or legal guardian.
If this cannot be done promptly, transport.
2. If the child does not need transport, they can be left at the scene in the
custody of a responsible adult (e.g., teacher, social worker, grandparent).
It should only be in very rare circumstances that a child of any age be left
at the scene if the parent is not also present.
3. If the minor has a life-threatening injury or illness, transport and treat per
protocols. If the parent objects to treatment, CONTACT BASE
immediately and treat to the extent allowable, and notify police to respond
and assist.
Return to Table of Contents
PHYSICIAN AT THE SCENE/MEDICAL DIRECTION
Purpose
A. To provide guidelines for prehospital personnel who encounter a physician at the
scene of an emergency
General Principles
A. The prehospital provider has a duty to respond to an emergency, initiate
treatment, and conduct an assessment of the patient to the extent possible.
B. A physician who voluntarily offers or renders medical assistance at an
emergency scene is generally considered a "Good Samaritan." However, once a
physician initiates treatment, he/she may feel a physician-patient relationship has
been established.
C. Good patient care should be the focus of any interaction between prehospital
care providers and the physician.
Procedure
See algorithm.
Special notes
A. Every situation may be different, based on the physician, the scene, and the
condition of the patient.
B. CONTACT BASE when any question(s) arise.
NOTE TO PHYSICIANS ON INVOLVEMENT WITH EMTs
THANK YOU FOR OFFERING YOUR ASSISTANCE.
The prehospital personnel at the scene of this emergency operate under standard
policies, procedures, and protocols developed by their physician advisor. The drugs
carried and procedures allowed are restricted by law and written protocols.
After identifying yourself by name as a physician licensed in the State of Colorado and
providing identification, you may be asked to assist in one of the following manners:
1. Offer your assistance or suggestions, but the prehospital care providers will
remain under the medical control of their base physician or
2. With the assistance of the prehospital care providers, talk directly to the base
physician and offer to direct patient care and accompany the patient to the
receiving hospital. Prehospital care providers are required to obtain an order
directly from the base physician for this to occur.
THANK YOU FOR OFFERING YOUR ASSISTANCE DURING THIS EMERGENCY.
Medical Director
Go to Table of Contents
Agency
PHYSICIAN AT THE SCENE/MEDICAL DIRECTION ALGORITHM
EMT arrives on scene
EMS attempts patient care
Physician reports on patient.
Relinquishes patient care.
Physician wants to help or is
involved in patient care and will
not relinquish patient care
Provide care per protocol
Prehospital provider identifies
self and level of training
Physician wishes to just help
out
Physician requests or performs
care inappropriate or
inconsistent with protocols
Provide general instructions
and utilize physician assistance
Prehospital care provider shares
Physician at the Scene/Medical
Direction note with physician.
Advise physician of your
responsibility to patient
Physician does not relinquish
patient and continues care
inconsistent with protocols
Contact base physician
Physician complies
Continue per patient protocol
Follow base physician’s
direction
Document patient care on run report.
Document difficulties or problems on the unusual circumstance report.
Return to Table of Contents
RESUSCITATION AND FIELD PRONOUNCEMENT GUIDELINES
Purpose
A. To provide guidelines for resuscitation and field pronouncement of patients in
cardiac arrest in the prehospital setting
General Principles
A. Agency policy determines base contact requirements for patients for whom
resuscitative efforts are being withheld.
B. All patients found pulseless and apneic are to be resuscitated, except patients
found in any of the following conditions:
1. Decapitation or
2. Decomposition or
3. Third degree burns over more than 90% of the total body surface area or
4. Dependent lividity or rigor mortis or
5. A valid CPR directive present with the patient or
6. Evidence of massive blunt head, chest, or abdominal trauma
Special Considerations in Resuscitation Decisions:
A. All cases described below require contact with a base physician to approve
termination of treatment.
1. Blunt Trauma: Resuscitative efforts may be withheld or terminated in patients
found apneic and pulseless with:
a. Blunt trauma to the head, neck or torso; and
b. No spontaneous pulse or respirations following appropriate medical
interventions, which include, for example: ensuring a patent airway or
chest decompression. (The majority of injuries sustained by these
patients are not compatible with life. "Appropriate" interventions will
vary and should be dictated by guidance from the base.)
2. Penetrating Trauma:
a. Research data shows that a significant number of victims of
penetrating trauma to the neck or torso, who are found without signs
of life, may be successfully resuscitated. Therefore, resuscitation and
rapid transport to a trauma facility should be initiated on all patients
found in full arrest secondary to penetrating trauma. Exceptions may
exist in the following circumstance:
i. Patients found pulseless and apneic with penetrating trauma if
the provision of ALS (EMT-Intermediate or EMT-Paramedic or
emergency department) has been unavailable for at least 10
minutes from the time EMS personnel initiate on-scene
assessment. (Some of the injuries sustained by these patients
may be compatible with life. "Appropriate" interventions will
vary and should be dictated by guidance from the base
physician.)
ii. However, if there is any doubt about duration of the arrest,
then resuscitation and rapid transport should be initiated.
3. Medical Patients (i.e., no evidence of trauma and presumed medical arrest)
should receive resuscitative treatment until there is:
Go to Table of Contents
a. No return of spontaneous pulse or respirations during 15 minutes of
CPR (after successful intubation and medications) and no reversible
causes have been identified; or
b. Continuous asystole for at least 10 minutes in the adult patient, and
30 minutes in a pediatric patient (after successful intubation and
medications), and no reversible causes have been identified
c. The following patients found pulseless and apneic warrant
resuscitation efforts beyond 30 minutes and should be transported:
i. Hypothermic; or
ii. Drowning with submersion less than 60 minutes (with
hypothermia); or
iii. Pregnant and estimated to be 20 weeks or later in gestation
4. After pronouncement, do not alter condition in any way or remove equipment
(lines, tubes, etc.) as the patient is now a potential coroner’s case.
Advance Medical Directives
A. There are several types of advance medical directives (documents in which a
patient identifies the treatment to be withheld in the event the patient is unable to
communicate or participate in medical treatment decisions).
B. Do not resuscitate (DNR) orders are generally intended to be written by a
physician for a patient whose medical condition is such that commencement of
resuscitation efforts would be futile.
C. A Colorado living will ("Declaration as to Medical or Surgical Treatment") requires
a patient to have a terminal condition, as certified in the patient's hospital chart by
two physicians. For the document to become operative, the patient must be
unresponsive because of a terminal condition for a period of seven days.
D. Other types of advance directives may be a "Durable Medical Power of Attorney,"
or "Health Care Proxy" (the CPR Directive is covered separately. Each of these
documents can be very complex and require careful review and verification of
validity and application to the patient's existing circumstances. Therefore, the
consensus is that resuscitation should be initiated until a physician can review
the document or field personnel can discuss the patient’s situation with the base
physician.
E. Resuscitation may be withheld from or terminated for a patient who has a valid,
written do not resuscitate order or other advance medical directive.
1. The document is clear, unequivocally to the prehospital provider that CPR,
intubation and defibrillation are refused by the patient or by the patient's
attending physician who has signed the document; and
2. Base physician has approved of withholding or ceasing resuscitative efforts;
and
3. There is no apparent indication of suicidal gesture or intent by the patient.
F. If there is disagreement at the scene about what should be done, the base
should be contacted immediately for guidance.
G. Prehospital providers presented with equivocal DNR orders or advance medical
directives should proceed with resuscitation and establish base contact for
guidance on treatment and transport.
1. If the directive document is long and detailed, then it is probably more
reasonable for resuscitation to be initiated and the patient to be transported
so that the base physician can review the document and possibly contact the
patient's attending physician.
Return to Table of Contents
2. The duration of the resuscitation should be guided by the same factors of any
medical cardiac arrest.
H. Verbal DNR "orders" are not to be accepted by the prehospital provider. In the
event family or an attending physician directs resuscitation be ceased, the
prehospital provider should immediately CONTACT BASE. The prehospital
provider should accept verbal orders to cease resuscitation only from the base
physician.
I. There may be times in which the prehospital provider feels compelled to perform
or continue resuscitation, such as a hostile scene environment, family members
adamant that "everything be done," or other highly emotional or volatile
situations. In such circumstances, the prehospital provider should attempt to
confer with the base for direction and if this is not possible, the prehospital
provider must use his or her best judgment in deciding what is reasonable and
appropriate, including transport, based on the clinical and environmental
conditions, and establish base contact as soon as possible.
Additional Considerations:
A. Mass casualty incidents are not covered in detail by these guidelines. (See
Colorado State Unified Disaster Tag and Triage System: A Guide to MCI).
B. These guidelines apply to both adult and pediatric patients.
C. If the situation appears to be a potential crime scene, EMS providers should
disturb the scene as little as possible.
D. ALS personnel should document asystole for 10 seconds in at least two leads
prior to withholding or terminating resuscitative efforts. However, base
physicians and prehospital providers must use discretion when considering the
need for a rhythm strip (i.e., monitor strips are not necessary in patients found
decapitated, decomposed or with dependent lividity or rigor mortis).
E. Mechanism for disposition of bodies by means other than EMS providers and
vehicles should be prospectively established in each county or locale.
1. In all cases of unattended deaths occurring outside of a medical facility, the
coroner should be contacted immediately.
2. Patients with valid DNR orders or advance medical directives should receive
medical treatment and supportive or comfort care prior to cardiac arrest.
Return to Table of Contents
1000
AIRWAY & VENTILATION
GENERAL PRINCIPLES
The following protocols are recommended as a guide for approaching difficult medical
and trauma airway problems. They assume that the responder is skilled in the various
procedures, and will need to be modified according to training level. Advanced
procedures should only be attempted if simpler ones fail and if the technician is qualified.
Individual cases may require modification of these protocols.
All patients require continuous monitoring of their airways to ensure airway patency.
Wherever the term "Monitor airway" is used throughout these protocols, the following
elements shall be utilized:
• Position of the patient's head
• Need for airway adjuncts
• Need for oropharyngeal suctioning;
• Need for Advanced Life Support airway management techniques
• Use of Pulse Oximetry (SpO2), if available
• Use of secondary form of Endotracheal Tube confirmation (Example: End Tidal
Capnography (ETCO2). Secondary confirmation devices are not a substitute for
primary confirmation techniques that rely upon direct visualization and
auscultation, but serve as an additional method of documenting proper
endotracheal tube placement.
Definitions
Respiratory distress – Signs and symptoms may include increased respiratory effort,
peripheral cyanosis, tachypnea, accessory muscle use, anxiety and adventitious lung
sounds upon auscultation.
Respiratory insufficiency/failure – signs and symptoms include the above with central
cyanosis and insufficient air exchange, tiring, and inability to speak in complete
sentences.
Pediatric respiratory distress is characterized by increased respiratory effort with
peripheral cyanosis, i.e. anxiety, tachypnea, nasal flaring and intercostal retractions.
Respiratory failure in a child is characterized by ineffective respiratory effort with central
cyanosis, i.e. agitation or lethargy, severe dyspnea or labored breathing, bobbing or
grunting, and marked intercostal and parasternal retractions.
Use appropriate airway adjuncts as indicated – These are devices that are approved for
the level of the provider and by the agency’s Medical Director.
NOTE: Bradycardia is an ominous sign that indicates hypoxic cardiac arrest may be
imminent
Go to Table of Contents
METHODS OF OPENING THE AIRWAY
HEAD TILT-CHIN LIFT:
Technique: From beside head, place one hand on forehead. Grasp lower edge of
chin with fingers of other hand and lift chin forward. Teeth may come
together.
Indications: Medical patient. May require less neck extension than head tilt. Useful
with dentures. May be used without head tilt in trauma victims.
JAW THRUST:
Technique: Position yourself above patient. Place fingers of each hand under angle
of jaw, just below ears. Lift jaw, using forearms to maintain head
alignment.
Indications: Trauma victim or medical patient, where neck extension is not possible.
Another rescuer must do BVM ventilation, and this is a fatiguing method.
May be used with dentures in place.
Providers are reminded that aggressive treatment is indicated for better outcomes.
Return to Table of Contents
1010
OBSTRUCTED AIRWAY
Indications
A. Complete or partial obstruction of the airway due to a foreign body.
B. Complete or partial obstruction due to airway swelling from anaphylaxis, croup,
or epiglottitis.
C. Patient with unknown illness or injury who cannot be ventilated after procedures
of previous protocol: Opening the Airway.
Precautions
A. Perform chest thrusts only in visibly pregnant patients, obese patients, and in
infants.
B. Patients with partial airway obstruction can be very uncomfortable and
vociferous. Abdominal or chest thrusts will not be effective and may cause injury
to the patient who is still breathing. Be ready to intervene promptly if arrest
occurs.
C. Hypoxia from airway obstruction can cause seizures. Chest or abdominal thrusts
may not be effective until the patient becomes relaxed after the seizure is over.
Technique
A. COMPLETE AIRWAY OBSTRUCTION:
1. Open airway using head tilt-chin lift or jaw thrust.
2. Attempt to ventilate using BVM ventilations or mouth to mask.
3. If unable to ventilate, reposition airway and reattempt ventilations.
4. If airway remains obstructed, visualize with laryngoscope and remove any
obvious foreign body.
IN
5. If unable to ventilate, administer 5 subdiaphragmatic abdominal thrusts.
6. Reposition the airway and reattempt to ventilate.
7. Consider percutaneous cricothyrotomy if obstruction is above the cords
unrelieved or unusable to ventilate adequately with bag-valve. See Appendix
for more information.
P
8. When obstruction is relieved:
a. Keep patient on side, sweeping airway to remove debris.
b. Administer high flow oxygen via reservoir mask.
c. Assess adequacy of ventilation, and support as needed.
d. Suction aggressively.
e. Restrain if combative
.
B. PARTIAL AIRWAY OBSTRUCTION:
1. Have patient assume most comfortable position.
2. Administer high flow oxygen by non-rebreather mask.
3. Attempt suctioning of upper airway.
4. If patient is unable to move air, confused, or otherwise deteriorating, visualize
airway, remove foreign body or perform abdominal thrusts as noted above.
Go to Table of Contents
Complications
A. Hypoxic brain damage and death from unrecognized or unrelieved obstruction.
B. Trauma to ribs, lung, liver and spleen from chest or abdominal thrusts
(particularly when forces are not evenly distributed).
C. Vomiting and aspiration after relief of obstruction.
D. Creation of complete obstruction after blind incorrect finger probing.
E. Tonsillar or pharyngeal laceration from over vigorous finger sweep.
Return to Table of Contents
1020
CLEARING AND SUCTIONING THE AIRWAY
Indications
A. To remove foreign material that can be removed by a suction device.
B. To remove excess secretions or pulmonary edema fluid in upper airway or lungs
(with endotracheal tube in place).
C. To remove meconium or amniotic fluid in mouth, nose and oropharynx of
newborn
Technique
A. Turn patient on side if possible, to facilitate clearance.
B. Open airway and inspect for visible foreign material.
C. Remove large or obvious foreign matter with gloved hands. Use padded tongue
blade or oropharyngeal airway (do not pry) to keep airway open. Sweep finger
across posterior pharynx and clear material out of mouth.
D. Suction of oropharynx:
1. Attach tonsil tip (or use open end for large amounts of debris).
2. Ventilate and oxygenate the patient as needed prior to the procedure.
3. Insert tip into oropharynx under direct vision, with sweeping motion.
4. Continue intermittent suction interspersed with active oxygenation by mask or
cannula. Use positive pressure ventilation if needed.
IN
E. Catheter suction of endotracheal tube:
1. Hyperventilate patient prior to any suctioning attempts.
2. Put on sterile gloves.
3. When catheter tip has been gently advanced as far as possible, apply suction
and withdraw catheter slowly.
NOTE: Suctioning should only done with a sterile catheter.
4. Rinse catheter tip in sterile water or saline.
5. Administer oxygen appropriately following suctioning.
F. Suction of the newborn:
1. Use neonatal suctioning device.
2. As soon as infant's head has delivered, insert suction tip into the mouth and
back to oropharynx.
3. Apply suction while slowly withdrawing catheter from the mouth.
4. Insert catheter tip into each nostril and back to posterior pharynx.
5. Apply suction while slowly withdrawing catheter from each nostril.
6. As soon as infant has delivered, repeat process.
IN
G. Suction trachea under direct vision with laryngoscope if there is evidence of
meconium aspiration.
Complications
A. Hypoxia due to excessive suctioning time without adequate ventilation between
attempts.
B. Persistent obstruction due to inadequate tubing size for removal of debris.
C. Lung injury from aspiration of stomach contents due to inadequate suctioning.
D. Asphyxia due to recurrent obstruction if airway is not monitored after initial
suctioning.
E. Conversion of partial to complete obstruction by attempts at airway clearance.
F. Trauma to the posterior pharynx from forced use of equipment.
Go to Table of Contents
G. Vomiting and aspiration from stimulation of gag reflex.
H. Induction of cardio-respiratory arrest from Vagal Nerve stimulation.
Side Effects and Special Notes
A. Complications may be caused both by inadequate and overly vigorous
suctioning. Technique and choice of equipment are very important. Choose
equipment with enough power to suction large amounts rapidly to allow time for
ventilation.
B. Proper airway clearance can make the difference between a patient who survives
and one who dies. Airway obstruction is one of the most common treatable
causes of prehospital death.
Return to Table of Contents
1030
ASSISTING VENTILATION
Indications
A. Inadequate patient ventilation due to fatigue, coma, or other causes of respiratory
depression.
B. To apply positive pressure ventilation in patients with pulmonary edema and
severe fatigue.
C. To ventilate patients in respiratory arrest.
Precautions
A. Two people are often required to obtain an adequate mask fit and also ventilate.
B. Assisted ventilation will not hurt a patient, and should be used whenever the
breathing pattern seems shallow, slow, or otherwise abnormal. Do not be afraid
to be aggressive about assisting ventilation, even in patients who do not require
or will not tolerate intubation.
C. Early intubation may be of benefit for patients who continue to bleed or vomit.
Technique
A.
B.
C.
D.
E.
Open the airway. Check for ventilation.
Administer ventilations. If unsuccessful, go to Airway Obstruction protocol.
Check pulse. If absent, go to Cardiac Arrest protocol.
Attach oxygen to BVM.
Position yourself above patient's head, continue to hold airway position, seat
mask firmly on face, and begin assisted ventilation.
F. Watch chest for rise, and feel for air leak or resistance to air passage. Adjust
mask fit as needed.
G. If patient resumes spontaneous respirations, continue to administer supplemental
oxygen. Intermittent assistance with ventilation may still be needed.
H. Continuous monitoring of pulse oximetry is required.
I. Use Capnography, if available.
Complications
A. Continued aspiration of blood, vomitus, and other upper airway debris
B. Inadequate ventilations due to poor seal between patient's mouth and ventilatory
device
C. Gastric distention, possibly causing vomiting
D. Trauma to the upper airway from forcible use of airways
E. Pneumothorax
Go to Table of Contents
IN
1040
OROTRACHEAL INTUBATION
P
Indications
A. In most cases orotracheal intubation provides definitive control of the airway. Its
purposes include:
1. Actively ventilating the patient
2. Delivering high concentrations of oxygen
3. Suctioning secretions and maintaining airway patency
4. Preventing aspiration of gastric contents, upper airway secretions, or
bleeding
5. Preventing gastric distention due to assisted ventilation
6. Administering positive pressure when extra fluid is present in alveoli
7. Allowing more effective CPR
8. Administering drugs during resuscitation for absorption through the lungs as a
last resort.
Precautions
A. Do not use intubation as the initial method of managing the airway in an arrest.
Oxygenation prior to intubation should be accomplished with pocket mask or
BVM as needed.
B. Appropriate intubation precautions should be taken in the trauma patient.
Nasotracheal intubation is preferred in the breathing patient. Oral intubation with
in-line cervical immobilization is the best alternative for a trauma patient requiring
definitive airway control.
C. Never lever the laryngoscope against the teeth. The jaw should be lifted with
direct upward traction by the laryngoscope.
D. Prepare suction beforehand. Vomiting is particularly common when the
esophagus is intubated.
E. Intubation should take no more than 20 seconds to complete: do not lose track
of time. If visualization is difficult, stop and re-ventilate before trying again.
F. Orotracheal intubation can be accomplished in trauma victims if an assistant
maintains stabilization and keeps the neck in neutral position. Careful
visualization with the laryngoscope is needed, and McGill forceps may be helpful
in guiding the ET tube.
G. If the patient presents with a difficult airway or difficulties are expected then use
of OTHER AIRWAY DEVICES may be preferable to intubation.
Technique
A. Use BSI including gloves, mask, eye protection. Assemble the equipment while
continuing ventilation:
1. Choose tube size (see table on next page). Use the largest tube available.
2. Introduce the stylette and be sure it stops ½” short of the tube’s end.
3. Assemble laryngoscope and check light.
4. Connect and check suction.
B. Position patient: neck flexed forward, head extended back. Back of head should
be level with or higher than back of shoulders.
C. Give a minimum of 4 good ventilations before starting procedure.
D. Have an assistant apply gentle cricothyroid pressure to prevent aspiration and to
assist in visualization of vocal cords.
E. Gently insert laryngoscope to right of midline. Move it to midline, pushing tongue
to left and out of view.
Go to Table of Contents
F. Lift straight up on blade (no levering) to expose posterior pharynx.
G. Identify epiglottis: tip of curved blade should sit in vallecula (in front of epiglottis);
straight blade should slip over epiglottis.
H. With gentle further traction to straighten the airway, identify trachea from
arytenoid cartilages and vocal cords.
I. Insert tube from right side of mouth, along blade into trachea under direct vision.
J. Advance tube so cuff is 1-1½" beyond cords. Inflate cuff with 5-10 ml of air,
clamp if necessary to secure against leaks.
K. Ventilate and watch for chest rise. Listen for breath sounds over stomach
(should not be heard), lungs and axillae.
L. Note proper tube position and secure tube with tape or ties.
M. Re-auscultate over stomach and both sides of chest whenever patient is moved.
N. End tidal CO2 colormetric devices can be used for initial tube confirmation
however, IT IS REQUIRED TO CONFIRM TUBE PLACEMENT WITH
CAPNOGRAPHY.
See Protocol: Capnography
O. Accurate documentation includes indications for intubation as well as measures
taken for tube verification.
P. If patient is in cardiac arrest for medical reasons then use of a ResQPod device
is required.
Complications
A. Esophageal intubation: particularly common when tube not visualized as it
passes through cords. The greatest danger is in not recognizing the error.
Auscultation over stomach during trial ventilations should reveal air gurgling
through gastric contents with esophageal placement. Also make sure patient's
color improves as it should when ventilating.
B. Intubation of right main stem bronchus: be sure to listen to chest bilaterally.
C. Upper airway trauma due to excess force with laryngoscope or to traumatic tube
placement
D. Vomiting and aspiration during traumatic intubation or intubation of patient with
intact gag reflex
E. Hypoxia due to prolonged intubation attempt
F. Cervical spine fracture in patients with arthritis and poor cervical mobility
G. Cervical cord damage in trauma victims with unrecognized spine injury
H. Ventricular arrhythmias or fibrillation in hypothermia patients from stimulation of
airway
I. Induction of pneumothorax, either from traumatic insertion, forceful bagging, or
aggravation of underlying pneumothorax
Return to Table of Contents
OROTRACHEAL TUBE SIZE
AGE
ENDOTRACHEAL TUBE
2.5 - 3.0 uncuffed
Preemie
3.0-3.5 uncuffed
Newborn
3.5 uncuffed
6 mos.
4.0 uncuffed
18 mos.
4.5 uncuffed
3 yrs.
5.0 uncuffed
5 yrs.
6.0 cuffed
8 yrs.
6.5-7.0 cuffed
15 yrs.
7.0-9.0 cuffed
Adult
Note: The pediatric Broselow™ tape is the most accurate predictor of tube
size.
Return to Table of Contents
1050
NASOTRACHEAL INTUBATION
P
Indications
A. Same function as orotracheal intubation in patients greater than 12 years of age
B. Used in the breathing patient requiring intubation
C. Asthma or pulmonary edema with respiratory failure, where intubation may need
to be achieved in a sitting position
Precautions
A. Head must be exactly in midline for successful intubation.
B. Have suction ready. Vomiting can occur, as with any stimulation of the airway.
C. Often nares are asymmetrical and one side is much easier to intubate. Avoid
inducing bilateral nasal hemorrhage by forcing a nasotracheal tube on multiple
attempts.
D. The use of nasotracheal intubation should be discouraged in patients with
significant nasal or craniofacial trauma.
E. Blind nasotracheal intubation is a very gentle technique. In the field, the secret of
blind intubation is perfect positioning and patience.
F. Only absolute contraindication is apnea
G. Should not be attempted in children under 12 years of age
Technique
A. Choose correct ET tube size (usually 7 mm tube in adult). Limitation is nasal
canal diameter.
B. Position patient with head in midline, neutral position (cervical collar may be in
place, or assistant may provide cervical stabilization in trauma patients).
C. Administer Phenylephrine nasal drops, 1 – 2 gtts, in both nostrils.
D. Assist ventilations prior to procedure if spontaneous respirations are inadequate.
E. Lubricate ET tube with Xylocaine jelly or other water-soluble lubricant.
F. With gentle steady pressure, advance the tube through the nose to the posterior
pharynx. Use right or largest nostril. Abandon procedure if significant resistance
is encountered.
G. Keeping the curve of the tube exactly in midline, continue advancing slowly.
H. There will be a slight resistance just before entering trachea. Wait for an
inspiratory effort before final advance into trachea. Patient may also cough or
buck just before breath.
I. Continue advancing until air is exchanging through the tube.
J. Advance about 1 inch further, then inflate cuff.
K. Ventilate and auscultate chest and abdomen for proper tube placement.
L. Note proper tube position and tape securely.
M. Apply Capnography for continuous end tidal CO2 monitoring
Complications
A. Same as orotracheal intubation. In addition:
1. Further craniofacial injury particularly in patients presenting with facial trauma
2. Nasal bleeding caused by tube trauma.
3. Vomiting and aspiration in the patient with intact gag reflex.
Go to Table of Contents
IN
1060
END-TIDAL CO2 MONITORING
P
Indications
A. All intubated patients require continuous end-tidal CO2 monitoring device and
although end-tidal colorimetric devices can be used for initial confirmation,
Capnography must still be used. Colorimetric devices are not standard of
care for prolonged monitoring of intubated patients.
B. Continuous end-tidal CO2 monitors are to be used to monitor patients requiring a
mechanical ventilator during transportation. The monitor is used to determine if
an endotracheal tube has become displaced or to detect the disruption of the
ventilator circuit.
See Protocol: Capnography
Precautions
A. Caution should be exercised to ensure that the clinical picture matches the
colorimetric end-tidal CO2 detector reading.
Technique - Colorimetric End-tidal CO2 Detectors
A. The colorimetric end-tidal CO2 detector should be placed in-line between the
endotracheal tube and the BVM immediately after the endotracheal tube is
passed.
B. Proper tube placement is confirmed by a color change in the colorimetric device,
indicating the elevated concentrations of CO2 expected in the trachea. Elevated
concentrations of CO2 are not expected in the esophagus.
Complications
A. Contamination with blood and secretions may render colorimetric end-tidal CO2
detectors ineffective.
B. Device may be ineffective or inaccurate in patients without spontaneous
circulation.
Note
A. Adhere to the expiration dates on these devices.
B. Follow manufacturers instructions for appropriate ranges and color indications.
Go to Table of Contents
1070
PERCUTANEOUS CRICOTHYROTOMY
P
Introduction
A. Percutaneous cricothyrotomy is a difficult and hazardous procedure that is to be
used only in extraordinary circumstances as defined below. The reason for
performing this procedure must be documented and submitted for review to the
physician advisor or designee within 24 hours. Percutaneous cricothyrotomy is
to be performed only by paramedics trained in the procedure.
Indications
A. When a life threatening condition exists and advanced airway management is
indicated, and you are unable to establish airway by other means.
Precautions
A. Bleeding is possible, even with correct technique. Straying from the midline is
very dangerous and likely to cause hemorrhage from the carotid or jugular
vessels, or their branches.
Technique
A. Using aseptic technique (Betadine/alcohol wipes) cleanse the area.
B. Position the patient in a supine position, with in-line spinal immobilization if
indicated.
C. At this time the scalpel included with the kit may be used to make a ¼ inch
vertical incision through the skin, over the cricothyroid membrane.
D. Using the prepackaged set, insert the needle or over-the-needle-catheter through
the cricothyroid membrane in a caudal direction at a 45-degree angle.
E. If using an over-the-needle-catheter, remove the syringe and needle. Otherwise
remove the syringe.
F. Insert the guidewire through the catheter or needle.
G. Remove the catheter or needle over the wire.
H. Slide the dilator and tracheostomy tube onto the wire into the neck incision.
I. Push the dilator through the cricothyroid membrane with a twisting motion, and
insert the tracheostomy tube into the trachea.
J. Remove the dilator and wire, leaving the tracheostomy tube in place.
K. Ventilate with BVM and 100% oxygen.
L. Confirm tube placement is successful. (Chest rise and fall, breath sounds,
secondary confirmation device). Observe for subcutaneous air, indicating
tracheal injury or improper placement.
M. Secure tube with ties.
N. Transport to appropriate facility.
Go to Table of Contents
1080
OTHER AIRWAY DEVICES
Introduction
Dual lumen airway device(s) are to be used as a rescue when
endotracheal intubation is not preferable, possible and/or BLS
methods have proven unsuccessful. These devices have external
insertion depth marks, an anatomically shaped proximal cuff to seal
the nasopharynx and oropharynx, and a distal cuff to seal the
esophagus and to help minimize the possibility of gastric insufflation.
The second channel, or gastric access lumen, allows the ability to
pass a French suction catheter (18 f for adults) into the stomach.
Depending on the device, the airways may be sized or limited to
patients between 4’8” and 6 ft in height.
Indications
1. Cardiac arrest
2. Difficult airway cases where endotracheal intubation is not possible
and BLS methods are unsatisfactory or unsuccessful.
Contraindications/Precautions
1. Responsive patients with an intact gag reflex
2. Known esophageal disease
3. Known ingestion of caustic substances
4. Respiratory burns
King LT-D
1. Choose correct size, based on patient height.
2. Test cuff and inflation system for leaks by injecting the maximum recommended
volume of air into the cuffs. Remove all air from both cuffs prior to insertion.
3. Apply lubricant to the beveled distal tip and posterior aspect of the tube, taking
care to avoid introduction of lubricant in or near the ventilatory openings.
4. Pre-oxygenate, if possible.
5. Position the head. The ideal head position is the "sniffing position". However, it
may also be inserted with the head in a neutral position.
6. With the dominant hand holding the King device at the connector. With nondominant hand, hold mouth open and apply chin lift.
7. With the device rotated laterally 45-90o such that the blue orientation line is
touching the corner of the mouth, introduce tip into mouth and advance behind
base of tongue.
8. As tube tip basses under tongue, rotate tube back to midline (blue orientation line
faces chin).
9. Without exerting excessive force, advance tube until base of connector is aligned
with teeth or gums.
10. Using syringe, inflate both cuffs, using the recommended amount of air for the
device (size 3 = 50 ml, size 4 = 70 ml, size 5 = 80 ml).
11. Attach EtCO2 monitor to ventilation port.
12. While gently ventilating with a BVM, withdraw until ventilation is optimized.
Go to Table of Contents
13. Attach ResQPod to ventilation port
14. Confirm proper position by auscultation, chest movement and verification of CO2
by EtCO2 monitor.
a. Depth markings are provided at the proximal end of the King LT-D.
These refer to the distance from the distal ventilatory opening. When
properly placed, with the distal tip and cuff in the upper esophagus, and
the ventilatory openings aligned with the opening to the larynx, the depth
markings give an indication of the distance, in centimeters, from the vocal
cords to the teeth.
15. Secure King device to patient using tape or other accepted means. A bite block
can also be used, if desired.
Complications and Special Notes
Because of the relative lack of complications and the ability to place
this airway without interruption of CPR, it should be considered a
primary airway device in cardiac arrest.
The King LT-D Airway is to be used in unconscious, apneic patients or
those unconscious patients who are spontaneously breathing but
without a gag reflex,
If the patient regains consciousness or develops a gag reflex, prepare
suction, immediately deflate all cuffs and remove the device.
Patients that do not fall within the height ranges of the device will
instead require intubation. DO NOT USE THIS DEVICE IF THE
PATIENT IS NOT OF ADEQUATE HEIGHT.
Return to Table of Contents
1081
ResQPod (Circulatory Enhancer)
The ResQPOD circulatory Enhancer provides a small but important
amount of resistance when breathing through the device. This
resistance increases blood flow back to the heart, so that on the next
chest compression, more blood is circulated out of the heart, through
the coronary arteries and the rest of the body. This device can be
used during assisted ventilation to improve circulation.
Indications
Assisted ventilations for patients with an advanced airway during
cardiac arrest (ET tube or King Airway)
Contraindications/Precautions
Conscious patients
Known dilated cardiomyopathy
Known pulmonary hypertension and/or aortic stenosis
Chest trauma
Technique
1. Once the patient is endotracheally intubated, attach the EtCO2 device to the ET
tube then attach the bottom of the ResQPOD directly to the top of the EtCO2
device.
2. Be sure all pieces fit as tightly together as possible, ensuring that the airway
adjunct has not become dislodged.
3. Attach the BVM to the top of the ResQPOD and begin ventilating, using the
EtCO2 values to direct your rate of ventilations.
Complications and Special Notes
The device has a timing assist light, that when switched to the "On"
position may serve as a guide to administering ventilations at a rate of
ten (10) per minute.
The ResQPOD is for single patient use only.
The ResQPOD may be used with other airway adjuncts, such as
rescue airways (King LT-D).
Return to Table of Contents
2000
CARDIAC ARREST
GENERAL PRINCIPLES
Specific Information Needed
A. History of arrest: onset, preceding symptoms, bystander CPR, other treatment,
duration of arrest
B. Past history: medical/surgical history, medications, allergies
C. Surroundings: environmental conditions, evidence of drug ingestion, trauma,
other unusual presentations
Document Specific Objective Findings
A.
B.
C.
D.
E.
Absence of consciousness
Agonal or no respirations
Absence of pulse
Signs of trauma, blood loss
Skin temperature
General Treatment Guidelines
A. Assure unobstructed airway
B. Request ALS assistance if not already on scene or responding.
C. Refer to appropriate protocol
1. Automated External Defibrillator (AED) – protocol 2010
2. Witnessed/Unwitnessed Adult Cardiac Arrest – protocol 2020
3. Trauma Arrest - protocol 5010
4. Pediatric Arrest - protocol 6020
Special Notes
A. Survival from cardiac arrest is related to the time to BOTH BLS and ALS
treatment. Don't forget CPR in the rush for advanced equipment. A call for backup should be initiated promptly by any BLS unit. Likewise, standing order
administration of the first steps in treatment is recommended to minimize time
delays to ALS.
B. Large peripheral veins (antecubital or external jugular) are preferred IV sites in
cardiac arrest. IO access should be considered if first attempt peripheral access
is unsuccessful. Additional lines can be started later in the arrest and IO access
is preferred to ET drug administration.
C. Quick-look paddles-or Combi-Pads are preferred for initial rhythm check. Be
sure machine is set to record from whichever mode is in use.
D. Be sure to recheck for pulselessness and unresponsiveness upon arrival, even if
CPR is in progress. This will avoid needless and dangerous treatment of
"collapsed" patients who are inaccurately diagnosed initially, or who have
spontaneous return of cardiac function after an arrhythmia or vasovagal episode.
E. After conversion to another rhythm, providers should switch to the appropriate
protocol for continued and ongoing treatment.
F. Good high quality CPR with minimal interruption is shown to improve survival
more than any procedure or drug administration. Be sure it is being done
correctly. Avoid hyperventilation.
G. If appropriate, OTHER AIRWAY DEVICES like the King airway should be
considered first line to avoid delay in securing the airway while minimizing
interruptions to compressions.
H. The ResQPod device should be used in arrest when appropriate.
Go to Table of Contents
2010
AUTOMATED EXTERNAL DEFIBRILLATOR
Indications
A. Patient must be unconscious, pulseless and apneic.
Precautions
A. A patient who is talking is not pulseless.
B. AEDs may be utilized for pediatric arrests if pediatric-sized defibrillator pads are
available and compatible with the machine.
C. Do not use on trauma patients.
D. Dry the chest well if wet.
E. Remove any transdermal patches to avoid igniting a Nitroglycerin patch.
F. If an airway obstruction exists, clear the airway before using AED.
G. Protect rescuers: “Clear” the patient, use only in safe and dry environment.
H. May not be able to use in a moving vehicle.
Technique
A. Follow manufacturer directions for AED operation. In absence of specific
operational instructions, the following technique is used.
1. Determine unresponsiveness.
2. Open airway, check for breathing, give a breath if no respirations.
3. Determine pulselessness.
4. Apply AED according to manufacturer’s guidelines.
5. Turn the AED on and follow its instructions.
6. Assure all rescue personnel are “Clear” and not touching the patient or
stretcher.
7. Whenever “no shock advised” or following a delivered shock, check patient’s
pulse. If no pulse, begin CPR and reanalyze every 2 minutes.
8. Use appropriate airway adjuncts to secure airway. If there is a pulse, check
breathing and assist as needed.
9. Once the AED is applied, necessary steps should begin immediately to
transport the patient to the hospital or rendezvous with an advanced life
support ambulance.
10. Shocks may be continued during transport, as long as indicated.
11. After 2 minutes of CPR, check pulse again. If no pulse, repeat steps to
analyze and defibrillate as long as shocks are indicated.
Special Notes
A. A rescuer may be shocked if one forgets to clear the area, or leans against metal
stretcher or patient during procedure.
B. Expired AED patches can cause arching of electricity or inadequate shock.
C. Do not delay this procedure by performing other procedures first, such as airway
adjuncts and IV access.
D. In presumed hypothermic patients, institute hypothermia protocol and contact
base.
Go to Table of Contents
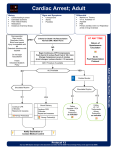
2020
VENTRICULAR FIBRILLATION/PULSELESS VENTRICULAR TACHYCARDIA
Unwitnessed
* Witnessed
Adult (>12) Cardiac Arrest
2 Minutes of Compressions (80100/min)
No interruptions
**IV, Epi, Airway
V-Fib or Pulseless V-Tach
Defibrillate 1x at
Max Joules
Asystole/PEA/NSA*
V-Fib or Pulseless V-Tach
ROSC
ACLS/BCLS Algorithm
Defibrillation x 1 Max joules
ACLS/BCLS Algorithm
Asystole/PEA/NSA*
V-Fib or Pulseless V-Tach
ROSC
ACLS/BCLS Algorithm
Compressions 2 minutes without
pauses
**IV, Epi, Airway
ACLS/BCLS Algorithm
Defibrillation x 1 Max joules
Asystole/PEA/NSA*
V-Fib or Pulseless V-Tach
ROSC
ACLS/BCLS Algorithm
Compressions 2 minutes without
pauses
**IV, Epi, Airway
ACLS/BCLS Algorithm
Defibrillation x 1 Max joules
Asystole/PEA/NSA*
V-Fib or Pulseless V-Tach
ROSC
ACLS/BCLS Algorithm
ACLS/BCLS V-Fib / Pulseless VTach Algorithm
ACLS/BCLS Algorithm
Must be medical, normothermic arrest
Must be from primary respiratory mechanism
NSA* - no shock advised on AED
* Witnessed by provider with defibrillator immediately available
** If possible without interrupting compressions
** Ventilation rate should be 8-10 per minute
Go to Table of Contents
2020
VENTRICULAR FIBRILLATION
PULSELESS VENTRICULAR TACHYCARDIA
(Continued from 2020 – Unwitnessed/Witnessed Adult Cardiac Arrest)
1.
2.
3.
4.
5.
Administer Amiodarone 300 mg IV bolus for refractory VF/VT.
Defibrillate at maximum joule setting. (Pridemark: 360 Joules)
Consider Magnesium Sulfate, 2 gm IV bolus
Defibrillate at maximum joule setting.
Consider transport options.
Special notes
A. Per AHA guidelines CPR should be performed immediately after each
defibrillation attempt for two minutes prior to performing rhythm checks.
B. Torsade de pointes is a rare and special form of ventricular-tachycardia.
Consider treating with Magnesium sulfate.
C. The initiation of IV or airway treatments should not delay defibrillation.
D. After conversion from VF/VT, consider Amiodarone 150 mg IV bolus infusion
over 10 minutes.
Return to Table of Contents
2030
ASYSTOLE
IN
A.
B.
C.
D.
E.
IN
CB
Begin Basic Life Support measures, including CPR
Establish airway.
Establish IV/IO access
Begin cardiac monitoring. Confirm asystole in at least two leads.
Consider transcutaneous pacing.
F. Administer epinephrine 1.0 mg, (1 ml of a 1:10,000 solution) IV bolus. If no
change, repeat every 3-5 minutes.
G. Administer atropine 1.0 mg, IV bolus. If no change, repeat every 3-5 minutes, not
to exceed 3.0 mg.
H. Administer sodium bicarbonate 1.0 mEq/kg, IV bolus. This should be considered
only in prolonged cardiac arrest situations.
I. Contact base for transport options.
Special notes
A. Patients who convert from a viable rhythm into asystole should have
transcutaneous pacing initiated immediately. However, pacing should be
withheld from those patients who present in asystole.
B. The effectiveness of transcutaneous pacing is directly related to the speed with
which this therapy is initiated.
C. When asystole is diagnosed, check the integrity of the leads and electrode
patches and confirm this interpretation in at least two leads.
D. In pediatric patients, after ABCs have been initiated, ventilate, consider an IV
fluid bolus of normal saline 20 ml/kg, reassess, consider epinephrine.
Go to Table of Contents
2040
PULSELESS ELECTRICAL ACTIVITY (PEA)
INITIATE SUPPORTIVE MEASURES:
IN
- ABCs
- CPR
- Endotracheal intubation
- Establish venous access
IN
CB
CONSIDER POSSIBLE CAUSES:
TREATMENT:
Hypovolemia
IV fluid bolus (20 ml/kg normal saline)
Tension pneumothorax
Chest decompression (per protocol)
Hypoxia
Ensure airway patency
Acidosis
Ventilation
Cardiac tamponade
IV fluid bolus (20 ml/kg normal saline)
Hypothermia
see 4063 Hypothermia protocol
Pulmonary embolism
Myocardial infarction
Drug overdose
Hyperkalemia
Sodium bicarbonate
EPINEPHRINE (1:10,000)
1.0 mg IV/IO push, repeat every 3 – 5
minutes
Pediatric doses: First dose: 0.01
mg/kg IV/IO/ET (0.1 ml/kg of 1:10,000
solution); Subsequent doses: 0.01
mg/kg, IV/IO/ET (0.1 ml/kg of
1:10,000 solution
ATROPINE for BRADYCARDIA
1.0 mg IV/IO push, repeat every 3-5
minutes, not to exceed 3.0 mg
Pediatric dose: refer to Length Based
Measurement tool
INITIATE TRANSPORT
Special notes
A. Standing orders should expedite care - not prolong scene time. Rapid transport
is still the goal.
B. In pediatric patients, ventilate, consider fluid bolus, reassess, consider
epinephrine.
Go to Table of Contents
IN
2050
ARRHYTHMIAS: GENERAL CONSIDERATIONS AND TREATMENT
Specific Information Needed
A. Present symptoms: sudden or gradual onset, palpitations
B. Associated symptoms: chest pain, dizziness or fainting, trouble breathing,
abdominal pain, fever
C. Prior history: arrhythmias, cardiac disease, exercise level, pacemaker
D. Current medications, particularly cardiac
Specific Objective Findings
A. Vital signs
B. Signs of poor cardiac output:
1. Altered level of consciousness
2. Outward appearance of shock: cool/clammy skin, pallor, diaphoresis
3. Systolic blood pressure < 90 mmHg
C. Signs of cardiac failure (increased back-up pressure):
1. Neck vein distention
2. Lung congestion, rales
3. Peripheral edema: sign of chronic failure, not acute
D. Signs of hypoxia: marked respiratory distress, cyanosis, tachycardia
Advanced treatment, general
A. Administer oxygen, position of comfort.
B. Establish venous access.
C. Evaluate the patient. Is the patient perfusing adequately or are there signs of
inadequate perfusion?
D. Apply cardiac monitor and evaluate arrhythmia.
1. Is there a pulse corresponding to monitor rhythm?
2. Rate: tachycardia, bradycardia, normal?
3. Are the ventricular complexes wide or narrow?
4. What is the relation between atrial activity (P waves) and ventricular
activity?
5. Is the arrhythmia potentially dangerous to the patient?
E. Document the arrhythmia by rhythm strip and 12 lead EKG if available.
F. Treat if needed according to pulse rate, perfusion status, risk of deterioration or
as directed by base physician.
G. Document results of treatment (or lack thereof) by checking pulse and recording
change on paper tape.
H. Transport patient. Monitor condition enroute.
Go to Table of Contents
Specific Precautions
A. Treat the patient, not the arrhythmia! If the patient is perfusing adequately, he
does not need emergency treatment. This is true of bradyarrhythmias as well as
tachyarrhythmias. What is normal for one person may be fatal to another.
B. Documentation of arrhythmias is extremely important. Field treatment of an
arrhythmia may be life saving, but long-term treatment requires knowing what the
problem was.
C. Correct arrhythmia diagnosis based only on monitor strip recordings is difficult
and often not possible. Treatment must be based on observable parameters:
rate, patient condition and distance from the hospital.
D. Dangerous rhythms are those which do not necessarily cause poor perfusion, but
are likely to deteriorate. They require recognition and treatment to prevent
degeneration to mechanically significant arrhythmias. Some of these dangerous
rhythms include ventricular tachycardia and Mobitz II 2nd degree block.
E. Cardiac arrest and life-threatening arrhythmias can be treated in the field, and
show the benefits of "stabilization before transfer" in prehospital care. The
patient is better off when the duration of arrest or poor perfusion is minimized.
F. Drug dosages vary in the pediatric and elderly populations.
Return to Table of Contents
IN
2060
PREMATURE VENTRICULAR CONTRACTIONS (PVCs)
A. The treatment of PVCs is rarely, if ever, indicated in the prehospital setting.
B. Patients with PVCs and active chest pain should have their pain treated
aggressively with oxygen, Aspirin, nitrates, and pain medications.
C. Prophylactic use of Amiodarone is contraindicated.
Go to Table of Contents
IN
2070
BRADYCARDIA WITH PULSE
Patients who are asymptomatic with normal blood pressure do not need treatment of
bradycardia in the field, they require transport.
Initiate Supportive Measures:
• Airway management
• Initiate oxygen therapy
• Establish venous access
Is the patient conscious, alert and
without signs of poor perfusion?
Yes
No
(Intermediates contact base)
Initiate transport
Atropine
0.5-1.0 mg IV
bolus
Evaluate response
Systolic BP >90
mmHg
Heart rate normal
Systolic BP <90 mmHg
Persistent
hemodynamically
unstable bradycardia
Initiate transport
Fluid bolus up to 250 cc
maximum
Atropine
0.5-1.0 mg IV push
Evaluate response
Initiate transport and contact
base to consider dopamine
or epinephrine administration
Consider
Transcutaneous pacing,
if available
Initiate transport and
contact base to consider
dopamine or epinephrine
administration
Special notes
A. Do not delay Transcutaneous Pacing while awaiting IV access or for Atropine to
take effect if the patient is showing signs of poor perfusion.
Go to Table of Contents
B. When pacing, verify mechanical capture and patient tolerance. Administer
Midazolam or Diazepam per protocol, if conscious, after initial pacing.
C. Differentiate premature ventricular beats from escape beats, which are wide
complexes occurring late after preceding beat as a lower pacemaker cell takes
over. Escape beats are beneficial to the patient and should be treated by
increasing the underlying rate and conduction; not by suppressing the escape
beats.
D. In pediatric patients, bradycardia is most often a sign of hypoxia. After therapy
for the ABCs has been initiated, hyperventilate, give fluid bolus, reassess, and
consider epinephrine. Epinephrine should be the first medication utilized.
Return to Table of Contents
IN
2080
NARROW COMPLEX TACHYCARDIA WITH PULSE
Initiate Supportive Measures:
•
Airway management
•
Initiate oxygen therapy
•
Establish venous access (If unable and patient is
hemodynamically unstable, move to synchronized cardioversion)
Is the patient conscious, alert and without signs of poor perfusion?
Yes
No
(Intermediates contact base)
Attempt Valsalva’s maneuver
Refer to Synchronized Cardioversion
Protocol (paramedic only)
Initiate Transport
Initiate Transport
Administer Adenosine 6 mg, rapid IV
bolus followed by 20 ml Normal Saline
Flush
Contact Base
If no change, administer Adenosine 12
mg, rapid IV bolus followed by 20 ml
Normal Saline Flush
Contact Base
Special notes
A. Valsalva’s Maneuver
1. This is any action that causes the patient to bear down against the closed
glottis.
2. Carotid sinus massage, orbital pressure or stimulation of mammalian diving
reflex is Not Permitted.
B. A narrow, QRS complex is less than 0.12 seconds in duration.
C. Tachycardia is most likely a secondary problem when the pulse is less than 150
in an adult. Treat hypoxia, hypovolemia, pain, and other problems first.
D. Adenosine is not effective in treating atrial fibrillation, which is an irregular
rhythm.
E. Adenosine must be administered over 1-3 seconds and followed by a rapid 20ml
saline flush. A proximal vein and port are preferred.
F. Pridemark specific: Consider Cardizem for A-Fib >150
Go to Table of Contents
G. If the patient takes theophylline or xanthine derivatives, higher doses of
adenosine may be needed.
Return to Table of Contents
2081
WIDE COMPLEX TACHYCARDIA WITH PULSE
IN
•
Initiate Supportive Measures:
• Airway management
• Initiate oxygen therapy
Establish venous access (If unable and patient
is hemodynamically unstable, move to
synchronized cardioversion)
Is the patient conscious, alert and without
signs of poor perfusion?
Yes
No
Initiate transport
Refer to synchronized cardioversion
protocol (paramedic only)
Contact Base for consideration of one of
the following medications:
• Adenosine
• Amiodarone
• Magnesium (paramedics only)
Initiate transport
Special notes
A. A wide QRS complex is defined as a complex with a width of 0.12 seconds or
greater.
B. A wide complex tachycardia is usually ventricular in origin but may, on occasion,
be a supraventricular rhythm with aberrant conduction.
C. Consider Midazolam or Diazepam for cardioversion in conscious patients.
D. Immediate cardioversion is rarely needed for heart rates < 150.
Go to Table of Contents
2090
CHEST PAIN
Specific Information Needed
A. Symptoms: Patient of either gender, more than 20 years old, with any of the
following chief complaints:
1. Suspected Acute Coronary Syndrome
a. Pressure, tightness, heaviness in chest
b. Chest pain radiating into neck, jaw, shoulders, back, one or both
arms
c. Indigestion or heartburn, nausea and/or vomiting
d. Persistent shortness of breath
e. Weakness/dizziness/lightheadedness/loss of consciousness
f. No pain or discomfort; however, patient may experience painless
syncope, change in mental status, or dyspnea.
g. Cocaine or other stimulant drug use
2. Respiratory
a. Acute onset of shortness of breath
b. Wheezing
Document Specific Objective Findings
A. Vital signs
B. General appearance: color, apprehension, sweating
C. Signs of heart failure: neck vein distention, peripheral edema, respiratory
distress
D. Lung exam by auscultation: rales, wheezes or decreased sounds
E. Chest wall tenderness, abdominal tenderness
Treatment
A. Reassure and place patient at rest, position of comfort.
B. Administer oxygen.
C. If patient’s history suggests a potential cardiac origin to the chest pain:
1. Administer 4 chewable aspirin tablets, 324mg total, if patient is able to
swallow
2. Establish venous access.
IV
3. Monitor cardiac rhythm and obtain 12 lead EKG if available. If patient has
1mm ST elevation in two or more contiguous leads, notify receiving hospital
for CARDIAC ALERT.
IN
D. Administer nitroglycerin, 0.4mg SL if BP > 100 systolic. Repeat every 5 min until
pain is relieved or systolic BP drops < 100.
IN
CB
E. If pain persists after third nitroglycerin, administer morphine sulfate or Fentanyl
for patients with no alteration of mental status and systolic BP > 100.
F. Consider base contact for additional nitroglycerin and/or morphine sulfate or
Fentanyl if pain persists.
Go to Table of Contents
Specific Precautions
A. “All chest pain should be considered cardiac in origin until proven otherwise” but
remember, there are many causes for chest pain. Consider pulmonary
embolism, pneumonia, aortic aneurysm, pneumothorax.
B. Consider Normal Saline fluid challenge or vasopressor if hypotensive. Beware of
IV fluid overload in the potential cardiac patient. Document breath sounds.
C. Patients taking medication for erectile dysfunction should not be given
nitroglycerin.
Return to Table of Contents
2095
CARDIAC ALERT
Cardiac Alert:
A. Cardiac alert is a program that is designed to mobilize cardiac catheterization
staff and have them awaiting the arrival of EMS. This reduces the door to
catheterization times and improves overall patient outcomes. By reducing time until
reperfusion, less damage occurs in the myocardium and reduces mortality
significantly.
B. Most hospitals in the metro and Boulder County area recognize cardiac alert with
the notable exceptions of Denver Health Medical Center and Boulder Foothills.
Criteria
1. Pt presenting with active chest pain or discomfort consistent with acute coronary
syndrome.
2. Pt is between the ages of 35 and 80
3. 1mm ST segment elevation in 2 or more anatomically contiguous leads See 12Lead ECG Patterns protocol
4. Consider MD consultation if transport time is greater than 10 minutes.
Exclusions
1.
2.
Procedure
1.
2.
3.
Paced Rhythm
Left Bundle Branch Block
Assess patient for all criteria listed above
Ensure that none of the exclusionary criteria exists
Contact dispatch IMMEDIATELY and inform them that you have a cardiac
alert and where your intended transport destination is.
4. Transport emergently and notify the receiving hospital while transporting
via normal means (Bio-phone) and inform them of patient condition and
that the patient is a cardiac alert.
5. Attempt to include all of the following in your report
i. Patient Age
ii. Patient Sex
iii. PMHx
iv. Elevated Leads
v. Cardiologist (if any)
vi. ETA
vii.
Special Considerations
1. If a patient does not meet all cardiac alert criteria it does not mean that
transport cannot be done emergently.
2. Cardiac Alert is a procedure and not a condition.
Go to Table of Contents
2100
HYPERTENSION
Specific Information Needed
A. History of hypertension and current medications
B. New symptoms: dizziness, nausea, confusion, visual impairment, paresthesia,
weakness
C. Drug use: phenylpropanolamine (found in a wide variety of over-the-counter
weight-loss products), amphetamines, cocaine or other stimulant drug use
D. Other symptoms: chest pain, breathing difficulty, abdominal/back pain, severe
headache
Specific Objective Findings
A. Evidence of encephalopathy: confusion, seizures, coma, vomiting
B. Presence of associated findings: pulmonary edema, neurologic signs, neck
stiffness, unequal peripheral pulses
Treatment
A.
B.
C.
D.
E.
IN
CB
Administer oxygen.
Place patient in position of comfort.
Monitor vital signs.
Treat chest pain, pulmonary edema or seizure activity per protocol.
Establish venous access.
F. If diastolic blood pressure remains above 130 mmHg on repeated readings and
patient has symptoms of encephalopathy without evidence of CVA or head injury,
CONTACT BASE to consider:
1. Nitroglycerin, 0.4 mg SL.
2. Morphine sulfate, 4.0 mg slow IV bolus, with repeat boluses of 2.0 mg slow IV
up to a maximum of 10 mg.
G. Monitor cardiac rhythm. Obtain 12 lead ECG, if available.
H. Monitor vital signs and mental status during transport.
Specific Precautions
A. Secondary hypertension (high BP in response to stress or pain) is commonly
seen in the field. It does not require field treatment, and may not even mean the
patient has chronic hypertension requiring ongoing treatment.
B. Hypertensive encephalopathy is rare, but can be treated with nitroglycerin or
morphine. Hypertension is more common in association with other problems
(pulmonary edema, seizures, chest pain, coma, or altered mental states). It
should be managed by treating the primary problem.
C. Diastolic pressures and mean arterial pressures are much more important in
determining danger of severe hypertension than is systolic pressure. These are
poorly measured in the field. The diagnosis of "malignant" hypertension is not
based on numerical levels, but rather on microscopic changes in blood vessels
and damage to organs, which place this disease beyond the scope of prehospital
care.
Return to Table of Contents
D. Hypertension is seen in severe head injury and intracranial bleeding, and is
thought to be a protective response that increases perfusion to the brain.
Treatment should be directed at the intracranial process, not the blood pressure.
Return to Table of Contents
3010
RESPIRATORY DISTRESS
Specific Information Needed
A. History: acute change or injury, slow deterioration
B. Past history: chronic lung or heart problems or known diagnosis, medications,
home oxygen, past allergic reactions, recent surgery, tobacco abuse
C. Associated symptoms: chest pain, cough, fever, hand or mouth paresthesia
Document Specific Objective Findings
A.
B.
C.
D.
E.
F.
G.
H.
I.
Vital signs
Oxygenation: level of consciousness, cyanosis
Respiratory effort: accessory muscle use, forward position, pursed lips
Neurologic signs: slurred speech, impaired consciousness, evidence of
drug/alcohol ingestion
Signs of upper airway obstruction: hoarseness, drooling, exaggerated chest wall
movements, inspiratory stridor
Signs of congestive failure: neck vein distention in upright position, rales,
peripheral edema
Breath sounds: clear, decreased, rales, wheezing, or rhonchi
Hives, upper airway edema
Evidence of trauma: crepitation of neck or chest, bruising, steering wheel
damage, penetrating wounds
Treatment
A. Put patient in position of comfort, usually upright.
B. Identify and treat upper airway obstruction if present (e.g. suctioning, NPA/OPA,
CPAP, endotracheal intubation, etc.).
C. Administer high flow oxygen.
D. Prepare to assist ventilations if patient fatigues or develops altered mentation, or
if respiratory arrest occurs.
E. If diagnosis unclear, place patient in position of comfort, and administer oxygen,
transport.
F. Assess and consider treatment for other problems if respiratory distress is severe
and patient does not respond to proper positioning and administration of oxygen.
G. Establish venous access.
H. Monitor cardiac rhythm.
Specific Precautions
A. Don't overdiagnose "psychogenic" in the field. Your patient could have a
pulmonary embolus or other serious problem; give him/her the benefit of the
doubt. Treatment with oxygen will not harm the “hyperventilator”, and it will keep
you from underestimating the problem.
B. Wheezing in older persons may be due to pulmonary edema ("cardiac asthma").
Pulmonary embolus is an uncommon cause of wheezing
Go to Table of Contents
3020
ASTHMA
Specific Objective Findings
A.
B.
C.
D.
Vital signs
Oxygenation: level of consciousness, cyanosis
Respiratory effort: accessory muscle use, forward position, pursed lips
Breath sounds: clear, decreased, wheezing, or rhonchi
Treatment
A.
B.
C.
D.
Put patient in position of comfort, usually upright.
Administer high flow oxygen.
Use appropriate airway adjuncts as indicated.
Assess and consider treatment for other problems if respiratory distress is severe
and patient does not respond to proper positioning and administration of oxygen.
E. If the patient is wheezing and has a metered dose inhaler (MDI), initiate MDI
protocol. EMT’s must contact base.
IV
F. Establish venous access.
IN
G. Monitor cardiac rhythm
IN
P
CB
H.
I.
J.
K.
Administer Albuterol Sulfate. Consider adding Ipratropium.
Use continuous nebulization of Albuterol Sulfate for respiratory distress.
Consider Epinephrine, 0.3 mg SQ/IM (0.3 ml of 1:1,000 solution).
Consider Methylprednisolone, 125 mg IV.
L. Consider Magnesium Sulfate, 2.0 gm, IV bolus, over 2 minutes
Specific Precautions
A. Prepare to assist ventilations if patient fatigues or develops altered mentation, or
if respiratory arrest occurs.
B. Wheezing in older persons may be due to pulmonary edema ("cardiac asthma").
Pulmonary embolus is an uncommon cause of wheezing.
C. If available, utilize pulse oximetry and capnography.
Go to Table of Contents
3030
CHRONIC OBSTRUCTIVE PULMONARY DISEASE
Specific Objective Findings
A.
B.
C.
D.
Vital signs
Oxygenation: level of consciousness, cyanosis
Respiratory effort: accessory muscle use, forward position, pursed lips
Breaths sounds: clear, decreased, rales, wheezing, or rhonchi
Treatment
A. Place patient in position of comfort, usually upright
B. Identify and treat upper airway obstruction of present (suctioning,
nasopharyngeal airway, endotracheal intubation, etc.).
C. Administer high flow oxygen.
D. Use appropriate airway adjuncts as indicated.
E. If the patient is wheezing and has a metered dose inhaler (MDI), initiate MDI
protocol. EMT’s must contact base.
F. Monitor cardiac rhythm. Perform 12-lead, if available.
G. Assess and consider treatment if respiratory distress is severe and patient does
not respond to proper positioning and administration of oxygen.
IN
IN
P
CB
H. Administer Albuterol Sulfate. Consider adding Ipratropium.
I. Use continuous nebulization of Albuterol Sulfate for respiratory distress.
J. Consider Methylprednisolone, 125mg IV bolus.
K. CONTACT BASE for Magnesium Sulfate, 2 gms IV over 2 minutes.
Specific Precautions
A. Wheezing in older persons may be due to pulmonary edema ("cardiac asthma").
Pulmonary embolus is an uncommon cause of wheezing.
B. Some COPD patients rely on a hypoxic drive for ventilatory support. Never
withhold oxygen for fear of decreasing this hypoxic drive.
C. If available, utilize pulse oximetry and capnography.
Go to Table of Contents
3040
PULMONARY EMBOLISM
Specific Information Needed
A. History: diabetes, chronic lung disease, congestive heart failure (CHF).
B. Past history: sedentary life style, surgery or recent fractures, pregnancy, oral
contraceptives, atrial fibrillation.
C. Associated symptoms: anxiety, dyspnea, chest pain, tachycardia, JVD
Document Specific Objective Findings
A.
B.
C.
D.
E.
Vital signs
Oxygenation: level of consciousness, anxiety
Respiratory effort: dyspnea, tachypnea, shortness of breath
Neurologic signs: impaired consciousness, syncope
Objective findings: distended neck veins, chest splinting, hypotension,
tachycardia.
F. Breath sounds: clear, decreased, rales, wheezing, or rhonchi
Treatment
A.
B.
C.
D.
E.
Put patient in position of comfort, usually upright.
Identify and treat upper airway obstruction if present
Administer high flow oxygen
Assist ventilation if necessary
If available, utilize pulse oximetry and capnography.
Special Precautions
A. Because prehospital care is primarily supportive and diagnosis difficult;
understanding the contributing factors is paramount.
B. A pulmonary embolism should be considered with any person who has an
unexplained cardiorespiratory problem.
Go to Table of Contents
3050
PULMONARY EDEMA
Specific Objective Findings
A.
B.
C.
D.
Vital signs
Oxygenation: level of consciousness, cyanosis
Respiratory effort: accessory muscle use, forward position, pursed lips
Signs of congestive failure: Neck vein distention in the upright position, rales,
peripheral edema.
E. Breath sounds: clear, decreased, rales, wheezing, or rhonchi.
Treatment
A. Place patient in position of comfort, usually upright.
1. Sit patient up, legs dangling if possible.
B. Administer high flow oxygen.
C. Consider CPAP
D. Assist ventilations with pocket mask or bag valve mask if necessary.
E. Establish venous access.
F. Monitor cardiac rhythm. Perform 12-lead, if available.
IN
P
CB
G. Consider:
1. Nitroglycerin 0.4mg SL
2. Morphine Sulfate, initial dose up to 4mg, then 2mg increments up to a total
dose of 10mg.
3. Lasix, 20-80mg slow IV push.
4. If available, consider CPAP.
Specific Precautions
A. If diagnosis is unclear, place patient in position of comfort, administer oxygen,
and transport.
B. Wheezing in older persons may be due to pulmonary edema (“cardiac asthma”).
Pulmonary embolus is an uncommon cause of wheezing.
C. Prepare to assist ventilations if patient fatigues or develops altered mentation, or
if respiratory arrest occurs.
D. If available, utilize pulse oximetry and capnography.
Go to Table of Contents
3060
HYPERVENTILATION
Specific Information Needed
A. History: anxiety provoking episode, acute change or injury
B. Past history: panic attack, anxiety attack, chronic lung or heart problems or
known diagnosis, medications, home oxygen, past allergic reactions, recent
surgery, tobacco use,
C. Associated symptoms: chest pain, cough, fever, hand or mouth paresthesia,
carpal pedal spasm, cerebrovascular constriction resulting in headache,
dizziness or euphoria.
Document Specific Objective Findings
A.
B.
C.
D.
E.
F.
G.
H.
I.
Vital signs
Oxygenation: level of consciousness, cyanosis
Respiratory effort: accessory muscle use, forward position, pursed lips.
Neurologic signs: slurred speech, impaired consciousness, evidence of
drug/alcohol ingestion.
Signs of upper airway obstruction: hoarseness, drooling, exaggerated chest wall
movements, inspiratory stridor.
Signs of congestive failure: neck vein distention in upright position, rales,
peripheral edema.
Breath sounds: clear, decreased, rales, wheezing, or rhonchi.
Hives, upper airway edema
Evidence of trauma: crepitation of neck or chest, bruising, steering wheel
damage, penetrating wounds.
Treatment
A.
B.
C.
D.
E.
Put patient in position of comfort, usually upright.
Identify and treat upper airway obstruction if present.
Administer high flow oxygen.
Use appropriate airway adjuncts as indicated.
Assess and consider treatment for the following problems
1. Coaching of breathing pattern and ventilations.
2. Calming of anxiety and stress inducing factors.
3. Suspicion that the symptoms are indicative of other illness, disorder or
overdose, patient should be transported.
Specific Precautions
A. Don’t over-diagnose “psychogenic” in the field. Your patient could have a
pulmonary embolus or other serious problem; give him/her the benefit of the
doubt. Treatment with oxygen will not harm the “hyperventilator”, and it will keep
you from underestimating the problem.
B. Utilize pulse oximetry and Capnography, if available.
Go to Table of Contents
3070
SPONTANEOUS PNEUMOTHORAX
Specific Information Needed
A. History: acute change or injury, slow deterioration
B. Past history: chronic lung or heart problems, medications, home oxygen, past
allergic reactions, recent surgery, tobacco use
C. Associated symptoms: chest pain
Document Specific Objective Findings
A. Vitals signs
B. Oxygenation: level of consciousness, cyanosis
C. Respiratory effort: accessory muscle use, shortness of breath, tachypnea,
decreased breath sounds on affected side
D. Neurologic signs: impaired consciousness, evidence of drug/alcohol ingestion
E. Signs of upper airway obstruction: exaggerated chest wall movements
F. Breath sounds: clear, decreased, rales, wheezing, or rhonchi
G. Assess for evidence of trauma: crepitation of neck or chest, bruising, steering
wheel damage, penetrating wounds
H. Other signs and symptoms: sudden onset of chest pain, diaphoresis, pallor,
subcutaneous emphysema.
Treatment
A.
B.
C.
D.
E.
Put patient in position of comfort, usually upright.
Identify and treat upper airway obstruction if present
Administer high flow oxygen.
Use appropriate airway adjuncts as indicated.
Assess and consider treatment for severe cases: airway, ventilatory and
circulatory support.
F. If a tension pneumothorax develops, follow “Tension Pneumothorax” protocol.
Special Precautions
A. May occur in apparently healthy persons; often men between 20 and 40 years of
age, which are tall and thin.
B. May occur in patients with COPD, patients with AIDS and pneumonia, history of
Marfan’s Syndrome, drug abusers.
C. Utilize pulse oximetry and capnography if available.
Go to Table of Contents
3080
PNEUMONIA
Specific Information Needed
A. History: acute change or injury, slow deterioration, general malaise.
B. Past history: chronic lung or heart problems or known diagnosis, medications,
home oxygen, past allergic reactions, recent surgery, tobacco abuse
C. Associated symptoms: chest pain, productive cough, fever, sputum production.
Treatment
A. Place patient in position of comfort, usually upright.
B. Identify and treat upper airway obstruction if present (suctioning, nasopharyngeal
airway, endotracheal intubation, etc.).
C. Administer high flow oxygen.
D. Assist ventilation if necessary.
E. Assess and consider treatment if respiratory distress is severe and patient does
not respond to proper positioning and administration of oxygen.
IN
CB
1. Administer Albuterol Sulfate 2.5 mg nebulization.
Special Precautions
A. Pneumonia can be caused by bacterial, viral, or fungal infection; these diseases
may spread by droplets or contact with infected persons. Utilize appropriate
Body Substance Isolation (BSI) precautions.
B. If diagnosis is unclear, place patient in position of comfort, administer oxygen,
and transport.
C. Prepare to assist ventilations if patient fatigues or develops altered mentation, or
if respiratory arrest occurs.
D. If available, consider pulse oximetry and capnography.
Go to Table of Contents
4000
MEDICAL EMERGENCIES
The following are protocols for various medical emergencies. Treatment for each may
be unique but there are similar things to consider when treating all medical patients.
A. Ensure the scene is safe and wear the appropriate protective equipment for
proper body substance isolation.
B. Obtain clues from the scene to help create a picture of the nature of the illness.
C. Determine if your patient is physiologically stable or unstable. Certain
assessment findings may help determine this, including:
1. Any airway obstruction that is limiting ventilation.
2. The patient is unable to maintain or protect their airway.
3. Not breathing or breathing inadequately.
4. Absent or diminished breath sounds.
5. Working hard to breathe and use of accessory chest muscles with retractions.
6. Absent or weak peripheral or central pulses.
7. H th8/chehat too fequason t, too sfol, oider1( thing out taregns of )( as. )]Tc -0.0009 Tc 0 TJ1.639
1. Repeat all previous assessments for any change.
2. Reassess vital signs.
3. Evaluate the effectiveness of any interventions.
J. It is always appropriate to err on the side of caution. If you feel the patient is
unstable, aggressively treat and transport rapidly to the appropriate facility.
Return to Table of Contents
4010
NEUROLOGICAL EMERGENCIES
Go to Table of Contents
4011
STROKE/CVA
Indication
A. For patients presenting with an acute episode of neurological deficits without any
evidence of trauma as the causative agent.
Specific Information Needed
A. Symptoms:
1. Altered level of consciousness
2. Impaired speech
3. Unilateral weakness / hemiparesis
4. Facial asymmetry / facial droop
5. Headache
6. Poor coordination or balance
7. Vision changes
8. Seizure activity
9. Previous CVA / TIA
10. Chest Pain
11. Last time “without symptoms”
Document Specific Objective Findings
A. Vital signs and complete history including patient medications
B. General appearance: color, apprehension, sweating
C. Cincinnati Prehospital Stroke Scale (CPSS)
1. Face – facial droop present
2. Arm – upper extremity arm drift present (arms extended, palms up)
3. Speech – inability to speak a simple sentence
4. Time – time of onset of symptoms / last time without symptoms
D. Complete Neurologic Exam
IV
E. Determine Blood Glucose level
IN
F. Monitor cardiac rhythm. Perform 12-lead EKG, if available.
Treatment
A.
B.
C.
D.
E.
Reassure and place patient with head slightly elevated (<30 degrees)
Administer oxygen.
NPO
Transport to appropriate facility
Contact receiving facility early with symptoms and objective findings
F. Establish venous access (proximal18 gauge or larger is preferred)
G. Administer dextrose 25 gm (50 ml of a 50% solution), IV bolus if blood glucose
reading <60 and if clinically indicated.
Special Precautions
A. Treatment of hypertension in the setting of CVA / TIA is not indicated in the
prehospital setting.
Go to Table of Contents
4012
COMA/ALTERED MENTAL STATUS/NEUROLOGIC DEFICIT
Specific Information Needed
A. Present history: duration of illness, onset and progression of present state
illness; preceding symptoms such as headaches, seizures, confusion, or trauma.
B. Past history: previous medical or psychiatric problems
C. Medications: use, misuse, or abuse
D. Surroundings: check for pill bottles or syringes and bring with patient. Note odor
in house.
Specific Objective Findings
A.
B.
C.
D.
E.
F.
G.
Safety of rescuer. Check for gases or other toxins.
Vital signs
Level of consciousness and neurological status
Signs of trauma
Breath odor
Needle tracks
Medical alert tag
Treatment
A. Use appropriate airway adjuncts as indicated
B. Administer oxygen.
C. If patient a known diabetic and can swallow administer one full tube of oral
glucose per protocol.
D. Establish venous access and fluid bolus as indicated.
E. Draw appropriate blood tubes. Test blood glucose level
F. Administer Dextrose 25 gm (50 ml of a 50% solution), IV bolus if blood glucose
reading <60 and/or if clinically indicated.
IV
IN
CB
G. Administer Naloxone up to 2 mg IV, IN, IM or IO if clinically indicated.
H. If venous access is unsuccessful and unable to administer dextrose, administer
Glucagon 1 mg IM.
I. Monitor cardiac rhythm.
J. Transport in lateral recumbent position. (If trauma suspected, transport supine
with cervical collar and backboard; logroll as necessary.)
K. Monitor vitals during transport.
Specific Precautions
A. Be particularly attentive to airway. Difficulty with secretions, vomiting, and
inadequate tidal volume are common.
B. Hypoglycemia may present as a focal neurological deficit or coma (stroke like
picture).
C. Coma in the diabetic may be due to hypoglycemia or to hyperglycemia (diabetic
ketoacidosis). Dextrose should be given IV Bolus to all unconscious diabetics,
as well as patients with coma of unknown origin unless a blood glucose reading
in the high range is obtained. The treatment may be life saving in hypoglycemic
Go to Table of Contents
patient, and will do no harm in the normal or hyperglycemic patient. Do not give
oral sugar to an unconscious patient.
D. Stroke patients may be alert but unable to respond (aphasic); therefore,
communicate with the patient and explain what you are doing. Avoid
inappropriate comments.
E. Naloxone is useful in any potential narcotic overdose, but be sure the airway and
the patient are controlled before giving naloxone to a known drug addict. The
acute withdrawal precipitated in an addict may result in violent combativeness.
Return to Table of Contents
4013
SEIZURES
Specific Information Needed
A. Seizure history: onset, time interval, previous seizures, type of seizure
B. Medical history: especially head trauma, diabetes, headaches, drugs, alcohol,
medications, compliance with anticonvulsants, pregnancy
Document Specific Objective Findings
A.
B.
C.
D.
E.
F.
G.
Vital signs
Description of seizure activity
Level of consciousness
Head and mouth trauma
Incontinence
Air temperature; patient temperature
Skin color and moisture
Treatment
A. Ensure airway patency. Nasopharyngeal airways are useful.
NOTE: Don’t force anything between the teeth.
B. Administer oxygen.
C. Suction as needed.
D. Protect patient from injury.
E. Check pulse immediately after seizure stops.
F. Keep patient on side.
G. Establish venous access.
H. Draw appropriate blood tube; test for blood glucose if available.
I. Administer Dextrose 25 gm (50 ml of a 50% solution), IV bolus if blood glucose
<60 and if clinically indicated.
J. Administer Naloxone up to 2 mg IV or IN (may also be given IM or IO by EMTIntermediate or paramedic) if clinically indicated.
1. If EMT-IV, contact base for consideration of administration of Naloxone as
described above
IV
IN
CB
L. If venous access unsuccessful after two attempts, administer Midazolam 1-5 mg
IM or IN.
P
IN
K. Administer Diazepam 1-10 mg slow IV push for status epilepticus.
CB
M. If venous access is unsuccessful and unable to administer dextrose, administer
Glucagon 1 mg, IM.
N. Monitor cardiac rhythm.
O. Keep in lateral recumbent position for transport.
P. Monitor vitals.
Specific Precautions
Go to Table of Contents
A. Move hazardous materials away from patient. Restrain the patient only if needed
to prevent injury. Protect patient's head.
B. Trauma to tongue is unlikely to cause serious problems, however, trauma to
teeth may. Attempts to force an airway into the patient's mouth can completely
obstruct airway. Do not use bite sticks or jaw screws.
C. Seizure can be due to lack of glucose or oxygen to the brain, as well as to the
irritable focus we associate with epilepsy. Hypoxia from transient arrhythmia or
cardiac arrest (particularly in younger patients) may cause seizure and should be
treated promptly. Don't forget to always check for pulse once a seizure
terminates.
D. Hypoxic seizures can also result when the tongue obstructs the airway in the
supine position, or when overly helpful bystanders prop the patient up or
improperly elevate the head.
E. Alcohol related seizures are common, but cannot be differentiated from other
causes of seizure in the field. Assessment in the intoxicated patient should still
include consideration of hypoglycemia and all other potential causes. Field
management is as for any seizure.
F. Seizures may be due to arrhythmias or stroke. It is important to look for and
recognize arrhythmias in the field since they may be the cause of the seizure.
G. Medical personnel are often called to assist epileptics who seize in public. If
patient clears completely, is taking his/her medications, has his/her own
physician, and is experiencing his/her usual frequency of seizures, transport may
be unnecessary. Consult your base physician.
H. Diazepam has a tendency to decrease respiratory effort, therefore be prepared to
assist ventilations.
I. Seizures in pregnant patients (or even those who are postpartum) may be the
presenting sign of eclampsia or toxemia of pregnancy.
P
1. Seizures in those patients will respond better to administration of magnesium
sulfate.
Return to Table of Contents
4014
SYNCOPE
Specific Information Needed
A. History of the event: onset, duration, seizure activity, precipitating factors. Was
the patient sitting, standing, or lying? Pregnant?
B. Past history: medications, diseases, prior syncope
C. Associated symptoms: dizziness, nausea, chest or abdominal/back pain,
headache, palpitations
Specific Objective Findings
A.
B.
C.
D.
Vital signs
Neurological status: level of consciousness, residual neurological deficit
Signs of trauma to the head or mouth or incontinence
Neck stiffness
Treatment
A. Place patient in position of comfort: do not sit patient up prematurely; supine or
lateral positioning if not completely alert
B. Monitor vital signs and level of consciousness closely for changes or recurrence.
IV
IN
C. Establish venous access and administer Normal Saline if indicated.
D. Consider hypoglycemia. If signs of hypoglycemia are present (clinical indications
and blood glucose<60):
1. Establish venous access.
2. Draw appropriate blood tubes.
3. Administer dextrose 25 gm (50 ml of a 50% solution), IV bolus.
4. If venous access is unsuccessful and unable to administer dextrose,
administer glucagon 1 mg IM.
E. If vital signs unstable or age > 40 years:
1. Administer oxygen.
2. Keep patient supine, elevate legs 10-12 inches.
IV
3. Establish venous access.
IN
4. Monitor cardiac rhythm. Consider 12-lead EKG if available.
Specific Precautions
A. Syncope is by definition a transient state of unconsciousness from which the
patient has recovered. If the patient is still unconscious, treat as coma. If the
patient is confused, treat according to Coma/Altered Mental Status/Neurologic
Deficit protocol.
B. Most syncope is vasovagal, with dizziness progressing to syncope over several
minutes. Recumbent position should be sufficient to restore vital signs and level
of consciousness to normal.
C. Syncope that occurs without warning or while in a recumbent position is
potentially serious and often caused by an arrhythmia.
Go to Table of Contents
D. Patients with syncope, even though apparently normal, should be transported. In
middle-aged or elderly patients, syncope can be due to a number of potentially
serious problems. The most important of these to monitor and recognize are
arrhythmias, occult GI bleeding, seizure, or ruptured abdominal aortic aneurysm.
E. Any elderly patient with syncope and back pain should be considered to
have a ruptured abdominal aortic aneurysm until proven otherwise.
F. In children 1-4 years of age breath-holding spells associated with heightened
emotional states can cause syncopal-like events. Children may be pallid or
cyanotic and seizures can occur. No specific treatment is indicated for these
events. Consult base station if questions.
Return to Table of Contents
4020
ALLERGY/ANAPHYLAXIS
Specific Information Needed
A. History: current sequence of events, exposure to allergens (bee stings, drugs,
nuts, seafood most common), prior allergic reactions.
B. Current symptoms: itching, wheezing, respiratory distress, nausea, weakness,
rash, anxiety, swelling.
C. Medications, past medical history.
Specific Objective Findings
A.
B.
C.
D.
Vital signs, level of consciousness
Respirations: wheezing, upper airway noise, effort
Mouth: tongue and airway swelling
Skin: hives, swelling, flushing
Treatment
A. Ensure airway patency. Early endotracheal intubation may be advisable before
swelling becomes severe. Suction as needed. Prepare to assist ventilations.
B. Position of comfort (upright if respiratory distress predominates; supine if shock
prominent)
C. Administer oxygen as indicated.
D. Remove the mechanism of injection if still present (stinger, needle, etc). Do not
squeeze venom sac; rather, scrape with straight edge.
E. Remove any clothing or other items which may contain the allergen, for example
if a person was horse back riding, clothing may still contain the allergen.
IV
F. If signs of severe generalized reaction present establish venous access.
G. Consider Epi-Pen if available (EMT-B must contact base).
IN
H. Monitor cardiac rhythm.
IN
CB
I.
Administer diphenhydramine 50 mg IV or IM (IO if already established) as
indicated.
J. For objective findings of respiratory distress such as stridor, wheezing, hypoxia,
tachypnea or angioedema, Epinephrine 0.3 mg of 1:1000 SQ/IM is indicated.
K. For signs of shock (BP < 90) or altered mental status:
1. Fluid bolus of Normal Saline at 20 ml/kg
2. Administer epinephrine, 0.1 mg 1:10,000 IV followed by epinephrine 1.0 mg
mixed in 250 ml Normal Saline infusion started at: 2mcg/min. Titrate to
desired effects including signs of improved perfusion or a systolic blood
pressure greater than 90 mmHg.
Specific Precautions
A. Allergic reactions can take multiple forms. Early consult with base physician is
encouraged.
B. Anxiety, tremor, palpitations, tachycardia, and headache are not uncommon with
administration of epinephrine. These may be particularly severe with IV
administration. In children, epinephrine may induce vomiting.
Go to Table of Contents
C. Angina, MI, or dysrhythmias may be precipitated.
D. Use caution in the administration of epinephrine in cardiac patients or the elderly.
E. Two forms of epinephrine are carried as part of paramedic equipment. The
standard ampules of aqueous epinephrine contain a 1:1000 dilution appropriate
for SQ or IM injection. IV epinephrine should be given in a 1:10,000 dilution. Use
the 1:10,000 premix for IV dosing to avoid mistakes. Be sure you are giving
the proper dilution to your patient, and give slowly.
F. Before treating anaphylaxis, be sure your patient has objective signs as well as
subjective symptoms and history. Hyperventilators will occasionally think they are
having an allergic reaction. Epinephrine will just aggravate their anxiety.
G. Lethal edema may be localized to the tongue, uvula, or other parts of the upper
airway. Examine closely, and be prepared for early intubation before swelling
precludes this intervention.
Return to Table of Contents
4030
ABDOMINAL PAIN
Specific Information Needed
A. Pain: nature (crampy or constant), duration, location; radiation to back, groin,
chest, shoulder
B. Associated symptoms: nausea, vomiting (bloody or coffee ground), diarrhea,
constipation, black or tarry stools, urinary difficulties, menstrual history, fever
C. Past history: previous trauma, abnormal ingestions, medications, known
diseases, surgery
Document Specific Objective Findings
A.
B.
C.
D.
E.
Vital signs
General appearance: restless, quiet, sweaty, pale
Abdomen: tenderness, guarding, distention, rigidity, pulsatile mass
Emesis, stool, or urine, describe, amount
Check for equality of pulses.
Treatment
A. Place patient in position of comfort
B. Give nothing by mouth
C. If BP <90 mmHg systolic and signs of hypovolemic shock:
1. Administer oxygen.
2. Establish venous access with 2 large bore lines. Consider Normal Saline
bolus of 20 ml/kg.
3. Consider transport to a trauma center based upon destination protocol.
D. Establish venous access even if vital signs normal.
IV
E. Cardiac monitor and 12 lead EKG (if available) for upper abdomen pain.
IN
IN
CB
F. Consider pain medication for hemodynamically stable patients with transport
times >10 minutes
Fentanyl 1-2 mcg/kg IV bolus to a cumulative dose of less than 200 mcg.
G. Monitor vitals during transport.
H. For patients who are nauseated or vomiting consider antiemetic administration.
Specific Precautions
A. The most important diagnoses to consider are those associated with catastrophic
internal bleeding: ruptured aneurysm, liver, spleen, ectopic pregnancy, etc.
Since the bleeding is not apparent, you must think of the volume depletion and
monitor patient closely to recognize shock. If a patient presents in shock,
consider transport to a trauma center where appropriate surgical consultation is
readily available.
B. Elderly patients may have significant hypovolemic shock with systolic blood
pressures above 90 mmHg. With signs of hypovolemia, treat with fluids.
C. Upper abdomen and lower chest pain may reflect thoracic pathology such as
myocardial infarction, etc. Massive fluid resuscitation may be contraindicated.
Go to Table of Contents
4031
VOMITING
Document Specific Objective Findings
A.
B.
C.
D.
E.
F.
G.
H.
I.
Frequency, duration of vomiting
Presence of blood or bile in vomitus
Associated symptoms: abdominal pain, weakness, confusion
Medication ingestion
Past medical history: diabetes, cardiac disease, abdominal problems, alcoholism
Vital signs
Color of vomitus: presence of blood
Abdomen: tenderness, guarding, rigidity, distention
Signs of dehydration: poor skin turgor, dry mucous membranes, confusion
Treatment
A. Position patient: left lateral recumbent if vomiting; otherwise, supine.
B. Administer oxygen.
C. Nothing by mouth
IV
P
D. If BP < 90 mmHg systolic and signs of hypovolemic shock or for signs of poor
perfusion in pediatric patients:
1. Elevate legs 10-12 inches.
2. Establish venous access.
3. Normal Saline bolus of 20 ml/kg
E. For patients who are nauseated or vomiting consider antiemetic administration.
a. Ondansetron (Zofran) 4mg IV/IM
b. Promethazine (Phenergan) 12.5mg IV
Specific Precautions
A. Vomiting may be a symptom of a more serious problem. The most serious
causes are GI bleed or other intra-abdominal catastrophe. A rare cardiac patient
may also present with vomiting as the predominant symptom.
B. Consider drug overdose; a patient who does not call the ambulance for
medication ingestion may call later when GI symptoms become severe.
C. The vast majority of persons with vomiting have become sick over days, not
minutes. Treat appropriately.
D. Dehydration may be particularly severe in children with simple vomiting. IVs may
be very difficult to start, particularly with infants.
Go to Table of Contents
4040
POISONS AND OVERDOSES
Specific Information Needed
A. Type of ingestion: What, when, and how much was ingested? Bring the poison,
the container, description of emesis, all medications and everything questionable
in the area with the patient to the Emergency Department.
B. Reason for exposure: think of child neglect, depression, etc.
C. Symptoms: respiratory distress, sleepiness, nausea, agitation or decreased level
of consciousness
D. Past history: medications, diseases, psychiatric
E. Action taken by bystanders: induced emesis? "antidote" given?
Document Specific Objective Findings
A.
B.
C.
D.
E.
F.
Vital signs
Airway: patency and adequacy of ventilation
Level of consciousness and neurologic status: check frequently.
Breath odor, increased salivation, oral burns
Skin: sweating, cyanosis
Systemic signs: vomitus, arrhythmias, lung sounds
Treatment
A. Use appropriate airway adjuncts as indicated.
B. Administer oxygen.
C. Support patient on side and protect airway.
IV
IN
CB
D. Establish venous access.
E. Test for blood glucose level, if available.
F. Administer dextrose 25 gm (50 ml of a 50% solution), IV bolus if blood glucose
<60 and if clinically indicated.
G. Administer naloxone up to 2 mg IV or IN (may also be administered IM or IO) in
patients with decreased respiratory effort and observe patient for improved
ventilations.
H. If venous access is unsuccessful and unable to administer dextrose, administer
glucagon 1 mg, IM.
I. Monitor cardiac rhythm.
J. Administration of sodium bicarbonate may be necessary with signs of a widened
QRS or ventricular arrhythmias after excessive tricyclic antidepressant(s)
ingestion. Administration of diazepam 1-10 mg slow IV bolus may be necessary
in suspected stimulant use or abuse (cocaine, Ecstasy, etc.)
Specific Precautions
A. There are few specific "antidotes." Product labels and home kits can be
misleading and dangerous. Watch the ABCs: these are important.
B. Do not neutralize acids with alkalis. Do not neutralize alkalis with acids. These
"treatments" cause heat releasing chemical reactions that can further injure the
GI tract.
C. Inhalation poisoning is particularly dangerous to rescuers. Recognize an
environment with ongoing contamination and extricate rapidly.
Go to Table of Contents
D. Organophosphate exposure may require massive doses of atropine.
E. For personal exposure to nerve agents refer to Mark I auto-injector protocol.
Rocky Mountain Poison Center #: 303-739-1123 (local) or 1-800-332-3073 (statewide)
Nationwide Poison Control Access#: 1-800-222-1222
Poison Control Phone for Hearing Impaired: 303-739-1127
CHEMTREC: 1-800-424-9300
Return to Table of Contents
4050
ENVIRONMENTAL EMERGENCIES
Go to Table of Contents
4051
HIGH ALTITUDE ILLNESS
Specific Information Needed
A. Presenting symptoms generally fall into two categories:
1. Acute mountain sickness (AMS) - headache, sleeplessness, anorexia,
nausea, fatigue.
2. High-altitude pulmonary edema (HAPE) - breathlessness, cough, headache,
trouble breathing, confusion, fatigue, nausea
3. High-altitude Cerebral Edema (HACE) – ataxia, headache, confusion, stroke
like picture with focal deficits, seizure and coma
B. Current and highest altitude, time at this altitude, duration of ascent
C. Medical problems, medications, previous experience at altitude
Document Specific Objective Findings
A. Vital signs
B. Mental status: confusion, lack of coordination, coma
C. Lungs: respiratory rate, distress, rales, sputum (bloody or frothy)
Treatment
A. Put patient at rest in position of comfort.
B. Administer oxygen.
C. Suction as needed. Assist ventilation if patient has cyanosis, confusion, and
poor respiratory effort.
D. For Pulmonary Edema consider Continuous Positive Airway Pressure (CPAP)
and if the patient fails to respond consider intubation.
IV
E. Establish venous access if conditions permit
Specific Precautions
A. Recognition of the problem is the most critical part of treating high altitude illness.
While in the mountains, recognize symptoms which are out of proportion to those
being experienced by the rest of the party: fatigue, or trouble breathing
(particularly at rest).
B. The mainstay of treatment is descent from altitude. Even a loss of 1,000 - 1,500
feet makes enough difference in the oxygen content of air that symptoms may be
relieved or stop progressing. Oxygen administration can also relieve symptoms
and may allow more time for orderly evacuation.
C. In addition to the more common pulmonary edema, cerebral edema may occur,
with confusion and a stroke-like picture with focal deficits. Treatment is the
same.
D. Acute mountain sickness, the mild form of illness during altitude adaptation,
consists of fatigue, headache, and poor sleeping, without severe CNS or
respiratory symptoms. Treatment is rest. This increases the body's time to
acclimatize. Descend if symptoms progress, or ataxia present.
E. Commercial airlines pressurize cabins to a level equivalent to about 5,000 8,000 feet.
F. Patients at risk for high altitude illness for whatever reason may be taking
Diamox (acetazolamide). Diamox may be useful in preventing some altitude
Go to Table of Contents
illness because of direct effects on acid-base balance. Diuretics are not useful,
however, in treating high altitude pulmonary edema, because the cause is
excess capillary leakage of fluid, rather than increased venous pressure.
Return to Table of Contents
4052
DROWNING/NEAR-DROWNING
Specific Information Needed
A. How long patient was submerged?
B. Degree of contamination, water temperature?
C. Diving accident? Water depth?
Specific Objective Findings
A. Vital signs
B. Neurologic status: monitor on a continuing basis.
C. Lung exam: rales or signs of pulmonary edema, respiratory distress
Treatment
A. Clear upper airway of vomitus or large debris.
B. Start CPR if needed.
C. Stabilize neck prior to removing patient from water if any suggestion of neck
injury.
D. Suction as needed.
E. Administer oxygen.
F. If patient not awake and alert:
1. Assist ventilation if necessary.
IV
2. Establish venous access
3. Consider use of Continuous Positive Airway Pressure (CPAP)
IN
4. Intubate when indicated and apply positive pressure ventilation.
5. Monitor cardiac rhythm during transport; treat arrhythmias per protocol.
G. Transport patient, even if normal by initial assessment.
Specific Precautions
A. Be prepared for vomiting. Patients should be secured on spineboard when
indicated for log-rolling to protect the neck and manage the airway.
B. All near-drownings should be transported. Even if patients initially appear fine,
they can deteriorate. Monitor closely. Pulmonary edema often occurs due to
aspiration, hypoxia, and other factors. It may not be evident for several hours
after near-drowning.
C. Beware of neck injuries - they often go unrecognized. Collar and backboard
straps can be applied in the water.
D. If patient is hypothermic, defibrillation and pharmacologic therapy may be
unsuccessful until the patient is rewarmed. Prolonged CPR may be needed.
E. Under current ACLS standards, Heimlich maneuver is not indicated.
Go to Table of Contents
4053
HYPOTHERMIA AND FROSTBITE
Specific Information Needed
A.
B.
C.
D.
E.
F.
Length of exposure
Air temperature, water temperature, winds, patient wet?
History and timing of changes in mental status
Drugs: alcohol, tranquilizers, anticonvulsants, others
Medical problems: diabetes, epilepsy, alcoholism, etc.
With local injury: history of thawing/refreezing?
Specific Objective Findings
A. Vital signs, mental status, shivering. (Prolonged observation for 1-2 min. may be
necessary to detect pulse, respirations.)
B. Skin temperature (estimated); also note current temperature of environment
C. Evidence of local injury: blanching, blistering, erythema of extremities, ears,
nose
D. Cardiac rhythm
Treatment
A. Generalized:
1. CPR, if no pulse
2. Administer oxygen. Assist with bag-valve-mask as needed.
3. Use appropriate airway adjunct only to protect airway or in absence of
organized cardiac electrical activity.
4. Avoid unnecessary suctioning or airway manipulation.
5. Remove wet or constrictive clothes from patient. Wrap in blankets and
protect from wind exposure. Increase ambient temperature in ambulance.
6. Attempt defibrillation, if appropriate, up to 3 shocks.
IV
7. Establish venous access. Solution should be warmed if possible. Do not
start IV until patient is moved to transport vehicle.
IN
8. Monitor cardiac rhythm.
IN
CB
9. No more than one round of ACLS drugs should be administered to a
hypothermic patient in the prehospital setting.
B. Local (frostbite):
1. Remove wet or constricting clothing. Keep skin dry and protected from wind.
2. Do not allow the limb to thaw if there is a chance that limb may refreeze
before evacuation is complete, or if patient must walk to transportation.
3. Rewarm minor "frostnip" areas by placing in axilla or against trunk under
clothing.
4. Dress injured areas lightly in clean cloth to protect from pressure, trauma or
friction. Do not rub. Do not break blisters.
5. Maintain core temperature by keeping patient warm with blankets, warm
fluids, etc.
6. Transport with frostbitten areas supported and elevated if feasible.
Go to Table of Contents
Specific Precautions
A. HYPOTHERMIA:
1. Shivering does not occur below 90˚ Fahrenheit. Below this the patient may
not even feel cold, and occasionally will even undress and appear
vasodilated.
2. The heart is most likely to fibrillate below 85-88˚ Fahrenheit. Defibrillation
should be attempted with no more than 3 shocks. Prolonged CPR may be
necessary until the temperature is above this level.
3. ALS drugs should be used sparingly, since peripheral vasoconstriction may
prevent entry into central circulation until temperature is restored. At that
time, a large bolus of unwanted drugs may be infused into the heart.
4. Bradycardias are normal and should not be treated.
5. If patient has organized monitor rhythm, CPR is currently felt to be
unnecessary. In general, even very slow rates are probably sufficient for
metabolic demands. CPR is indicated for asystole and ventricular fibrillation.
6. Patients who appear dead after prolonged exposure to cold air or water
should not be pronounced "dead" until they have been rewarmed. Full
recovery from hypothermia with undetectable vital signs, severe bradycardia,
and even periods of cardiac arrest has been reported.
7. Rewarming should be accomplished with careful monitoring in a hospital
setting, whenever possible.
8. Consider other reasons for altered mental status.
B. FROSTBITE:
1. Thawing is extremely painful and should be done under controlled conditions,
preferably in the hospital. Careful monitoring, pain medication, prolonged
rewarming, and sterile handling are required.
2. It is clear that rewarming followed by refreezing is far more injurious to
tissues than delay in rewarming or walking on a frozen extremity to reach
help. Do not rewarm prematurely. Indications for field rewarming are almost
nonexistent.
3. Warming with heaters or stoves, rubbing with snow, drinking alcohol and
other methods of stimulating the circulation are dangerous and should not be
used.
Return to Table of Contents
4054
HYPERTHERMIA
Specific Information Needed
A. Patient age, activity level
B. Medications: depressants, tranquilizers, alcohol, etc.
C. Associated symptoms: cramps, headache, orthostatic symptoms, nausea,
weakness
Specific Objective Findings
A. Vital signs: temperature; usually 104 degrees Fahrenheit or greater (if
thermometer available)
B. Mental status: confusion, coma, seizures, psychosis
C. Skin flushed and warm to hot: with or without sweating
D. Air temperature and humidity; patient dress
Treatment
A.
B.
C.
D.
E. Establish venous access:
1. TKO if vital signs stable
2. IV fluid bolus of 20 ml/kg if signs of hypovolemia.
IV
IN
Use appropriate airway adjuncts as indicated.
Remove clothing.
Administer oxygen.
Cool with water-soaked sheets.
CB
F. Treat seizures with diazepam 1-10 mg slow IV push.
G. If unable to obtain venous access after two attempts administer midazolam 1-5
mg IM.
P
H. Monitor cardiac rhythm.
.
Specific Precautions
A. Heat stroke is a medical emergency. It is distinguished by altered level of
consciousness. Sweating may still be present, especially in exercise-induced
heat stroke. The other persons at risk for heat stroke are the elderly and persons
on medications which impair the body's ability to regulate heat.
B. Differentiate heat stroke from heat exhaustion (hypovolemia of more gradual
onset) and heat cramps (abdominal or leg cramps). Be aware that heat
exhaustion can progress to heat stroke.
C. Do not let cooling in the field delay your transport. Cool patient as possible
while en route.
D. Do not use ice water or cold water to cool patients, as these may induce
vasoconstriction.
Go to Table of Contents
4055
BITES AND STINGS
Specific Information Needed
A. Type of animal or insect.
B. Time of exposure.
C. Symptoms:
1. Local: pain, stinging
2. Generalized: dizziness, weakness, itching, trouble breathing, muscle cramps
D. History of previous exposures, allergic reactions
Specific Objective Findings
A. Identification of spider, bee, marine animal if possible
B. Local signs: erythema, swelling, heat in area of bite
C. Systemic signs: hives, wheezing, respiratory distress, abnormal vital signs
Treatment
A. SNAKES: See Snake Bites.
B. SPIDERS:
1. Ice for comfort
2. Bring in spider, if captured and contained or if dead, for accurate
identification, if possible.
3. Transport for observation if systemic signs and symptoms present.
C. BEES AND WASPS:
1. Remove sting mechanism. Do not squeeze venom sac if this remains on
stinger, rather, scrape with straight edge.
2. Observe patient for signs of systemic allergic reaction. Treatment per the
Allergy/Anaphylaxis protocol and transport rapidly if needed
3. Transport all patients with systemic symptoms or history of systemic
symptoms from prior bites.
Specific Precautions
A. For all types of bites and stings, the goal of prehospital care is to prevent further
inoculation and to treat allergic reactions.
B. Allergy kits consist of injectable epinephrine and oral antihistamine, and are
prescribed for persons with known systemic allergic reactions. Prehospital care
personnel need not contact the resource hospital before assisting the patient with
their own medication.
C. About 60% of patients who have experienced a generalized reaction to a bite or
sting in the past will have a similar or more severe reaction upon reinoculation.
Thus, although it is not inevitable, this group of patients must be considered at
high risk for anaphylaxis. In addition, a small group of patients will have
anaphylaxis as a "first" reaction.
D. Time since envenomation is important. Anaphylaxis rarely develops more than
60 minutes after inoculation.
Go to Table of Contents
4056
SNAKE BITES
Specific Information Needed
A.
B.
C.
D.
Appearance of snake (e.g. rattle, color, banding)
Time of bite
Prior first-aid by patient or friends
Symptoms: local pain and swelling, peculiar or metallic taste sensations. Severe
envenomations may result in hypotension, coma, and bleeding.
Specific Objective Findings
A. Bite wound: location, configuration (1, 2, or 3 fang marks; entire jaw imprint,
none)
B. Snake identification: look for elliptical pupils, thermal pit and rattle
C. Signs of envenomation: spreading numbness and tingling from the site, local
edema and pain, ecchymosis, bleeding, hypotension. Mark time and extent of
erythema and edema with pen.
Treatment
A.
B.
C.
D.
E.
F.
G.
Remove patient and rescuers from area of snake to avoid further injury.
Remove rings or other bands which may become tight with local swelling.
Immobilize bitten part at heart level.
Minimize venom absorption by keeping bite area still and patient quiet.
Transport promptly for definitive observation and treatment.
Do not use ice or refrigerants.
For all suspected envenomations establish venous access and administer
oxygen.
H. Monitor vital signs, cardiac rhythm, and swelling.
Specific Precautions
A. The prairie rattlesnake is native to the Denver metro region. If the snake is dead,
bring it in for examination. Do not jeopardize fellow rescuers by attempting to
"round it up." Be careful: a dead snake may still reflexively bite and
envenomate. Do not pick up with hands, even if dead. Use a shovel or stick.
B. At least 25% of poisonous snake strikes do not result in envenomation.
Conversely, the initial appearance of the bite may not reflect the severity of
envenomation.
C. Fang marks are characteristic of pit viper bites, such as from the rattlesnake,
water moccasin, or copperhead, which are native to North America. Jaw prints
(without fangs) are more characteristic of nonvenomous species.
D. Ice can cause serious tissue damage. Never use!
E. Exotic poisonous snakes, such as those found in zoos, have different signs and
symptoms than those of pit vipers.
Go to Table of Contents
4060
SHOCK: MEDICAL
Specific Information Needed
A. Onset: gradual or sudden; precipitating cause or event
B. Associated symptoms: itching, peripheral or facial edema, thirst, weakness,
respiratory distress, abdominal or chest pain, dizziness on standing
C. History: allergies, medications, blood in vomitus or stools, significant medical
diseases, history of recent trauma, last menstrual period, vaginal bleeding, fever
Specific Objective Findings
A.
B.
C.
D.
E.
Vital signs: pulse > 120 (occasionally < 50); Systolic BP < 90 mmHg
Mental status: apathy, confusion, restlessness, combativeness
Skin: flushed, pale, sweaty, cool or warm, hives, or other rash
Signs of trauma
Signs of cardiogenic shock: jugular venous distention in upright position, rales,
peripheral edema
F. In children <8 years old, 2 or more of the following signs: tachycardic for age,
diminished capillary refill, thready pulses, cool extremities, poor color, altered
mental status, diminished respiratory effort
Treatment
A. Administer oxygen.
B. Cover patient to avoid excess heat loss. Do not over bundle.
C. Assess for cardiogenic cause:
IN
1. If pulse is > 150 treat tachyarrhythmia according to protocol.
2. If pulse is < 60 treat bradyarrhythmia according to protocol.
3. If distended neck veins, chest pain, or other evidence of cardiac cause:
a. Position of comfort
b. Be prepared to assist ventilations or initiate CPR.
c. Evaluate for possible tension pneumothorax
IV
d. Establish venous access.
IN
e. Monitor cardiac rhythm.
P
D. Consider dopamine.
E. Transport rapidly for definitive diagnosis and treatment.
F. If no evidence of cardiogenic cause, institute general treatment measures:
1. Place patient supine, elevate legs 10-12 inches. (If respiratory distress
results, leave patient in position of comfort.)
IV
2. Establish venous access.
3. Administer IV Fluid bolus of normal saline.
G. Assess and treat for specific cause, such as anaphylaxis, if this can be
determined.
Go to Table of Contents
H. Monitor vital signs, cardiac rhythm, and level of consciousness during transport.
Specific Precautions
A. Shock in a cardiac patient may be caused by hypovolemia; however, contact
should be made with base prior to administering fluid boluses.
B. Mixed forms of shock are treated as hypovolemia, but the other factors
contributing to the low perfusion should be considered. Neurogenic shock is
caused by relative hypovolemia as blood vessels lose tone, either from spinal
cord trauma, drug overdose, or sepsis. Cardiac depressant factors can also be
involved. Anaphylaxis is a mixed form of shock with hypovolemic, neurogenic,
and cardiac depressant components. Epinephrine is used in addition to fluid
load.
C. Cardiogenic shock from various causes is difficult to treat even in a hospital
setting. Rapid transport is recommended.
SHOCK: MEDICAL
Mechanism/Causes
HYPOVOLEMIA
Dehydration
Vomiting, diarrhea
Diabetes with hyperglycemia
Ectopic pregnancy
GI bleed
Ruptured abdominal aneurysm
Vaginal bleeding
Intra-abdominal bleeding
CARDIOGENIC
Arrhythmia
Pericardial tamponade
Tension pneumothorax
Myocardial failure
Pulmonary embolus
MIXED
Sepsis symptoms
Drug overdose
Anaphylaxis
Return to Table of Contents
Differential/Symptoms
suggestive illness
Diabetes; acute illness, increased urine or blood
loss, thirst, fever
female, 12-50 years, abdominal pain
bloody vomitus, black or red stool
severe back/abdomen pain, age, history of high
blood pressure
suggestive history, miscarriage, abortion or
delivery
minor trauma; abdominal, back, or shoulder pain
palpitations
chest area cancer, blunt or penetrating trauma
respiratory distress, COPD, trauma
chest pain, history of congestive failure
sudden respiratory distress, chest pain, SOB
fever, elderly, urinary symptoms
suggestive history
SOB, itching, mouth swelling, dizziness, exposure
to allergen
4070
PSYCHIATRIC/BEHAVIORAL
Specific Information Needed
A. Obtain history of current event, inquire about recent crisis, toxic exposure, drugs,
alcohol, emotional trauma, suicidal or homicidal ideation
B. Obtain past history; inquire about previous psychiatric and medical problems,
medications.
Specific Objective Findings
A.
B.
C.
D.
Evaluate vital signs.
Note medic alert tags, odor to breath.
Determine ability to relate to reality.
Note hallucinations and behavior.
Treatment
A.
B.
C.
D.
Attempt to establish rapport.
Assure airway.
Restrain if necessary.
Chemical restraint if needed
a. Midazolam (Versed)
b. Diphenhydramine 50mg as a synergist (not stand alone treatment)
OR
c. Diazepam 1-10mg slow IVP
d. DO NOT USE BOTH VERSED AND DIAZEPAM ON THE SAME
PATIENT
E. Monitor vital signs.
F. If altered mental status or unstable vital signs:
1. Administer oxygen.
2. Establish venous access.
3. Draw appropriate blood tubes.
4. Administer dextrose 25 gm (50 ml of a 50% solution), IV bolus if blood
glucose <60 and if clinically indicated.
5. Administer naloxone up to 2 mg IV or IN (may also be administered IM or IO)
in patients with decreased respiratory effort and observe patient for improved
ventilations. (EMT-IV can only give naloxone IV or IN)
6. If EMT-IV, contact base for consideration of administration of Naloxone as
described above
7. If venous access is unsuccessful and unable to administer dextrose,
administer Glucagon 1 mg, IM.
IV
IN
CB
8. Consider Diazepam 1-10 mg slow IV bolus for stimulant use.
Specific Precautions
P
A. Psychiatric patients often have an organic basis for mental disturbances.
Beware of hypoglycemia, hypoxia, head injury, intoxication, or toxic ingestion.
B. If emergency treatment is unnecessary, do as little as possible except to
reassure while transporting. Try not to violate the patient's personal space.
Go to Table of Contents
C. If the situation appears threatening, consider a show of force involving police
before attempting to restrain.
D. Beware of weapons. These patients can become very violent.
E. The paramedic may initiate a Mental Health Hold only with the permission and
online contact with the BASE PHYSICIAN.
Return to Table of Contents
4080
OBSTETRICS/GYNECOLICAL EMERGENCIES
Specific Information Needed
A. Symptoms: pain, cramping, passage of clots or tissue, dizziness, weakness; if
pregnant, inquire about swelling of face and extremities, urge to push,
contractions (regularity and timing), ruptured membranes, fever
B. Obtain menstrual history: last normal menstrual period, duration of period,
amount of flow, birth control method
C. If pregnant, inquire about due date, prior problems with pregnancy.
D. Past and present history of hypertension (preeclampsia/eclampsia)
E. Past history: bleeding problems, pregnancies, medications, allergies
Specific Objective Findings
A. Vital signs and orthostatic changes
B. Evidence of blood loss, clots or tissue fragments; bring tissue to the ED
C. Signs of hypovolemic shock, altered mental status, hypotension, tachycardia,
sweating, pallor
D. Fever
E. If pregnant, observe for contractions and relaxation of uterus. Where privacy is
possible, examine perineum by observation only for:
1. Vaginal bleeding or fluid (note color)
2. Crowning (check during contraction)
3. Abnormal presentation (i.e. foot, arm, face, or cord)
Treatment
A. If patient is bleeding vaginally (moderate to heavy):
1. Administer oxygen.
2. If hypotensive and pregnant, position onto left side.
IV
3. Establish venous access.
4. If hypotensive, give IV fluid bolus of normal saline, further fluids as directed
and consider a second line.
B. If patient is delivering:
1. Use clean or sterile technique.
2. Administer oxygen.
3. Guide and control but do not retard or hurry the delivery.
4. Suction the mouth (not throat) then nose with a bulb syringe.
5. Protect the infant from fall and temperature loss; wipe off amniotic fluid and
wrap in a clean or sterile blanket, check vital signs, provide CPR as indicated.
6. Clamp the umbilical cord in two places approximately 8-10" from the infant.
7. Cut the cord between the clamps.
IV
8. Establish venous access in mother and monitor vital signs.
9. Do not wait for or attempt delivery of placenta before transporting. If placenta
delivers spontaneously bring it to the hospital.
Go to Table of Contents
C. If patient is bleeding in the postpartum period (within 24 hours of delivery):
1. Massage uterus and have mother nurse infant to aid in uterine contractions.
2. Administer oxygen.
3. Establish venous access.
IV
Specific Precautions
A. If patient is in late pregnancy and there is crowning or other indication of
imminent delivery, deliver or transport. Be prepared to stop ambulance for
delivery while enroute.
B. Amount of vaginal bleeding is difficult to estimate. Try to get an estimate of
number of saturated pads in previous 6 hours.
C. Transport immediately any pregnant patient with an abnormal presenting part or
vaginal bleeding.
D. A patient in shock from vaginal bleeding should be treated like any other patient
with hypovolemic shock.
E. If patient is pregnant, bring in any tissue that was passed. Laboratory analysis
may be important in determining status of pregnancy.
F. Always consider pregnancy as a cause of vaginal bleeding. The history may
contain inaccuracies, denial, or wishful thinking.
G. If the patient is pregnant, ask if she feels as though she is delivering. Particularly
with prior deliveries, most mothers will know.
H. The primary enemy of newborns is hypothermia, which can occur within minutes
due to increased evaporative heat loss resulting from the infant's large body
surface area and the presence of amniotic fluid.
I. Record an APGAR score with vital signs, at one and five minutes.
IN
J. Consider early tracheal suctioning after delivery of the infant with evidence of
meconium.
APGAR Score
Sign
0
1
2
Muscle tone (Activity)
Pulse
Limp
Absent
Some flexion
<100/min
Active, good flexion
=100/min
Reflex irritability*
(Grimace)
Color (Appearance)
No response
Cough, cry or sneeze
Respirations
Absent
Some grimace or
avoidance
Pink body, blue
hands/feet
Slow, irregular,
ineffective
Blue, pale
*Nasal or oral suction catheter stimulus
Return to Table of Contents
Pink
Crying, rhythmic, effective
4090
EXCITED DELIRIUM
Purpose
Excited Delirium is a potentially lethal medical condition that often presents itself
as a law enforcement issue. This protocol is to guide EMS interaction with persons who
present with excited delirium.
General Principles
Excited Delirium seems to be a commonality in patients suffering cardiac arrest
after struggling with law enforcement, EMS or hospital staff. Patients who seem to be
prone to Excited Delirium generally fall into one of three categories.
1. Those suffering from psychiatric illness, eg., schizophrenia or bipolar disorder
2. Illicit substance users, especially stimulant drugs such as cocaine and
methamphetamine, and chronic alcohol abusers
3. A combination of mental illness and substance abuse
The patient presents with bizarre, violent behavior that usually leads them to be
contacted by law enforcement. There are often acts of aggression against persons or
property, with particular affinity to shiny, inanimate objects and may include breaking
glass. They are further found to be paranoid, often shout incoherently; They don’t seem
to be able to effectively communicate. They appear to be impervious to pain. As a result,
traditional methods of gaining compliance using pain are often ineffective. Often they
demonstrate superhuman strength and can battle multiple people for long periods of
time. They are almost always hyperthermic. These patients tend to disrobe and are often
found fully unclothed. Patients seem to follow a pattern that culminates in full cardiac
arrest preceded by a period of calm, listlessness that may be mistaken as compliance.
When patients progress to full arrest, they are most times refractory to treatment.
Procedure
1. Be aware of the signs and symptoms of Excited Delirium
2. Be prepared for the patient to have a full cardiac arrest, particularly if they
suddenly become calm.
3. Consider Midazolam (Versed) or Diazepam (Valium) for chemical restraint.
4. If at all possible, keep the patient supine while attempting to control them
5. Keep in mind that these patients will not respond to pain
6. As soon as it is feasible, begin continuous monitoring of vital signs, EKG,
SpO2, and ETCO2
7. There is conjecture that hypoventilation is ultimately what causes the cardiac
arrest so be prepared to assist in ventilations in patients who suddenly
become calm even though they have a patent airway.
Special Notes
1. While these patients will generally declare themselves, it is imperative that they
are transported by Advanced Life Support.
2. Law enforcement may request that the patient go to jail but responders must
reinforce that this is a significant medical problem that requires ALS transport.
3. It is not uncommon for these patients to have been exposed to a Conducted
Energy Weapon such as a Taser, multiple times.
4. Current reports are showing possible links that Taser use in conjunction with
excited delirium increases mortality.
See Protocol: Taser
Go to Table of Contents
5000
MULTIPLE TRAUMA OVERVIEW
Specific Information Needed
A. Mechanism of injury:
1. Cause, precipitating factors, weapons used
2. Trajectories and forces involved
3. For vehicular trauma:
a. Specific description of mechanism such as auto vs. pole, rollover,
broadside, high speed
b. Condition of vehicle including windshield, steering wheel, compartment
intrusion, condition of dashboard/firewall/pedals, type and use of
seatbelts, supplemental restraint system (e.g. airbag) deployment
4. Helmet use; motorcycle, bicycle, skiing, snowboarding, skateboarding,
rollerblading
B. Patient complaints.
C. Initial position and level of consciousness of patient.
D. Patient movement, treatment since injury
E. Other factors such as drugs, alcohol, medications, diseases, pregnancy
Specific Objective Findings
A. Scene evaluation:
1. Note potential hazard to rescuers and patient.
2. Identify number of patients; organize triage operations if appropriate
3. Observe position of patient, surroundings, probable mechanism, and vehicle
condition.
B. Patient evaluation: see treatment below
Treatment
A.
B.
C.
D.
E.
Initial assessment in multiple trauma is performed at the same time as treatment.
Airway with spinal precautions and immobilization
Breathing
Circulation, with control of major bleeding
Transport decision
1. If patient unstable, transport immediately. Treat enroute.
2. If patient stable, assess for potentially life-threatening injuries and treat
accordingly.
F. Monitor vital signs, neurologic status and cardiac rhythm enroute.
G. CONTACT BASE.
Specific Precautions
A. Assessment and management of trauma in the field has changed considerably in
the past 5 years. There are patients who cannot tolerate a full assessment before
life saving intervention is needed. Likewise, splinting, bandaging, and, often, the
focused history and physical examination are procedures that may need to be
bypassed in the critical patient. Time and the treatment available in a trauma
center are critical elements in resuscitation. Therefore, with severely injured
patients, it is most appropriate to rapidly transport (“load and go”) the patient
Return to Table of Contents
B.
C.
D.
E.
rather than using extended stabilization or the old "grab and run," with no trauma
stabilization or care rendered.
Critical injuries involve:
1. Difficulty with respiration.
2. Difficulty with circulation (hypoperfusion a.k.a. shock).
3. Decreased level of consciousness.
4. Any trauma patient with one or more of these above conditions is a "load and
go," with treatment occurring enroute.
Even in the noncritical patient with significant injury, "stabilization in the field"
does not occur. With major injuries, the very most you can do is to buy time. If
the initial bolus of fluids results in improved vitals, do not become complacent.
This patient frequently needs blood and an operating room to truly "stabilize" the
traumatic process. Rapid transport is still the highest priority.
Serial vital signs and observations of respiratory, circulatory and neurologic
status prior to arrival are critical.
The trauma patient is the greatest risk to the rescuer for exposure to "bodily
fluids." Use all appropriate body substance isolation precautions.
Return to Table of Contents
5010
TRAUMA ARREST
Specific Information Needed
A. Time of arrest
B. Mechanism: blunt vs. penetrating
C. Signs of irreversible death (decapitation, dependent lividity, etc.)
Specific Objective Findings
A. Vital signs
B. Evidence of massive external blood loss
C. Evidence of massive blunt head, thorax or abdominal trauma
Treatment
A. Blunt trauma arrest:
1. Initiate basic life support
2. Use appropriate airway adjuncts as indicated. Administer oxygen.
3. If no vital signs or other signs of life present after above treatments, consider
field pronouncement.
4. If pulse returns with above treatment, treat per protocol and transport rapidly
to a Level I or II trauma center.
5. CONTACT BASE.
B. Penetrating trauma arrest:
6. Initiate basic life support
1. Use appropriate airway adjuncts as indicated. Administer oxygen
2. Begin rapid transport.
3. CONTACT BASE to report patient status.
IV
4. Establish venous access, administer IV fluid bolus of normal saline.
5. If cardiac activity returns with above treatment, treat arrhythmias per
protocols.
6. Consider field pronouncement (See Resuscitation and Field Pronouncement)
Guidelines for the following:
a. Signs of irreversible death
b. ALS has been unavailable for at least 20 minutes from the time EMS
personnel initiate on-scene assessment and there is no return of vital
signs or signs of life
Specific Precautions
A. Victims of blunt trauma arrest without vital signs at the scene after initiation of
ALS have a mortality rate of nearly 100%.
B. Trauma arrests secondary to penetrating truncal injuries can be resuscitated and
saved. There is a higher rate of survival in victims of low velocity penetrating
injuries versus victims of high velocity injuries.
Go to Table of Contents
5020
AMPUTATIONS
Specific Information Needed
History: time and mechanism of amputation; care for severed part prior to rescuer
arrival
Past history: medications, bleeding disorders, medical problems
Specific Objective Findings
A.
B.
C.
D.
Vital signs
Other injuries
Blood loss at scene
Structural attachments in partial amputations if identifiable
Treatment
A.
B.
C.
D.
IV
Manage airway and breathing
Resuscitate and treat other more urgent injuries.
Control hemorrhage with direct pressure, elevation.
If hypotension or signs of shock:
1. Establish venous access.
2. Fluid bolus: normal saline
3. CONTACT BASE.
E. Patient: gently cover stump with sterile dressing. Saturate with sterile saline.
Cover with dry dressing. Elevate.
F. Severed part: wrap in sterile gauze, preserving all amputated material. Moisten
with sterile saline. Place in watertight container (specimen cup, plastic bag, etc).
Place container in cooler with ice (do not freeze).
G. CONTACT BASE for optimal transport destination.
Specific Precautions
A. Partial amputations should be dressed and splinted in alignment with extremity to
ensure optimum blood flow. Avoid torsion in handling and splinting.
B. Do not use dry ice to preserve severed part.
C. Control all bleeding by direct pressure only to preserve tissues. The most
profuse bleeding may occur in partial amputations, where cut vessel ends cannot
retract to stop bleeding. Never clamp bleeding vessels.
D. Many factors enter into the decision to attempt replantation (age, location,
condition of tissues, other options). A decision regarding treatment cannot be
made until the patient and part have been examined by a physician and may not
be made at the primary care hospital. Try to help the family and patient
understand this, and don't falsely elevate hopes.
Go to Table of Contents
5030
HEAD TRAUMA
Specific Information Needed
A. History: mechanism of injury, estimate of force involved; helmet use.
B. History since injury: loss of consciousness (duration), change in level of
consciousness, memory loss for events before and after trauma, movement
(spontaneous or moved by bystanders), seizure activity
C. Past history: medications (esp. insulin), medical problems, seizure history,
alcohol or drug use
Specific Objective Findings
A. Vital signs (note respiratory pattern and rate)
B. Neurologic assessment: Glasgow Coma Score
C. External evidence of trauma: contusions, abrasions, lacerations, drainage from
nose, ears
Treatment
A. Assess airway and breathing; treat life threatening conditions. Use assistant to
provide in-line cervical immobilization when indicated, while managing respiratory
difficulty.
B. Administer oxygen.
C. Control hemorrhage. Stop scalp bleeding with direct pressure. Continued
pressure may be needed.
D. TRANSPORT RAPIDLY if patient has multiple injuries, or unstable neurologic,
respiratory or circulatory status.
E. Obtain initial vital signs, neurologic assessment.
F. If unconscious:
1. Assist ventilations.
2. Consider airway adjuncts
3. Ventilate at 10 breaths per minute for adults (15 breaths for children, 20
breaths for infants).
4. If signs of cerebral herniation are present, hyperventilate at 20 bpm for adults
(30 bpm for children, 35 bpm for infants).
5. CONTACT BASE.
G. Immobilize cervical, thoracic and lumbosacral spine when indicated.
H. If signs of hypovolemic shock are present, initiate treatment en route:
1. Establish venous access.
2. Fluid bolus of normal saline.
IV
I.
IV
3. Look carefully for possible sources of bleeding (abdomen, pelvis, chest).
4. CONTACT BASE.
If patient stable:
1. Establish venous access.
2. Complete detailed assessment.
3. Splint fractures and dress wounds if time permits.
Go to Table of Contents
J. Monitor and record airway, vital signs, and level of consciousness repeatedly at
scene and during transport. Status changes are important.
Specific Precautions
A. When head injury patients deteriorate, check first for airway, oxygenation and
blood pressure. These are the most common causes of "neurologic"
deterioration. If the patient has tachycardia or hypotension, evaluate for
hypovolemia from associated injuries.
B. Secondary brain injury and adverse outcomes can occur in brain-injured patients
who exhibit hypotension and/or hypoxia. Early aggressive treatment of
hypotension and administration of high flow oxygen may prevent further injury.
C. The most important information you provide for the base physician is level of
consciousness and its changes. Is the patient stable, deteriorating or improving?
D. Restlessness can be a sign of hypoxia. Cerebral anoxia is the most frequent
cause of death in head injury.
E. Hypoventilation aggravates cerebral edema.
F. Scalp lacerations can cause profuse bleeding, and are difficult to define and
control in the field. If direct local pressure is insufficient to control the bleeding,
evacuate any large clots from flaps and large lacerations with sterile gauze, and
use direct hand pressure to provide hemostasis. If the underlying skull is
unstable, pressure should be applied to the periphery of the laceration over intact
bone.
G. Routine prophylactic hyperventilation should be avoided. It has been shown to be
detrimental to cerebral blood flow and patient outcome. Hyperventilation in the
field for head trauma is indicated only when signs of cerebral herniation such as
extensor posturing or pupillary abnormalities (asymmetric or bilaterally fixed and
dilated pupils) are present after correcting hypotension and/or hypoxemia.
Return to Table of Contents
5040
FACE AND NECK TRAUMA
Specific Information Needed
A. Mechanism of injury: impact to steering wheel, windshield, or other objects;
clothesline type injury to face or neck; blunt object to head, face, or neck
B. Management before arrival by bystanders, first responders
C. Patient complaints: areas of pain; trouble with vision, hearing; neck pain; dental
occlusion, tooth loss; short of breath
D. Past medical history: medications, medical illnesses
Specific Objective Findings
A. Vital signs
B. Airway: jaw or tongue instability, loose teeth, vomitus or blood in airway, other
evidence of impairment or obstruction
C. Neck: tenderness, crepitation, hoarseness, bruising, swelling, stridor
D. Blood or drainage from ears, nose
E. Level of consciousness, evidence of head trauma
F. Injury to eye: lid laceration, blood anterior to pupil, abnormal pupil, abnormal
globe position
Treatment
A. Control airway with cervical spine immobilization if indicated:
1. Open airway using jaw thrust, keeping neck in alignment with in-line cervical
immobilization.
2. Use finger sweep to remove oral foreign bodies.
3. Suction blood and other debris.
4. Stabilize tongue and mandible with chin lift. Manual traction of the tongue
may be necessary to keep posterior pharynx open as needed.
5. Note evidence of laryngeal injury and transport immediately if signs present.
6. If bleeding is severe, attempt to manage with suctioning, oral airway, and
bag-valve-mask.
7. Support breathing as needed.
8. Use appropriate airway adjuncts as indicated.
IN
P
9.
If intubation cannot be performed due to severe facial injury, attempt to
manage with suctioning and bag-valve-mask.
10. If necessary, consider percutaneous cricothyrotomy
B. Administer oxygen.
C. Control hemorrhage, check pulse and circulation.
IV
D. Establish venous access:
1. TKO if stable
2. With signs of hypovolemia:
a. Fluid bolus of normal saline; CONTACT BASE.
Go to Table of Contents
E. Cover injured eyes with protective shield or cup; avoid pressure or direct contact
to eye.
F. Do not attempt to stop free drainage from ears, nose. Cover lightly with dressing
to avoid contamination.
G. Bring avulsed teeth with you. Keep moist in saline soaked gauze.
H. Monitor airway closely during transport for development of obstruction or
respiratory distress. Suction and treat as needed.
Specific Precautions
A. Fracture of the larynx should be suspected in patients with respiratory distress,
abnormal voice, and history of direct blow to neck from steering wheel, rope,
fence wire, etc. Both intubation and percutaneous cricothyrotomy may be
unsuccessful in the patient with a fractured larynx, and attempts may result in
increased injury. Transport rapidly for definitive treatment if you suspect this
potentially lethal injury. Do not attempt intubation or percutaneous
cricothyrotomy unless the patient is in severe respiratory distress. Bag-valvemask ventilation is preferred.
B. Airway obstruction is the primary cause of death in persons sustaining head and
face trauma. Meticulous attention to suctioning and basic airway maneuvers
may be the most important treatment rendered.
C. Remember that the apex of the lung extends into the lower neck and may be
injured in penetrating injuries of the lower neck, resulting in pneumothorax or
hemothorax.
D. Do not be concerned with contact lens removal in the field.
E. When midface fractures are suspected, nasotracheal intubation is
contraindicated.
F. No nasotracheal intubation under age 12.
Return to Table of Contents
5050
SPINAL TRAUMA
Specific Information Needed
A. Mechanism of injury and forces involved: be suspicious with falls, decelerations,
diving accidents and motor vehicle accidents.
B. Past medical problems and medications
Specific Objective Findings
A. Vital signs, including neurological assessment
B. Level of sensory and motor deficit; presence of any evidence of neurological
function below level of injury
C. Physical exam, with careful attention to organs or limbs which may not have
sensation
Treatment
A. Assess airway and breathing; treat life threatening difficulties. Use controlled
ventilation for high cervical cord injury associated with abdominal breathing. Use
assistant to provide in-line cervical immobilization while managing ABCs.
B. Administer oxygen.
C. Control hemorrhage.
D. Immobilize cervical, thoracic and lumbosacral spine as indicated.
E. Obtain and record vital signs and neurologic assessment before and after
immobilization.
IV
F. Establish venous access. If signs of hypovolemia: fluid bolus of Normal Saline,
CONTACT BASE
G. Monitor airway, vitals, and neurologic status frequently at scene and during
transport.
Specific Precautions
A. Be prepared to turn entire board on side if patient vomits (patient must be
secured to spine board or scoop stretcher).
B. Neurogenic shock is likely with significant spinal cord injury. If present, elevate
legs 10-12 inches. Ensure adequate respirations.
C. If hypotension is unresponsive to simple measures, it is likely due to other
injuries. Neurological deficits make other injuries hard to evaluate. Cord injury
above the level of T-8 makes the abdominal examination unreliable.
D. Spinal immobilization in patients with penetrating trauma should be accomplished
only when neurological deficit or impaled foreign body is present.
E. It is important from a clinical and medical legal perspective to record neurological
assessment before and after spinal immobilization.
Go to Table of Contents
5055
SELECTIVE SPINAL IMMOBILIZATION
The purpose of this protocol is to minimize unnecessary application of
spinal precautions in trauma or potential trauma patients.
Selective Spinal Immobilization may only be performed by EMTs or
Paramedics trained in this procedure, and approved by their medical
director.
1. Patients who meet the following criteria may be excluded from spinal precautions. All
other patients must be placed in spinal immobilization
2. This protocol is for the patient over the age of 12 and under the age of 60
Assessment - Mental Status, Speech and History
1. There is no complaint of neck or back tenderness or pain elicited either while
obtaining a history or from the physical exam.
2. The patient is reliable
3. There is no significant language barrier
4. There is no history or appearance of drug or alcohol ingestion.
5. The patient is alert and oriented to person, place, time and event.
6. The history and exam exclude mental retardation, senility, Alzheimer's disease,
stroke, significant closed head injury, anoxia or hypovolemia.
7. There is no distracting social or emotional situation in which the patient cannot
focus on his/her physical condition.
8. There is no potentially distracting injury such as a painful extremity or
abdominal injury.
Assessment - Physical
If at any time, pain or discomfort occurs as a result of the exam, stop the assessment
and immobilize the patient.
1. Palpate down the spinal cord including the occipital notch at the top and the sacrum at
the bottom.
2. Have the patient shrug their shoulders against resistance.
3. Have the patient turn their head against resistance.
4. Test for motor strength, weakness, numbness, tingling, focal deficits or other
paresthesias or discomfort by having the patient move each joint against resistance and
compare to the opposite side. Be methodical.
1.
2.
3.
4.
1.
2.
3.
4.
5.
6.
7.
Have the patient spread their fingers against your resistance
Have the patient squeeze your hands
Have the patient flex wrist against your resistance
Have the patient extend wrist against your resistance
Have the patient flex their elbow against your resistance
Have the patient extend their elbow against your resistance
Have the patient flex their hip
Have the patient extend their knee
Have the patient flex their knee
Have the patient dorsiflex their ankle
Have the patient plantar flex their ankle
Go to Table of Contents
If there is notable weakness, determine if the weakness if unilateral or bilateral.
Special Considerations
Do not use in the elderly over the age of 60. Arthritic spinal rigidity
and osteoporosis can result in increased risk of injury even with minor
mechanism such as a ground level fall. There is a high degree of
peripheral neuropathy in the elderly, therefore complaints of pain are
unreliable.
Being ambulatory does not exclude spinal immobilization.
If the patient does not meet these criteria for exclusion, spinal
immobilization should be applied. It is inappropriate to walk a patient to
the ambulance and have them lie down on a board.
Immobilization devices, once applied, may require re-adjustment while
maintaining alignment, but shall not be removed.
Once applied, immobilization devices shall only be removed by the
receiving facility physician.
A patient may refuse any treatment being rendered at any time. If a
patient is refusing spinal precautions, the risks involved must be
relayed and the proper documentation of the patients condition and
associated risks must be documented on a patient care report or
refusal form that the patient signs.
Patients immobilized on devices are prone to losing body heat. Keep
the patient warm.
Return to Table of Contents
5060
CHEST INJURY
Specific Information Needed
A. Patient complaints: chest pain type (pleuritic, positional, location sharp, dull, etc.)
respiratory distress, neck pain, other areas of injury.
B. Mechanism: amount of force involved (particularly deceleration), speed of impact,
seatbelt use/type, airbag.
C. Penetrating trauma: size of object, caliber of bullet, trajectory, distance from
patient.
D. Past medical history: medications, prior medical problems.
Specific Objective Findings
A. Observe: wounds, air leaks, chest wall movement, neck veins
B. Palpate: tenderness, crepitation, tracheal position, tenderness on sternal
compression, pulse pressure
C. Auscultate: breath sounds, heart sounds (quality)
D. Surroundings: vehicle, steering wheel condition, dashboard.
Treatment
A.
B.
C.
D.
E.
F.
Clear and open airway. Immobilize cervical spine, if indicated.
Use appropriate airway adjuncts as indicated.
Assist breathing if patient is apneic or respirations depressed.
Administer oxygen.
If penetrating injury present, transport rapidly with further stabilization en route.
For open chest wound with air leak, use Vaseline type gauze or occlusive
dressing taped on three sides only, to allow air to escape but not enter the chest.
G. Observe chest for paradoxical movements.
H. Obtain baseline vital signs, neurologic assessment.
1. If the patient is in shock transport rapidly to a trauma center and CONTACT
BASE.
IV
IN
2. If neck veins flat and patient in shock, transport rapidly and treat hypovolemia
en route:
a. Establish venous access.
b. Fluid bolus: normal saline
c. Monitor cardiac rhythm.
3. If patient in shock with neck veins distended, also transport rapidly, and
consider:
a. Tension pneumothorax if respiratory status markedly deteriorating
with clinical findings of pneumothorax:
i. Release occlusive dressings on open chest wounds.
P
ii. Needle decompression; CONTACT BASE for orders
b. Pericardial tamponade, if suggested by clinical findings (distant heart
sounds, narrow pulse pressure):
Return to Table of Contents
i. Establish venous access.
ii. Fluid bolus: normal saline
IV
c. Cardiac contusion with typical ischemic chest pain or severe chest
wall contusion:
i. Monitor cardiac rhythm.
IN
4. If patient stable without signs or symptoms of shock:
a. Complete focused assessment.
b. If significant injury suspected:
i. Establish venous access.
IV
IN
ii. Monitor cardiac rhythm en route.
Immobilize impaled objects in place with dressings to prevent movement. Large
objects may require manual stabilization during transport.
J. Monitor and record vital signs, and level of consciousness every five minutes with
significant injury.
I.
Specific Precautions
A. Chest trauma is treated with difficulty in the field and prolonged treatment before
transport is not indicated if significant injury is suspected. If patient is critical,
transport rapidly and avoid treatment of nonemergent problems at the scene.
Penetrating injury particularly should receive immediate transport with minimal
intervention in the field.
B. Consider medical causes of respiratory distress such as asthma, pulmonary
edema or COPD that have either caused trauma or been aggravated by it.
C. Chest injuries sufficient to cause respiratory distress are commonly associated
with significant blood loss. Consider hypovolemia.
D. Myocardial contusion can occur, particularly with sudden deceleration injury, as
from a steering wheel. Pain is similar to myocardial infarct pain. Monitor the
patient and treat arrhythmias as in a medical patient, but think first of hypoxia and
hypovolemia as potential causes of arrhythmias.
E. Check the back for injuries, especially the patient in shock, where a cause is not
evident (check the back, axillary region and base of neck).
F. Significant intrathoracic injuries can exist without external signs of injury.
Return to Table of Contents
5070
ABDOMINAL TRAUMA
Specific Information Needed
A. Patient complaints
B. For penetrating trauma: weapon, trajectory
C. For auto: condition of steering wheel, dash, vehicle; speed, patient trajectory;
seatbelts in use, airbag deployment
D. Past history: medical problems, medications, pregnancy, drugs, alcohol
Specific Objective Findings
A. Observe: distention, bruising, entrance/exit wounds
B. Palpate: areas of tenderness, guarding; pelvis stability to lateral and suprapubic
compression
Treatment
A. Stabilize life threatening airway and circulatory problems first.
B. Administer oxygen.
C. Observe carefully for signs of blood loss. If signs of shock:
1. Rapid transport
IV
2. Establish venous access. Consider second IV using large bore catheter.
3. Administer fluid bolus of normal saline if clinically indicated; further fluids as
directed.
4. CONTACT BASE.
D. For penetrating injuries: cover wounds and eviscerations with moist saline gauze
to prevent further contamination and drying. Do not attempt to replace.
E. Monitor vital signs during transport.
Special precautions
A. The extent of abdominal injury is difficult to assess in the field. Be very
suspicious; with significant blunt trauma, injuries to multiple organs are the rule.
B. Patients with spinal cord injury, altered sensorium due to drugs or alcohol, head
injury or significant distracting injuries (i.e. long bone fractures) may not complain
of tenderness and may lack guarding in the face of significant intra abdominal
injury.
C. Seatbelts, steering wheels, and other blunt objects may cause occult intra
abdominal injury that is not apparent until several hours after the trauma. You
must consider forces involved to properly assess and treat a trauma victim.
D. In children, significant intra-abdominal injury, which may lead to shock, may be
present without any external signs of injury, such as abrasions or hematomas.
E. The pregnant patient deserves special attention during transport. Transport the
patient on her side or angle backboard to prevent Supine Hypotension Syndrome
from uterine compression of the inferior vena cava.
Go to Table of Contents
5080
EXTREMITY INJURIES
Specific Information Needed
A. Mechanism of injury: direction of forces, if known
B. Areas of pain, swelling or limited movement
C. Treatment prior to arrival: realignment of open or closed fracture, or dislocations,
movement of patient
D. Past medical history: medications, medical illnesses
Specific Objective Findings
A. Vital signs
B. Observe: localized swelling, discoloration, angulation, lacerations, exposed bone
fragments, loss of function, guarding
C. Palpate: tenderness, crepitation, instability, quality of distal pulses, sensation
D. Note estimated blood loss at scene.
Treatment
A. Treat airway, breathing, and circulation as first priorities.
B. Immobilize cervical spine when appropriate.
C. Examine for additional injuries to head, face, chest, and abdomen; treat those
problems with higher priority first.
D. If patient unstable, transport rapidly, treating life threatening problems en route.
Splint patient to minimize fracture movement by securing to long board.
E. If patient stable, or isolated extremity injury exists:
1. Check and record distal pulses and sensation prior to immobilization of
injured extremity.
2. Apply sterile dressing to open fractures. Note carefully wounds that appear
to communicate with bone.
3. Splint areas of tenderness or deformity: apply gentle traction throughout
treatment and try to immobilize the joint above and below the injury in the
splint.
4. Realign angulated fractures by applying gentle axial traction if indicated:
5. To restore circulation distally
6. To immobilize adequately, i.e., realign femur fracture
7. Check and record distal pulses and sensation after reduction and splinting.
8. Elevate simple extremity injuries. Apply ice pack if time and extent of injuries
allow.
9. Monitor circulation (pulse and skin temperature), sensation, and motor
function distal to site of injury during transport.
10. Establish venous access.
IV
IN
CB
11. Consider Morphine Sulfate 2-10 mg, IV bolus for pain control
OR
Consider Fentanyl, 1-2 mcg/kg, slow IV bolus for pain control.
Go to Table of Contents
Special precautions
A. Patients with multiple injuries have a limited capacity to recognize areas which
have been injured. A patient with a femur fracture may be unable to recognize
that he has other areas of pain. Be particularly aware of missing injuries
proximal to the obvious ones (e.g., a hip dislocation with a femur fracture, or a
humerus fracture with a forearm fracture).
B. Do not use ice or cold packs directly on skin or under air splints. Pad with towels
or leave cooling for hospital setting.
C. Do not attempt to realign angulated fractures in the field unless circulation is
compromised. Splint in the position of comfort.
D. Injuries around joints may become more painful and circulation may be lost with
attempted realignment. If this occurs, stabilize the limb in the position of most
comfort with the best distal circulation.
Return to Table of Contents
5090
BURNS
Specific Information Needed
A. History of injury: time elapsed since burn. Was patient in a closed space with
steam or smoke? Electrical contact? Loss of consciousness? Accompanying
explosion, toxic fumes, other possible trauma?
B. Past history: prior cardiac or pulmonary disease, medications?
Specific Objective Findings
A. Vital signs
B. Extent of burns: description or diagram of areas involved
C. Depth of burns: superficial - erythema only; partial or full thickness - blistered or
charred areas. Estimate size of burn. Use Rule of Nines or area of one patient
palm = 1% burn.
D. Evidence of carbon monoxide poisoning or other toxic inhalation: altered mental
state, headache, vomiting, seizure, coma
E. Evidence of inhalation burns: respiratory distress, cough, hoarseness, singed
nasal or facial hair, soot erythema of mouth, carbonaceous sputum
F. Entrance and exit wounds for electrical burns
G. Associated trauma
Treatment
A. THERMAL BURNS:
1. Remove clothing which is smoldering or which is non-adherent to the patient.
2. Administer oxygen if indications from history or physical of respiratory burns,
toxic inhalation, or significant flame or smoke exposure.
3. Assess and treat for associated trauma (blast or fall).
4. Consider cervical spine injury.
5. Remove rings, bracelets, and other constricting items.
6. If burn is moderate-to-severe (over 15% of body surface area), cover wounds
with dry clean dressings to avoid hypothermia. Preheat ambulance to
maximum temperature to prevent hypothermia during transport.
7. Use cool, wet dressings in smaller burns (less than 15%) for patient comfort.
8. Establish venous access in non-burned extremity when possible.
IV
IN
CB
9. Consider morphine sulfate 2-10 mg, IV bolus for pain relief.
10. If IV access is delayed consider Nebulized or IN (MAD device) Fentanyl
11. Transport, monitoring vital signs.
12. Observe for airway distress
IN
a. Be prepared to intubate.
NOTE:
Patients older than 12 years of age, with isolated second degree or third
degree burns greater than 20% body surface area, consider direct transport to the
University Hospital Emergency Department.
Go to Table of Contents
Patients 12 years of age and younger, with isolated second degree or third degree
burns greater than 20% body surface area, consider direct transport to the Children's
Hospital Emergency Department.
Patients in immediate need of airway management should be transported to the
nearest Emergency Department.
B. INHALATION INJURY:
1. Administer 100% oxygen during transport.
IN
2. Be prepared to intubate or assist if respirations inadequate.
3. Monitor cardiac rhythm.
C. CHEMICAL BURNS:
1. Protect rescuer from contamination. Wear appropriate gloves and clothing.
2. Remove all clothing and any solid chemical that might provide continuing
contamination.
3. Assess and treat for associated injuries.
4. Decontaminate patient using running water for 15 min. prior to transport if
patient stable.
5. Check eyes for exposure and rinse with free-flowing water for 15 min.
6. Evaluate for systemic symptoms that might be caused by chemical
contamination. CONTACT BASE for possible treatment.
7. Remove rings, bracelets, constricting bands.
8. Wrap burned area in clean, dry cloths for transport. Keep patient as warm as
possible after decontamination.
D. ELECTRICAL INJURY:
1. Protect rescuers from continued live electric wires.
2. Separate victim from electrical source when area safe for rescuers.
3. Initiate CPR as needed, monitor cardiac rhythm and treat arrhythmias per
protocols.
4. Prolonged respiratory support may be needed.
5. Immobilize cervical spine when appropriate, assess for other injuries.
IV
6. Establish venous access.
Specific Precautions
A. Leave blisters intact when possible.
B. Suspect airway burns in any facial burns or burns received in closed places.
Edema may become severe, but not be immediately apparent. Avoid
unnecessary trauma to the airway. Humidified oxygen is preferred if available.
C. Assume carbon monoxide poisoning in all closed space burns. Treatment is
100% oxygen continued for several hours. In addition, other toxic products of
combustion are more commonly encountered than realized.
D. CONTACT BASE for special instructions if other toxic inhalations are suspected.
Consider suicide attempt as cause of burn, and child abuse in pediatric burns.
E. Lightning injuries can cause ventricular asystole and prolonged respiratory arrest.
Prompt, continuous respiratory assistance (sometimes for hours to days) can
result in full recovery.
Return to Table of Contents
F. Field decontamination of chemical exposures has been shown to significantly
reduce extent of burn. Gross decontamination should occur prior to transport.
Notify hospital immediately to mobilize internal resources.
G. EMS personnel should not participate in decontamination unless trained and
equipped to do so.
H. In patients with severe burns, their ability to prevent heat loss is
significantly compromised. The time of transport may be enough to cause
hypothermia. Keep the ambulance as warm as possible during transport
despite discomfort to EMS personnel.
I. Isolated carbon monoxide poisoning should be taken to a hyperbaric oxygen
chamber. Multiple trauma patients with suspected carbon monoxide poisoning
should be taken to the appropriate trauma center.
Return to Table of Contents
5100
TASER PROTOCOL
I.
Purpose
To provide guidelines in handling patient who has been subjected to a Taser
General Principles
The Taser is a popular conducted electronic control weapon primarily used by law
enforcement as a less-than-lethal device
A Taser can be used as a contact device (touch-Taser) but is primarily used as a
distance weapon where it can fire probes up to 25 feet and engage an assailant
A controlled, pulsed electrical current is delivered that cause muscles in between the
probes to spasm uncontrollably
This is quite painful, and incapacitating
Special Considerations
1. Think safety—subjects who have been Tasered can still remain a threat
2. A thorough history and physical exam should be completed
3. All patients for whom a Taser has been utilized on shall be transported.
4. Patients with suspected stimulant use that have been tasered should have
continuous cardiac monitoring.
Procedure Taser Probe Removal
1. Taser probes imbedded anywhere above the clavicles, or in the nipple
or genitalia If found in this area, leave in place and transport
2. On most Taser probes there is a groove that runs along the side that
has the barb on it. Gently place counter pressure on each side of the
probe downward and perpendicular to the groove with one hand, then
firmly tug on the probe straight back.
3. Law enforcement may keep the probes as evidence. Otherwise treat
the probe as any other contaminated sharp and dispose of appropriately.
4. Document the contact appropriately
See Protocol: Excited Delirium
Go to Table of Contents
5200
Boulder Specific Trauma Activation Guidelines
Full Trauma Activation
1. GCS < 10 with trauma
2. Systolic BP < 90 and/or Pulse > 120
3. Respirations <10 or >29 or requiring intubation
4. Pediatric Criteria
a. Tachycardia with 2 or more signs of poor perfusion
b. BP lower limits for age (70 + 2 x age)
5. Flail chest
6. Multiple system traumatic blunt injury associated with suspected pelvic or long
bone fractures or altered mental status
7. Burns > 15% in adults and 10% in children AND associated trauma or
hemodynamically unstable or with inhalation injury
8. Suspected spinal injuries with neuro deficits
9. Amputation proximal to wrist or ankle
10. Penetrating trauma to Head, Neck, Chest, Abdomen, or Groin
11. Deterioration from Stable
12. Field Request for Activation
Limited Activation
1.
Hemodynamically stable patient without respiratory distress, but potential for
deterioration
2.
High energy transfer situations
a. Intrusion into passenger compartment > 12 inches
b. Auto vs. pedestrian, auto vs. bike, struck > 20 mph or thrown > 15 ft or
run over
c. MCC or ATV crash with separation of rider from vehicle
d. Death in same vehicle OR Ejection from vehicle
e. Unrestrained in rollover OR Extrication > 20 minutes
f. Blast injury OR Crush injury
g. Extrication > 20 minutes
3.
Stable electrical injury including lightning strikes
4.
Fall greater than 15 feet. Pediatric 2x height
5.
Pregnancy greater than 20 weeks, with mechanism
6.
Field Request for Activation
Special Considerations:
1. Extremes of age < 5 and > 55 y/o
2. Medical illness (COPD, CHF, renal failure, diabetes, HTN, etc.)
3. Presence of intoxicants
Special Notes:
1. The hospital shall be notified as soon as possible of a Trauma Activation.
2. A Trauma activation request will include: age, brief physiologic data and MOI.
3. Full Trauma Activation is based on physiological criteria while Limited Trauma
Activation is based on mechanism of injury.
4. A Full Trauma Activation will activate a surgeon who will evaluate the patient.
5. A Limited Trauma Activation will be met by the Emergency Physician who will then
evaluate the patient.
Return to Table of Contents
6000
GENERAL GUIDELINES FOR PEDIATRICS
Pediatric patients, for the purpose of the protocols, defined as age < 12 years, have
unique anatomy, physiology, and developmental needs that affect prehospital care as
well as hospital care. Because children make up a small percentage of total calls and
few pediatric calls are critically ill or injured, it is important to stay attuned to these
differences to provide good care. Therefore, CONTACT BASE early for guidance when
treating pediatric patients with significant complaints, including abnormalities of vital
signs. Pediatric emergencies are usually not preceded by chronic disease. If
recognition of compromise occurs early, and intervention is swift and effective, the child
will often be restored to full health.
The following should be kept in mind during the care of children in the prehospital
setting:
A. Airways are smaller, softer, and easier to obstruct or collapse.
B. Respiratory reserves are small. A minor insult like improper position, vomiting, or
airway narrowing can result in major deficits in ventilation and oxygenation.
C. Circulatory reserves are also small. The loss of as little as one unit of blood can
produce severe shock in an infant. Conversely, it is difficult to fluid overload
children. You can be confident that good hands-on circulation assessment will
accurately determine fluid needs.
D. Assessment of the pediatric patient can be accurately done using your
knowledge of the anatomy and physiology specific to infants and children.
E. Listen to the parents' assessment of the patient's problem. They often can detect
small changes in their child's condition. This is particularly true if the patient has
chronic disease.
F. The proper equipment is very important when dealing with the pediatric patient.
A complete selection of pediatric airway management equipment, IV catheters,
cervical collars, and drugs has been mandated by the state. This equipment
should be stored separately to minimize confusion.
G. When following these protocols, the age groups used are:
1. INFANTS:
birth to one year
2. TODDLERS:
one through five years
3. SCHOOL AGE: six through fourteen years
NORMAL VITAL SIGNS IN THE PEDIATRIC AGE GROUP
AGE
Newborn
6 mo
1 yr
3 yr
5 yr
8 yr
12 yr
PULSE
Average/minute
150
140
135
110
100
90
80
Return to Table of Contents
RESPIRATIONS
breaths/minute
40-60
25-40
20-30
20-30
20-30
12-25
12-25
BLOOD PRESSURE
systolic in mm Hg
60-80
65-105
70-110
76-116
80-120
86-126
95-120
6010
INFANT AND CHILD RESUSCITATION
Specific Information Needed
A. Time since the child was last in good health
B. History of any recent illness or injury
C. Past medical history
Specific physical findings
A. General appearance: LOC, muscle tone, color
B. Airway: obstruction, stridor, drooling, cough
C. Breathing: respiratory rate, skin color (cyanosis late sign), chest wall symmetry
and depth of movement, work of breathing (grunting, nasal flaring, retractions),
wheezing.
D. Circulation: heart rate, peripheral pulses, capillary filling time, skin color,
extremity skin temperature.
E. Level of consciousness, pupil size and reaction to light.
F. Physical assessment.
G. Respiratory distress is a critical situation that can be made worse with prolonged
scene times.
H. Any child with or suspected apnea episode should be transported.
Treatment
A. Airway/Breathing:
1. Manage airway. Effective airway management is by far the most critical
aspect of treatment. Bag-mask ventilation may be as good as and in some
cases superior to endotracheal intubation for EMS treatment.
2. Administer oxygen via blow-by, non-rebreather mask, or bag-mask
ventilation.
3. If apneic, ventilate with a BVM, intubate as indicated, ventilation rate per AHA
BLS protocols. Ensure adequate chest rise and fall (tidal volumes), and air
entry.
IN
4. Note the drugs that are appropriate for endotracheal administration
(naloxone, epinephrine, atropine). (mnemonic: N.E.A. – naloxone,
epinephrine, atropine). Endotracheal administration of any medication should
be considered LAST RESORT.
B. Circulation:
1. Initiate CPR if indicated.
IN
2. Monitor cardiac rhythm.
3. Establish peripheral venous access.
4. If unable to establish a peripheral IV after 1 attempt, establish an
intraosseous infusion. If unable to see good peripheral vein, go straight to IO
infusion.
5. If any signs of poor perfusion, infuse a 20 cc/kg of normal saline fluid bolus.
CONTACT BASE if you feel perfusion is compromised on reassessment.
C. Medications:
Go to Table of Contents
1. Stabilizing the airway and supporting respiration are the mainstays of
treatment. Specific treatment should be focused on the etiology of the arrest.
2. Arrhythmias are treated as noted in Arrhythmia Algorithms.
3. Hypoglycemia is common in younger children. If the child has altered mental
status, either administer dextrose (1-8 years should receive 2 ml/kg of a 25%
solution IV; <1 year should receive 5 ml/kg of 10% solution) or rule out
hypoglycemia with a bedside blood sugar check. Hypoglycemia in pediatrics
is commonly defined as a blood sugar <40.
Specific Precautions
A. The most successful pediatric resuscitations occur before a full cardiopulmonary
arrest. Assess pediatric patients carefully and assist with airway, breathing, and
circulatory problems before the arrest occurs, to improve the outcome in pediatric
patients.
B. Pediatric arrests are most likely to be primary respiratory events. The rescuer's
primary attention must be directed to securing the airway and providing good
ventilation before specific treatment of cardiac rhythm. Any cardiac rhythm can
spontaneously convert to sinus rhythm in a well-ventilated child.
C. Oxygen and epinephrine are the mainstays of pediatric resuscitations. Atropine
and sodium bicarbonate are not first line drugs in pediatrics.
D. Cardiopulmonary arrest from trauma is treated with airway management, rapid
transport, CPR and fluid administration en route.
E. Recommendations for obstructed airway are abdominal thrusts over the age of
one year. Infants less than one year old should be treated with back blows and
chest thrusts. Early laryngoscopy should be used in an attempt to visualize and
remove upper airway obstructions.
F. If a child 1 year of age or older is in cardiac arrest, an AED may be used,
preferably one with pediatric capabilities.
G. Use of a length-based emergency tape (LBET) such as the Broselow™ tape is
highly accurate and allows for rapid drug and fluid doses and correct equipment
size and use. LBET use should be routine for any pediatric emergency.
Return to Table of Contents
6020
POSSIBLE SUDDEN INFANT DEATH SYNDROME (SIDS)
Specific Information Needed
A. History: position in which the child was found, condition of the bed, last time the
child was seen well, seizure activity, trauma, possibility of ingestion
B. Associated symptoms: history of fever, respiratory symptoms, infection, vomiting,
diarrhea, other signs of infections
C. Past medical history: prematurity, chronic illness
Specific physical findings
A.
B.
C.
D.
E.
ABCs
Neurologic: level of consciousness, responsiveness, muscle activity and tone
Skin: signs of trauma
Dependent lividity or early rigor mortis.
Body temperature.
Treatment
A.
B.
C.
D.
IN
Initiate or continue resuscitation based on field pronouncement protocol.
Use appropriate airway adjuncts as indicated.
Ventilate with 100% oxygen; suction as needed.
Support cardiac output as indicated by:
1. CPR
2. External chest compressions
3. Establish venous access.
4. Pediatric ALS as indicated
5. Monitor cardiac rhythm
E. CONTACT BASE for field pronouncement if appropriate.
F. Support the parents and siblings.
Special Considerations
A. Activate appropriate support for the family if the patient is pronounced dead in
the field. Police, County Social Services, and the SIDS support line should be
contacted.
B. Automatic External Defibrillator (AED) should be used in patients >1 year old.
C. Avoid premature assessments.
D. The cause of SIDS is unknown. Cases occur between one month and one year
of age. All cases are mandatory coroner cases.
E. Consider possible NAT (non-accidental trauma, child abuse) and pass on any
concerns to receiving facility personnel.
F. For family support and community education, family members may welcome the
following contact information:
The Colorado SIDS Program, 6825 East Tennessee Ave., Suite 300, Denver, CO 80224
Local#: 303-320-7771 or toll-free#: 1-888-285-7437; Web: http://www.coloradosids.org
Go to Table of Contents
6030
PEDIATRIC DEHYDRATION
Specific Information Needed
A. History: onset and progression of symptoms, frequency of vomiting and
diarrhea, urine output, oral intake, recent trauma, possible drug ingestion
B. Past medical history
Document Specific physical findings
A. General appearance: LOC, muscle tone, color
B. ABCs and vital signs
C. Skin: warmth of distal extremities, color, skin turgor, capillary fill time (should be
less than 2 seconds), pulses
D. Mucous membranes: wetness of mouth, presence of tears
E. Musculoskeletal: evaluate for trauma
F. The signs of dehydration are:
1. EARLY - tachycardia and tachypnea for age, decreased LOC, capillary filling
time longer than two seconds, cool skin, mucous membranes dry, sunken
eyes and fontanelle;
2. LATE - loss of skin turgor, diminished pulses, and shock
Treatment
A.
B.
C.
D.
IV
Use appropriate airway adjuncts as indicated.
Administer oxygen
Breathing: ventilation as indicated
Circulation:
1. Establish pulse rate and capillary refill time
2.
3.
4.
5.
Establish peripheral venous access.
Consider fluid bolus of normal saline 20cc/kg.
Do not delay transport for IV attempts.
The patient with simple dehydration is not a candidate for intraosseous
infusion, CONTACT BASE for approval of IO if shock is present.
Specific Precautions
A. Assessment of dehydration is primarily by physical exam. Vital signs may be
abnormal, but they are nonspecific.
B. Determination of tachycardia or hypotension is based on age.
C. Monitor carefully for signs of decreased tissue perfusion (shock). Early
(compensated) shock is present if capillary fill time is greater than 2 seconds,
and there are poor pulses, muscle tone and color, and/or are normotensive.
Decompensated shock is present if systolic BP is <normal for age, have a
decreased mental status and/or have weak or absent central pulses.
Go to Table of Contents
6040
PEDIATRIC RESPIRATORY DISTRESS
Specific Information Needed
A. History: sudden or gradual onset of symptoms, cough, fever, sore throat,
hoarseness
B. History of potential foreign body aspiration or trauma
C. Past medical history
D. Current medication use
Specific Objective Findings
A. Airway: look for respiratory distress during inspiration, listen for abnormal
breathing sounds such as stridor, cough (croup-like?), and wheezing, feel for air
movement, crepitation, and tracheal deviation (late finding).
B. Breathing: respiratory rate and effort, chest wall movement/adequacy of tidal
volume, color, use of accessory muscles, retractions, nasal flaring, head
bobbing, or grunting
C. Respiratory sounds by auscultation of chest: wheezing, rales, decreased
(unilateral?), prolonged inspiratory (croup) or expiratory (wheezing) phases.
D. Mental status: AVPU
E. General appearance: leaning forward or drooling (suggests upper airway
obstruction), skin color and temperature, muscle tone.
Treatment
A. Administer high-flow oxygen by blow-by or non-rebreather mask.
B. As long as the child is adequately ventilating and has adequate mentation, avoid
agitating the patient. Keep the patient in his position of comfort.
C. If the child is not ventilating adequately, assist with a BVM.
D. If the patient is wheezing and has a metered dose inhaler (MDI), initiate MDI
protocol. EMT’s must contact base.
E. In the rare case that the child cannot be ventilated with a BVM device:
1. Reposition airway. Consider oral airway if patient unconscious.
2. If still unable to ventilate, visualize the airway with a laryngoscope. Remove
any foreign object with Magill forceps.
3. If nothing is seen, orally intubate the patient.
F. Consider intubation only if unable to provide ventilatory support with a BVM and
oral airway.
G. Assess and consider treatment for the following problems if respiratory distress is
severe and the patient does not respond to proper positioning and administration
of high flow oxygen.
IN
IN
CB
1. Croup or Epiglottitis:
a. Allow patient to remain in position of comfort if alert.
b. Consider administering nebulized racemic epinephrine 0.5 ml or Lepinephrine, 5 mg (5.0 ml of a 1:1000 solution) (under 10 kg use 0.5
ml/kg of a 1:1000 solution) via nebulizer if croup is likely and there is
respiratory distress.
2. Asthma:
Go to Table of Contents
a. Administer albuterol sulfate, one unit dose bottle by nebulizer. Consider
adding Ipratropium (0.5 mg/2.5ml) for patients over 2 years of age.
b. Use continuous nebulization of Albuterol sulfate for respiratory distress.
c. Consider Epinephrine 0.01 mg/kg (0.01 ml/kg of a 1:1000 solution),
SQ/IM.
H. If diagnosis is unclear, transport patient with 100% oxygen, reassess frequently
and be prepared to manage the patient's airway.
Specific Precautions
A. Children with croup, epiglottitis, or laryngeal edema usually have respiratory
arrest due to exhaustion. Most children can still be ventilated with a BVM.
B. Children with severe asthma may not exhibit wheezing. The patients will have
prolonged expiratory phases and may appear listless, agitated, or unresponsive.
C. Respiratory distress is a critical situation that can be made worse with prolonged
scene times.
D. Cyanosis is a late sign in pediatric hypoxia. Provide 100% oxygen for any child in
distress.
E. Consider the differential assessment for each finding:
1. Stridor: foreign body, croup, epiglottitis or other bacterial upper airway
infection, larynx trauma, etc
2. Wheezing: foreign body, asthma, bronchiolitis, hydrocarbon exposure, etc
3. Respiratory distress: pneumothorax, foreign body, pneumonia, shock, CHF,
etc
IN
F. Any child with a witnessed or suspected apnea episode should be transported.
G. Intubation of the infant is most easily accomplished with an infant-sized straight
laryngoscope blade.
H. Do not intubate unless you can visualize the ETT going through the cords. If you
are unable to intubate the trachea quickly, withdraw, re-oxygenate with BVM, and
try again. No harm will result to the child if you keep the patient well oxygenated
and don't traumatize the airway with intubation attempts. Transporting while
using BVM only is acceptable and may be preferable in many circumstances.
Return to Table of Contents
6050
PEDIATRIC SEIZURES
Specific Information Needed
A. History: preceding activity level, onset and duration of seizure, description of
seizure activity, fever, color change, recent illness, head trauma, possibility of
ingestion, cardiac symptoms.
B. Past history: previous seizures, current medications, chronic illness
Specific Objective Findings
A. Airway: look for respiratory distress, listen for abnormal breathing sounds, feel for
air movement, crepitus.
B. Breathing: respiratory rate and effort, chest wall movement (adequacy of tidal
volume), use of accessory muscles, retractions.
C. Circulation: heart rate, pulse, capillary filling time, skin color, blood pressure
D. Neurologic: mental status, muscle tone, focal findings, post-ictal period,
incontinence. Note improvement or deterioration in mental status with time.
E. Musculoskeletal: note any associated injuries.
Treatment
A. Airway: Maintain patent airway by BLS maneuvers. Suction as needed.
Administer high concentration oxygen.
B. Breathing: Assist ventilation as needed. (rarely necessary)
C. If child is in status epilepticus:
IN
P
IV
IN
CB
1. Attempt peripheral venous access x1. If successful, administer diazepam 0.3
mg/kg, IV/IO bolus, slowly, over 2 minutes OR 0.5 mg/kg rectally up to a
maximum of 10 mg OR administer diazepam, 0.5 mg/kg rectally, not to
exceed 10 mg.
2. If unable to start peripheral IV:
a. for ages 8 and under, administer diazepam, 0.5 mg/kg rectally, not to
exceed 10 mg.
b. for ages 9 and above, administer midazolam 0.1 mg/kg IM, not to exceed
10 mg.
2. Determine blood glucose level and draw appropriate blood tubes if possible.
3. If hypoglycemic, give dextrose (1-8 years should receive 2 ml/kg of a 25%
solution IV; <1 year should receive 5 ml/kg of 10% solution).
4. If seizures continue, CONTACT BASE.
D. If the child has stopped seizing and is postictal, transport while continuing to
monitor vital signs and neurological condition. Continue to provide supplemental
oxygen.
E. If child is febrile initiate passive cooling measures.
Go to Table of Contents
Specific Precautions
A. Febrile seizures occur in normal children between 6 months and 6 years. Such
seizures are usually short, lasting less than 5 minutes, generalized, and usually
do not require anti-seizure drug therapy.
B. Do not force anything between the teeth.
C. Consider hypoglycemia as a cause for non-traumatic seizure.
D. Breath-holding spells in toddlers can resemble seizures, but are not a true
seizure.
E. Most airways of seizing children can be managed with BLS measures. Intubation
is only necessary if there is prolonged apnea from diazepam or from the seizure
activity itself.
Return to Table of Contents
7010
STANDARD DRUG ADMINISTRATION PROTOCOL
A. The following protocol should be followed with the administration of any prehospital medication.
1. Perform initial patient assessment.
2. Administer supplemental oxygen.
3. Obtain vital signs.
4. Assess the need for medication.
5. Ensure medication to be delivered is prescribed to the patient.
6. Contact on-line medical control for an order to administer medication.
7. Administer the medication.
8. Reassess the vital signs and patient condition after 1-2 minutes.
9. If the patient’s condition persists or worsens, re-contact the base station for
additional guidance.
10. Complete your patient care record with full documentation of the patient’s
symptoms, the patient assessment, the patient vital signs, the time and the
amount of the drug given, and the effect the medication had on the patient’s
condition.
B. The above steps should be performed while initiating patient transportation. The
administration of field medication should not delay patient transportation.
C. ALL PATIENTS RECEIVING PATIENT ASSISTED DRUG ADMINISTRATION
SHOULD BE TRANSPORTED TO THE HOSPITAL.
Go to Table of Contents
7020
MEDICATION ADMINISTRATION (PARENTERAL)
Indications
A. Illness or injury which requires medication to improve or maintain the patient's
condition
Precautions
A. Use BSI.
B. Certain medications can be administered via one route only, others via several.
If you are uncertain about the drug you are giving - check with base.
C. Make certain that the medication you want to give is the one in your hand.
Always double check medication and dose before administration.
D. IM and SQ routes are unpredictable: medications are absorbed erratically via
these routes and may not be absorbed at all if the patient is seriously ill and
severely vasoconstricted. The IV route should be used almost exclusively in the
field. If an IV cannot be started, the endotracheal route is the best alternative.
Technique
A. Use syringe just large enough to hold appropriate quantity of medication (or use
prefilled syringe).
B. Attach large gauge needle to syringe.
C. Break ampule (use filtered needle, when available) or cleanse multi-dose vial
with alcohol (the latter is less desirable for field use).
D. Using sterile technique, draw medication into syringe.
E. Change needles to small gauge for IM or SQ.
Endotracheal Technique (LAST RESORT)
A. Prepare medication to be given, and set next to patient being ventilated.
B. Ventilate fully and rapidly 4-5 times prior to disconnecting the bag from the
endotracheal tube.
C. Check medication in hand. Confirm medication, dose, amount, and expiration
date.
D. Higher doses are required when administering drugs endotracheally
E. Dilute medication with 10 ml of normal saline, unless using prefilled syringes.
F. Administer medication.
G. Connect the bag and ventilate rapidly an additional 4-5 times.
H. Disconnect the bag and administer the remaining half of medication into the
endotracheal tube.
I. Again connect the self-inflating bag and ventilate rapidly 4-5 times before
resuming the recommended ventilation rate according to the age and condition of
patient.
J. Record medication given, dose, amount, and time.
Intraosseous Technique
A. Prepare medication to be administered.
B. Check medication in hand. Confirm medication, dose, amount, and expiration
date.
C. Wipe port site with alcohol.
D. Inject into port on intraosseous line, or
E. Remove needle from syringe and inject directly into intraosseous needle.
Go to Table of Contents
F. Record medication given, dose, amount, and time.
Intramuscular Technique (for ages 8 or greater only)
A. Prepare medication to be administered.
B. Check medication in hand. Confirm medication, dose, amount, and expiration
date.
C. Prep area of skin with alcohol or Betadine wipe.
D. Inject 22 g/1½" needle into desired muscular site (deltoid, gluteus, or vastus
lateralis) at 90˚ angle. Aspirate to ensure needle is not in blood vessel.
E. Inject medication slowly into muscular site.
F. Withdraw needle and observe for any bleeding or swelling. Apply sterile dressing
to injection site.
G. Record medication given, dose, amount, and time.
Intravenous Push (IVP) Technique
A. Use needle appropriate for viscosity of fluid injected.
B. Wipe IV tubing injection site with alcohol.
C. Check medication in hand. Confirm medication, dose, amount, and expiration
date.
D. Eject air from syringe.
E. Insert needle into injection site.
F. Pinch IV tubing closed between bag and needle.
G. Inject at a rate appropriate for medication.
H. Withdraw needle and release tubing to restore flow.
I. Record medication given, dose, amount, and time.
J. Give 20 cc saline fluid flush after giving any drugs.
Nebulization Technique
A. Use hand-held nebulizer with mouthpiece (or mask for patient unable to hold
mouthpiece).
B. Check medication in hand. Confirm medication, dose, amount, and expiration
date.
C. Draw up dose of medication in syringe or dropper; inject into nebulizer.
D. Attach to oxygen tubing and set at 6-8 L/min (sufficient to produce good
vaporization).
E. Administer for approximately 5 minutes, until solution is gone from chamber.
F. Record medication given, dose, amount, and time.
Rectal Technique
A. Technique One
1. Use a tuberculin syringe (without needle) lubricated with a water-soluble,
lubricating jelly.
2. Check medication in hand. Confirm medication, dose, and expiration date.
3. Insert needleless syringe into rectum completely to end of syringe (4-5cm).
4. Inject the medication and withdraw the syringe. No flushing is necessary.
B. Technique Two
1. Lubricate with a water-soluble lubricating jelly and insert a feeding tube 4-5
cm into the rectum.
2. Attach a syringe containing the appropriate dose of the medication to be
given and instill.
Return to Table of Contents
3. Remove the syringe from the tube, draw up 1 cc of air, reattach the syringe to
the tube, and instill the air to clear the tube of medication. Then withdraw the
feeding tube from the rectum.
Subcutaneous Injection Technique
A. Use 25 g needle, 5/8" length for most subcutaneous injections.
B. Check medication in hand. Confirm medication, dose, amount, and expiration
date.
C. Select injection site (usually jrm misctr todeltoid)(. )]TJEMC /P <</MCID119 >>BDC 0.001 Tc -0.0001
time. This may include the dilution of a medication to facilitate a slow
administration.
Return to Table of Contents
ADENOSINE (ADENOCARD)
Description
Adenosine is primarily formed from the breakdown product of adenosine triphosphate
(ATP). Both compounds are found in every cell of the human body and have a wide
range of metabolic roles. Adenosine slows tachycardias associated with the AV node via
modulation of the autonomic nervous system without causing negative inotropic effects.
It acts directly on sinus pacemaker cells and vagal nerve terminals to decrease
chronotropic and dromotropic activity. Adenosine is the drug of choice for paroxysmal
supraventricular tachycardia (PSVT).
Onset & Duration
Onset: almost immediate
Duration: 10 sec
Indications
Conversion of PSVT to sinus rhythm
Contraindications
Second- or third-degree AV block
Sick sinus syndrome
Hypersensitivity to adenosine
Adverse Reactions
Facial flushing
Lightheadedness
Paresthesia
Headache
Diaphoresis
Palpitations
Chest pain
Hypotension
Nausea
Metallic taste
Shortness of breath
Drug Interactions
Methylxanthines (for example, caffeine and theophylline) antagonize the action of
adenosine. Dipyridamole potentiates the effect of adenosine; reduction of adenosine
dose may be required. Carbamazepine may potentiate the AV-nodal blocking effect of
adenosine.
Dosage and Administration
Adult:
6.0 mg IV bolus, rapidly, followed by a Normal Saline flush.
Observe EKG monitor for 1-2 minutes for evidence of cardioversion.
If there is no evidence of cardioversion, administer Adenosine 12 mg, IV bolus,
rapidly, followed by a Normal Saline flush.
Observe EKG monitor for 1-2 minutes for evidence of cardioversion.
Contact medical control for further considerations
NOTE: Total maximum dose should not exceed 18 mg.
Go to Table of Contents
Pediatric:
0.1 mg/kg, IV or IO bolus, rapidly, followed by Normal Saline flush.
If SVT persists, a second dose may be given using 0.2 mg/kg IV or IO bolus,
followed by Normal Saline flush
If this fails to convert the dysrhythmia, Adenosine may be repeated at 0.2 mg/kg, IV
or IO bolus, rapidly, followed by Normal Saline flush.
Protocol
Narrow Complex Tachycardia
Special Considerations
May produce bronchoconstriction in patients with asthma or bronchopulmonary disease.
At the time of conversion asystole or new rhythms may result. These generally last a few
seconds without intervention
Adenosine is not effective in atrial flutter or fibrillation
Adenosine is safe in patients with a history of Wolff-Parkinson-White syndrome.
Concomitant use of dipyridamole (Persantine) enhances the effects of adenosine.
Smaller doses may be required.
Caffeine and theophylline antagonize adenosine's effects. Larger doses may be
required.
A 12-lead EKG should be performed and documented, when available.
Return to Table of Contents
ALBUTEROL SULFATE (PROVENTIL, VENTOLIN)
Description
Albuterol is a sympathomimetic that is selective for beta-2 adrenergic receptors. It
relaxes smooth muscles of the bronchial tree and peripheral vasculature by stimulating
adrenergic receptors of the sympathetic nervous system.
Onset & Duration
Onset: 5-15 min. after inhalation
Duration: 3-4 hr after inhalation
Indications
Relief of bronchospasm in patients with reversible obstructive airway disease
Prevention of exercise-induced bronchospasm
Contraindications
Prior hypersensitivity reaction to albuterol
Cardiac dysrhythmias associated with tachycardia
Tachycardia caused by digitalis intoxication
Adverse Reactions
Tachycardia
Restlessness
Anxiety
Headache
Dizziness
Nausea
Palpitations
Hypertension
Dysrhythmias
Drug Interactions
Sympathomimetics may exacerbate adverse cardiovascular effects. Antidepressants
may potentiate the effects on the vasculature. Beta blockers may antagonize albuterol.
Albuterol may potentiate diuretic-induced hypokalemia.
How Supplied
MDI: 90 mcg/metered spray (17-g canister with 200 inhalations)
Prediluted nebulized solution: 2.5 mg in 3 ml NS (0.083%)
Dosage and Administration
Bronchial asthma
Adult:
Albuterol sulfate solution 0.083% 2.5mg (one unit dose bottle of 3.0 ml), by nebulizer,
at a flow rate (6-8 lpm) that will deliver the solution over 5 to 15 minutes.
Pediatric:
Albuterol sulfate 0.083% 2.5mg (one unit dose bottle of 3.0 ml), by nebulizer, at a
flow rate (6-8 lpm) that will deliver the solution over 5-15 minutes.
Protocol
Asthma
Go to Table of Contents
Chronic Obstructive Pulmonary Disease
Pneumonia
Pediatric Respiratory Distress
Special Considerations
May precipitate angina pectoris and dysrhythmias
Should be used with caution in patients with diabetes mellitus, hyperthyroidism, prostatic
hypertrophy, or seizure disorder
Return to Table of Contents
AMIODARONE (CORDARONE)
Description
Amiodarone has multiple effects showing Class I, II, III and IV actions with a quick onset.
The dominant effect is prolongation of the action potential duration and the refractory
period.
Indications
Ventricular Fibrillation
Ventricular Tachycardia without a pulse
Wide complex tachycardia refractory to cardioversion
Precautions
Wide complex irregular tachycardia
Sympathomimetic toxidromes, i.e. cocaine or amphetamine overdose
NOT to be used to treat ventricular escape beats or accelerated idioventricular rhythms
Contraindications
Wolff-Parkinson-White Syndrome (relative contraindication)
Pulmonary congestion
Cardiogenic shock
Adverse Reactions
Severe hypotension
Profound bradycardia
Dosage and Administration
Adult:
Cardiac Arrest
300 mg IV bolus. Repeat once 150 mg IV bolus in 3-5 minutes. CONTACT BASE
for additional doses.
After successful defibrillation, 150 mg IV bolus infusion over 10 minutes
Wide Complex tachycardia
150 mg IV bolus infusion over 10 minutes.
Pediatric:
Cardiac Arrest
5mg/kg IV over 3-5 minutes. CONTACT BASE for additional doses.
Protocol
Ventricular Fibrillation/Ventricular Tachycardia without a pulse
Wide complex tachycardia refractory to cardioversion
Special Considerations
A 12-lead EKG should be performed and documented, when available.
Go to Table of Contents
ASPIRIN (ASA)
Description
In low doses, aspirin inhibits blood clotting, specifically the formation of thromboxane A2,
a platelet aggregating, vasoconstricting prostaglandin.
Platelet aggregation has been implicated in the pathogenesis of atherosclerosis
contributing to the acute episodes of transient ischemic attacks, unstable angina, and
acute myocardial infarction. This has been linked to anginal episodes. Unstable angina
is precipitated by a sudden fall in coronary blood flow.
Aspirin has been shown to be beneficial in decreasing sudden cardiac death and
myocardial infarction in patients with unstable angina. It has also been shown to be of
added benefit in maintaining vessel patency after thrombolytic therapy
Indications
Patients with chest pain that may be related to cardiac origin.
Contraindications
Patients with an active gastrointestinal bleed
Patients with an allergy to aspirin
Adverse Reactions
Wheezing, Tinnitus, GI Upset, GI bleeding
How Supplied
Chewable tablets 81mg
Dosage and Administration
Aspirin should be given to conscious patients who can voluntary chew and swallow.
Dose is four (4) 81 mg tablets for a total of 324mg.
Protocol
Premature Ventricular Contractions (PVCs)
Chest Pain
Special Considerations
Aspirin should not be given for analgesia, i.e. head or body aches.
Patients on coumadin may be given aspirin
Go to Table of Contents
ATROPINE SULFATE
Description
Atropine is a parasympathetic or cholinergic blocking agent. As such, it has the following
effects:
• Increases heart rate (by blocking vagal influences)
• Increases conduction through A V node
• Reduces motility and tone of GI tract
• Reduces action and tone of urinary bladder (may cause urinary retention)
• Dilates pupils
Note: This drug blocks cholinergic (vagal) influences already present. If there is little
cholinergic stimulation present, effects will be minimal.
Indications
Asystole and idoventricular cardiac arrests
Hemodynamically unstable bradycardias
To improve conduction in 2nd and 3rd degree heart block or in pacemaker failure
Organophosphate poisoning
Precautions
Should not be used without medical control direction for stable bradycardias
Closed angle glaucoma
Adverse Reactions
Headache
Dry mouth
Nausea
Dizziness
Tachycardia
Palpitations
Dosage and Administration
Cardiac Arrest
Adult:
1.0 mg IV/IO rapid bolus. Repeat every 3-5 minutes, not to exceed 3.0 mg.
Pediatric:
Refer to Length Based Measurement tool.
Hemodynamically Unstable Bradycardia
Adult:
0.5 – 1.0 mg IV/IO rapid bolus. Repeat if needed at 3-5 minute intervals to a dose of
3 mg. (Stop at ventricular rate which provides adequate mentation and B/P.)
Pediatric:
0.02 mg/kg, IV/IO bolus. Minimum dose is 0.1 mg.
Acute Organophosphate Exposure
Adult:
2mg IV/IO every 5 min. until secretions dry
Pediatric:
0.05 to 0.2mg/kg every 5 min. until secretions dry
Protocol
Go to Table of Contents
Asystole
Bradycardia with a pulse
Poisoning/Overdose
Infant and Child Resuscitation
Special Considerations
• Atropine causes pupil dilation, even in cardiac arrest settings.
• Endotracheal administration should be used only as a last resort.
• If given ET, dosing is x2 normal dosing with a max ET dose of 6mg.
Return to Table of Contents
Diltiazem (Cardizem)
Description
Diltiazem is an Antiarrhythmic / Calcium Channel Blocker. As such it has the following
effects:
• Slows conduction through the AV node.
• Vasodilation
• Decreases rate of ventricular response
• Decreases myocardial oxygen demand
Indications
To control rapid ventricular rates (>150 bpm) associated with atrial fibrillation and atrial
flutter.
Rapid narrow complex PSVT, unresponsive to adenosine.
Contraindications
Known hypersensitivity to diltiazem
Hypotension
Pulmonary congestion
Wide-complex tachycardia
Conduction disturbances: WPW, sick sinus syndrome, AV block
Precautions
Concurrent use with Midazolam may require decreased dose
Use with caution in patients on oral / IV beta-blockers
Adverse Reactions
Nausea and vomiting, hypotension, and dizziness
Dosage and Administration
1. Initial dose: Bolus 0.25 mg / kg (typically 20 mg) IV over 2 minutes
2. Second dose in 15 minutes if inadequate response to initial dose:
3. Bolus 0.35 mg / kg (typically 25 mg) IV over 2 minutes
4. All dosing in the physiologically elderly pt. should be reduced 50%.
Protocol
Narrow complex tachycardia
Special Considerations
• Patients with rapid atrial fibrillation who are unstable (BP < 80 and altered mental
status or signs of ischemia) should be cardioverted. If cardioversion is
unsuccessful then diltiazem can be considered.
• Patients with chronic atrial fibrillation run the risk of embolization with sudden
cessation of the rhythm by cardioversion. Therefore, in the semi-unstable patient
with chronic atrial fibrillation and now with a rapid ventricular response, slowing of
the rate with diltiazem is preferred so that cardioversion can be done after the
patient is anticoagulated.
Go to Table of Contents
•
•
The use of calcium channel blockers in patients with rapid atrial fibrillation
secondary to accessory conduction pathways (WPW) can potentially accelerate
conduction through the accessory pathway causing a fatal dysrhythmia. This
effect is primary found with verapamil and not diltiazem.
Stable patients with rapid atrial fibrillation and short transport times should be
transported to the ED, where calcium channel blocker therapy can be initiated.
Return to Table of Contents
DEXTROSE 50%
Description
Glucose is the body's basic fuel and is required for cellular metabolism. A sudden drop
in blood sugar level will result in disturbances of normal metabolism, manifested
clinically as a decrease in mental status, sweating and tachycardia. Further decreases
in blood sugar may result in coma, seizures, and cardiac arrhythmias. Serum glucose is
regulated by insulin, which stimulates storage of excess glucose from the blood stream,
and glucagon, which mobilizes stored glucose into the blood stream.
Indications
• Hypoglycemic states (i.e., insulin shock in the diabetic)
• The unconscious patient with an unknown history. Any patient with focal or
partial neurologic deficit or altered state of consciousness, which may be due to
hypoglycemia
• Non-traumatic seizure patients who show no improvement in post-ictal state
• Patients in status epilepticus not responsive to Valium
• Blood glucose test < 60 if clinically indicated
• Poisons and Overdoses protocol
• In children with alcohol exposure, suspected sepsis, hypoperfusion or altered
mental status
Precautions
Patients presenting with signs of CVA, unless presenting with a significantly low blood
glucose.
Dextrose can exacerbate Wernicke’s encephalopathy and Korsakoff’’s Psychosis found
primarily in the chronic ETOH abuse patient.
Dosage and Administration
Adult:
25 gm (50 ml of a 50% solution), IV bolus or Rectal.
Pediatric:
1-8 years: 2-4 ml/kg of a 25% solution IV or Rectal.
<1 year: 2-4 ml/kg of a 10% solution IV or Rectal.
NOTE: Oral glucose can be used for conscious patients able to swallow.
Protocol
Altered Mental Status
Seizures
Syncope
Poisoning/Overdose
Psychiatric/Behavioral
Infant and Child Resuscitation
Pediatric Seizures
Special Considerations
Draw blood sample before administration if possible.
Return to Table of Contents
Use glucometer before administration.
Extravasation may cause tissue necrosis; use a large vein and aspirate occasionally to
ensure route patency.
Dextrose should be diluted 1:1 with normal saline (to create D25W) for patient 8 years
and younger
Return to Table of Contents
DIAZEPAM (VALIUM)
Description
Diazepam acts as a tranquilizer, anticonvulsant, and skeletal muscle relaxant through
effects on the central nervous system
Indications
Status epilepticus
Drug-induced hyperadrenergic states manifested by tachycardia and hypertension (i.e.,
cocaine, amphetamine overdose)
Combative patients from head injury or from suspected stimulant abuse (i.e.: cocaine,
PCP, ecstasy, amphetamines)
Severe musculoskeletal back spasms
Precautions
Patients under the influence of alcohol
Adverse Reactions
Drowsiness
Dizziness
Respiratory depression
Fatigue
Ataxia
Paradoxical excitement or stimulation may occur
Dosage and Administration
A. Adult
1. Status Seizures
a. Initial dose: 1-10 mg IV or IM
b. Repeat dose: 1-10 mg IV or IM
2. Hyperadrenergic States/ Severe Musculoskeletal Spasm/
Combative Patients/Sedation
a. Initial dose 1-10 mg IV or IM
b. Repeat dose 1-5 mg IV or IM
3. Combination Analgesia
a. 1-5 mg IV over 2 minutes for spasm and/or anxiety.
b. Repeat Dose 1-2 mg IV over 2 minutes.
B. PEDIATRIC DOSAGES
Status Seizures
a. Initial dose 0.2 mg/kg IV/IM OR 0.50 mg/kg rectal
b. Repeat dose 0.2 mg/kg IV/IM OR 0.50 mg/kg rectal
Protocol
Seizures
Combination Analgesia
Poisoning/Overdose
Hyperthermia
Psychiatric/Behavioral
Pediatric Seizures
Go to Table of Contents
Head trauma
Special Considerations
Since diazepam can cause respiratory depression and/or hypotension, the patient
should be monitored closely (vitals signs, cardiac monitor, pulse oximeter). Very rarely,
cardiac arrest can occur.
Patients receiving diazepam should be placed on oxygen.
Do not give unless the patient is actively seizing.
Diazepam should be used with caution in any patient under the influence of alcohol.
Return to Table of Contents
DIPHENHYDRAMINE (BENADRYL)
Description
Diphenhydramine blocks action of histamine released from cells during an allergic
reaction. Direct CNS effects, which may be stimulant or, more commonly, depressant,
depending on individual variation. Also has anticholinergic, antiparkinsonian effects,
which is used to treat acute dystonic reactions to antipsychotic drugs (Haldol, Thorazine,
Compazine, etc.) These reactions include oculogyric crisis, acute torticollis, and facial
grimacing.
Indications
Moderate allergic reactions
Second line for anaphylaxis and severe allergic reactions
Control extrapyramidal effects
Synergist to other medications in Combative Patient
Precautions
Lower respiratory diseases such as asthma or COPD
Narrow-angle glaucoma
Bladder obstruction
Side effects
Dose-related drowsiness
Dilated pupils
Dry mouth and throat
Flushing
May potentiate with alcohol usage
Drug Interactions
CNS depressants and alcohol may have additive effects.
MAO inhibitors may prolong and intensify anticholinergic effects of antihistamines.
Dosage and Administration
Adults: 25-50 mg, IV bolus, or IM if vascular access has not been obtained
<8 years: 1-2 mg/kg slow IV bolus/IM (not to exceed 50 mg)
Protocol
Restraint
Allergic Reaction
Go to Table of Contents
DOPAMINE (INTROPIN)
Description
Dopamine is chemically related to epinephrine and norepinephrine. It acts primarily on
alpha-1 and beta-1 adrenergic receptors, increasing systemic vascular resistance and
exerting a positive inotropic effect on the heart. In addition, the actions of this drug on
dopaminergic receptors dilate renal and splanchnic vasculature, maintaining blood flow.
Dopamine is commonly used to treat hypotension associated with cardiogenic shock.
Indications
Symptomatic hypotension from causes other than hypovolemia
Contraindications
Patients with hypovolemia
Cardiogenic Shock secondary to Arrhythmia prior to treatment of the arrhythmia
Adverse Reactions
Dose-related tachydysrhythmias
Hypertension
Increased myocardial oxygen demand
Dosage and Administration
Mix: 400 mg in 250 ml NS or 800 mg in 500 ml NS to produce concentration of
1600 mcg/ml.
Actions of dopamine are dose dependent:
1. <5 mcg/kg/min Dilates renal/mesenteric vessels with no effect on
heart rate or blood pressure
2. 5-10 mcg/kg/min Mild effect on cardiac output and peripheral
vasoconstriction leading to slight increase in blood pressure
3. 10-20 mcg/kg/min Increased heart rate, cardiac output, and peripheral
vasoconstriction leading to increased blood pressure
4. >20 mcg/kg/min Diffuse vasoconstriction leading to increased blood
pressure, however, major decrease in renal and mesenteric blood
flow
Adults: 5-20 mcg/kg/min
Pediatrics:
5-20 mcg/kg/min CONTACT BASE EXCEPT IN CASES OF CARDIAC
ARREST
Protocol
Shock: Medical
Special Considerations
• Dopamine is better administered using an infusion pump to ensure accurate
dosing
• May become ineffective is added to solutions containing alkaloids
• At low doses, decreased blood pressure may occur due to peripheral
vasodilatation. Increasing infusion rate will correct this.
Go to Table of Contents
•
•
•
Tissue extravasation at the IV site can cause skin sloughing due to
vasoconstriction. Be sure to make Emergency Department personnel aware if
there has been any extravasation of dopamine-containing solutions, so that
proper treatment can be instituted.
Can cause hypertensive crisis in susceptible individuals
Certain antidepressants potentiate the effects of this drug.
INTRAVENOUS DRIP RATES FOR DOPAMINE
Concentration: 1600 mcg/ml
Dose
(mcg/kg/min)
Weight
5
10
15
20
50
10
20
30
40
60
10
25
35
45
70
15
25
40
50
80
15
30
45
60
90
15
35
50
70
100
20
35
55
75
110
20
40
60
85
microdrips/min
Return to Table of Contents
EPINEPHRINE (ADRENALIN)
Description
Epinephrine stimulates alpha, beta-1, and beta-2 adrenergic receptors in dose-related
fashion.
Indications
Bronchial asthma
Acute allergic reaction
Bradycardia
Cardiac arrest
Airway obstruction secondary to croup or epiglottitis
Adverse Reactions
Headache
Nausea
Vomiting
Anxiety
Tremors
Palpitations
May precipitate angina
Drug Interactions
May be deactivated by alkaline solutions (sodium bicarbonate, furosemide).
Dosage and Administration
Adult:
Cardiac Arrest
1.0 mg (10 ml of a 1:10,000 solution), IV/IO bolus. Repeat every 3-5 minutes.
Bradycardia refractory to other interventions:
1.0 mg in 250 ml of Normal Saline. Infuse at 2 mcg/min until desired BP of 90 mmHg
systolic.
Asthma:
0.3 mg (0.3 ml of a 1:1,000 solution), SQ/IM.
Moderate to Severe Allergic Reaction:
0.3 mg (0.3 ml of a 1:1,000 solution), SQ/IM.
Anaphylactic Reaction:
0.1 mg (1 ml of a 1:10,000 solution), IV followed by 1.0 mg in 250 ml of Normal
Saline infused at 2 mcg/min until desired BP of 90 mmHg systolic
Pediatric:
Cardiac arrest:
First dose: 0.01 mg/kg IV/IO/ET (0.1 ml/kg of 1:10,000 solution)
Subsequent doses: 0.01 mg/kg, IV/IO/ET (0.1 ml/kg of 1:10,000 solution)
Bradycardia
0.01 mg/kg (0.1 ml/kg of 1:10,000 solution) IV/IO
Moderate to Severe Allergic Reactions
0.01 mg/kg (0.01 ml/kg of 1:1,000 solution) IM/SQ
Anaphylaxis
0.01 mg/kg (0.1 ml/kg of 1:10,000 solution) IV/IO
Asthma
0.01 mg/kg (0.01 ml/kg of 1:1,000 solution) IM/SQ
Go to Table of Contents
Life threatening airway obstruction suspected secondary to croup or epiglottitis
In the absence of racemic epinephrine, plain L-epinephrine can be used. The dose is
5 mg (5.0 ml of 1:1000 solution of L-epinephrine, undiluted, nebulized). In smaller
infants, weighing <10 kg, the recommended dose is 0.5 ml/kg of 1:1000 Lepinephrine.
Protocol
Asystole
Bradycardia with a pulse
Asthma
Allergy/Anaphylaxis
Infant and Child Resuscitation
Pediatric Respiratory Distress
Pediatric Anaphylactic Reaction
Special Considerations
Syncope has occurred after epinephrine administration to asthmatic children.
May increase myocardial oxygen demand.
IV doses may be given through ET tube at 2 times the IV dose. Endotracheal
administration is a LAST RESORT.
Return to Table of Contents
EPINEPHRINE AUTO-INJECTOR (Adrenaline, Epi-Pen and Epi-Pen Jr.)
Pharmacology and Actions
Cardiovascular
1. Increased heart rate
2. Increased blood pressure
3. Arterial vasoconstriction
4. Increased myocardial contractile force
5. Increased myocardial oxygen consumption
6. Increased myocardial automaticity and irritability
Pulmonary
1. Potent bronchodilator
Indications
1. The patient has a history consistent with allergic reaction and exhibits any one of
the following:
a. Respiratory distress/airway compromise with tongue swelling or stridor.
b. Signs and symptoms of hypoperfusion (shock)
2. Patient has his/her own physician prescribed Epinephrine Auto-Injector.
Precautions
1. Increased myocardial oxygen consumption can precipitate angina or myocardial
infarction in patients with coronary artery disease.
2. Use with caution in patients with hypertension or known coronary artery disease.
Administration
1. The initial dosage for adult: one Epinephrine Auto-Injector (0.3 mg.)
2. The initial dosage for pediatric: one pediatric Epinephrine Auto-Injector (0.15
mg.)
3. Follow the standard drug administration protocol.
4. Contact on-line medical control for an order to administer if EMT-I or Basic
5. Standing order for Paramedics
6. Administer a single dose of Epinephrine Auto-Injector.
7. In a patient with hypoperfusion, early venous access should be anticipated.
8. Dispose of Auto-Injector in a biohazard container.
9. Reassess patient’s vital signs and condition 1-2 minutes after administration.
Side Effects and Special Notes
1. Experienced side effects include increased heart rate, pallor, dizziness, chest
pain, nausea, vomiting, excitabilty, anxiousness, headache, hypertension.
2. Only a single auto-injector should be utilized. Should the patient’s condition
persist or worsen, contact the base station for additional orders.
Go to Table of Contents
FENTANYL
Description
Used as an analgesic and sedative. Does not cause histamine release.
Onset & Duration
Onset: Within 5 minutes, with a peak effect within 30 minutes
Duration: 90 minutes
Indications
Pain management of extremity injuries; to be given only in the absence of any evidence
of head, chest or abdominal injuries
Management of pain secondary to selected medical problems (abdominal pain, back
pain, Chest Pain, kidney stones)
Burns
Contraindications
Hypersensitivity to opiates
Hypotension
Side Effects
Can cause significant respiratory depression and hypotension especially when used in
combination with other sedatives such as alcohol or benzodiazepines.
Can increase intracranial pressure
Chest wall rigidity has been reported with rapid administration that is unaffected by
narcan administration.
Pediatric patients may develop apnea without manifesting significant mental status
changes
Dosage and Administration
Adult:
The initial adult dose is 1-2 mcg / kg, SLOW IV bolus.
Pediatric (<12 years):
Initial dose is 1-2mcg / kg, SLOW IV bolus.
Contact base for any single or cumulative dose > 3 mcg/kg (not to exceed 100 mcg)
Combination Analgesia:
0.5 – 1.0 mcg/kg IV over two minutes
Repeat dose at 0.5 -1.0 mcg/kg over two minutes
Initial pain management : In certain circumstances it is appropriate to give
fentanyl via MAD device or nebulizer to initiate pain control. In the
hospice patient where no IV access is required, fentanyl may be
Nebulized. In the pediatric population it may be beneficial to initiate pain
control so IV access can be obtained more readily. In the pediatric
population MAD device administration should be the preferred route but
nebulization is acceptable. Once administered, every reasonable attempt
should be made to gain IV access
Go to Table of Contents
Special Notes:.Fentanyl should be given SLOWLY (over 2 min.) to prevent a
sudden onset of chest wall rigidity. This can be accomplished by diluting it
in a syringe or 50 ml bag and running it in over time.
Use with caution in patients with headache. If the headache is associated
with a clinical picture of CVA extra precaution should taken or the drug
withheld.
NOTE: Continuous pulse oximetry is necessary. Frequent evaluation of the
patient’s vital signs is also necessary. Emergency resuscitative equipment must
be immediately available
Protocol
Abdominal Pain
Combination Analgesia
Extremity Injuries
Return to Table of Contents
FUROSEMIDE (LASIX)
Description
Rapid acting, potent diuretic; inhibits re-absorption of Sodium Chloride. It is also a
venous dilator that decreases preload
Indications
Cardiogenic Pulmonary Edema
Contraindications
Pregnancy
Known hypersensitivity
Dehydration or shock
Side Effects
Hypotension
Headache
Dizziness
Hypovolemia
Nausea
Vomiting
Adverse Reactions
Rapid administration may cause auditory problems including tinnitus and hearing loss
Special Notes
Digitalis toxicity may be potentiated by the potassium depletion that can result from
furosemide administration.
Drug may be deactivated by exposure to light
Dosage and Administration
20-80 mg, IV bolus. Patients not on Lasix should receive 20 mg. Patients compliant with
Lasix should receive higher doses in the 40-80 mg range
Protocol
Pulmonary Edema
Go to Table of Contents
GLUCAGON
Description
Increases blood sugar concentration by converting liver glycogen to glucose. Glucagon
also causes relaxation of smooth muscle of the stomach, duodenum, small bowel, and
colon.
Onset & Duration
Onset: Within 1 min.
Duration: 3-6 min.
Indications
Altered level of consciousness where hypoglycemia is suspected and IV access is
unavailable.
May be used for beta-blocker overdose.
Contraindications
Hypersensitivity
Use with caution in patients with a history of cardiovascular disease, renal disease,
pheochromocytoma or insulinoma
Side Effects
Tachycardia
Headache
Nausea and vomiting
Dosage and Administration
Adult:
Hypoglycemia 1.0 mg, IM
Beta Blocker/Calcium Channel overdose 2.0 – 5.0mg IV bolus
Pediatric:
Hypoglycemia 0.1 mg/kg IM. Maximum dose 1.0 mg
Beta Blocker/Calcium Channel overdose 2.0 mg IV bolus
Protocol
Altered Mental Status
Seizures
Syncope
Poisoning/Overdose
Psychiatric/Behavioral
Go to Table of Contents
HALOPERIDOL (HALDOL)
Description
Haloperidol is a butyrophenone in the therapeutic class of antipsychotic medications.
Haloperidol produces a dopaminergic blockade, a mild alpha-adrenergic blockade, and
causes peripheral vasodilation. Its major actions are sedation and tranquilization.
Onset & Duration
Onset: Within 10 minutes after IM administration. Peak effect within 30 minutes
Duration: 2-4 hours (may be longer in some individuals)
Indications
Acts as a chemical restraint in patients that require transport and are behaving in a
manner that poses a threat to their own well-being or others.
Contraindications
Suspected myocardial infarction
Systolic BP of less than 100 mmHg or the absence of a radial pulse
Signs of sedation, respiratory or CNS depression
Known Parkinson’s Disease
Known pregnancy
History of severe liver or cardiac disease
Under 8 years of age
Precautions
A. Haldol may cause hypotension, tachycardia, and prolongation of the QT interval.
B. When administering this IM medication, paramedic must put patient on cardiac
monitor and establish an IV as soon as possible.
C. Due to the vasodilatory effect, haloperidol can cause a transient hypotension that
is usually self-limiting and can be treated effectively with position and fluids.
Haloperidol has also been known to cause tachycardia, which usually does not
require pharmacologic intervention.
D. Should profound hypotension occur that is unresponsive to positioning and fluid
therapy and vasopressors are required, epinephrine should not be used since
haloperidol may block its vasopressor activity and paradoxically further lower the
blood pressure. Haldol may also decrease the effectiveness of dopamine.
E. Some patients may experience unpleasant sensations manifested as
restlessness, hyperactivity, or anxiety following haloperidol administration.
F. Extra-pyramidal reactions have been noted hours to days after treatment, usually
presenting as spasm of the muscles of the tongue, face, neck, and back. This
may be treated with diphenhydramine.
G. Rare instances of neuroleptic malignant syndrome (very high fever, muscular
rigidity) have been known to occur after the use of haloperidol.
Dosage and Administration
Standing order:
5 - 10 mg, IM
May be followed with Diphenhydramine 25 – 50 mg, IV or IM
Base contact must be made for additional doses (consider if no effects within 10
minutes)
Go to Table of Contents
IPRATROPIUM BROMIDE (ATROVENT)
Description
Used as a bronchodilator that dries respiratory tract secretions.
Onset & Duration
Onset: 5-15 min. after inhalation
Duration: 6-8 hr after inhalation
Indications
Bronchospasm related to asthma, chronic bronchitis, or emphysema
Contraindications
Hypersensitivity reaction to this drug or atropine or soy or peanuts
Adverse Reactions
Palpitations
Dizziness
Anxiety
Tremors
Headache
Nervousness
Dry mouth
Precautions
Should not be used as the primary agent for treatment of bronchospasm.
Use with caution in patients with coronary artery disease.
Vital signs, and EKG must be monitored
How Supplied
Premixed Container: 0.5 mg in 2.5ml NS
Dosage and Administration
Bronchial asthma
Adult and Pediatrics over 2 years of age:
A. Mild / Moderate Bronchospasm:
1. Ipratropium may be used in combination with albuterol as described below if
patient is unresponsive to initial albuterol nebulization treatment.
B. Severe Bronchospasm:
1. Place one premixed vial of ipratropium (0.5 mg/2.5 ml) along with albuterol in
a nebulizer and administer via oxygen-powered nebulizer to create a fine
mist. If patient requires further treatment, continuous nebulization of plain
albuterol should be utilized
Protocol
Asthma
Chronic Obstructive Pulmonary Disease
Pediatric Respiratory Distress
Special Considerations
Can cause paradoxical bronchospasm. Discontinue treatment if this occurs.
Go to Table of Contents
IV SOLUTIONS
Pharmacology and Actions
Initiation of all IVs in the field in these protocols utilizes normal saline (NS). The
standard IV drip rate will be TKO unless a fluid bolus or fluid challenge is required.
TKO FLUID RATE
Indications
Prophylactic IV
Drug administration
Administration
TKO = 5-10 drops/min. or saline lock.
FLUID REPLACEMENT/BOLUS
Indications
Hemorrhagic shock, volume depletion (dehydration, burns, severe vomiting)
Shock caused by increased vascular space (neurogenic shock)
Precautions
A. In hemorrhagic shock, volume expansion with blood is the treatment of choice.
Normal saline will temporarily expand intravascular volume and "buy time," but
does decrease oxygen-carrying capacity, and is insufficient in severe shock.
Because of this, rapid transport is still necessary to treat severely hypovolemic
patients who need blood and possibly surgical intervention.
B. Volume overload is a constant danger, particularly in cardiac patients. Keep a
close eye on your IV rate during transport. For this reason, a fluid challenge (see
below) is more appropriate in cardiac patients.
Administration
20 ml/kg NS through large bore cannula, as rapidly as possible.
FLUID CHALLENGE
Indications
Hypotension felt to be secondary to cardiac cause (i.e. acute MI, pericardial tamponade,
cardiogenic shock)
Administration
250-500 ml rapidly through a large bore cannula, then reassess the patient.
Side Effects and Special Notes
A. Flow rate through a 14g cannula is twice the rate through an 18g cannula, and
volume administration in trauma patients can be accomplished more rapidly. If
the patient has poor veins, a smaller bore is better than no IV at all, in some
instances.
B. IVs in an unstable trauma patient should be placed enroute, and may be left to
the hospital setting for short transports. Do not delay transport in critical patients
for IV attempts.
C. If you are unable to start in two attempts, another qualified attendant may try, or
you may leave the IVs for the hospital.
Go to Table of Contents
D. If IV access is required but volume expansion is not, consider starting a saline
lock.
E. 1 ml/min = 60 microdrops/min = 15 regular drops/min.
Return to Table of Contents
LIDOCAINE 2% SOLUTION
Description
Used as a local anesthetic to reduce somatic pain during intraosseous fluid
administration.
Indications
Given following intraosseous insertion to patients over 8 years of age
Contraindications
Allergy to lidocaine or novacaine
Side Effects
Seizures
Drowsiness
Tachycardia
Bradycardia
Confusion
Hypotension
Precautions
Lidocaine is metabolized in the liver; elderly patients and those with liver disease or poor
liver perfusion secondary to shock or congestive heart failure are more likely to
experience side effect
Dosage and Administration
0.5 mg/kg IO bolus, slowly, maximum dose is 50 mg
Protocol
Intraosseous Administration
Special Notes
Diazepam should be available if seizures manifest
NOT to be used for treatment of cardiac events
Go to Table of Contents
Lidocaine (Xylocaine) Gel
Description
Used as a local anesthetic and lubricant to minimize discomfort and trauma during
airway insertion.
Indications
Prior to nasal pharangeal airway placement
Prior to nasal intubation
Contraindications
Allergy to lidocaine, xylocaine, or novacaine
Side Effects
When administered to nares side effects are uncommon and minimal
Precautions and Special Notes
Use with caution in patients with a heart rate <50 on in the presence of high degree AV
block. In Atrial fibrillation patients it may cause ventricular acceleration.
Should not be used to treat cardiac events.
Dosage and Administration
Administration can be accomplished in two ways:
1. Apply gel directly to airway
2. Insert gel directly in nare prior to airway insertion
As the medication is used to facilitate a procedure, the dose should be the amount
required to adequately lubricate the airway device. In nearly all cases this will not exceed
one container.
Protocol
Nasotracheal Intubation
Go to Table of Contents
MAGNESIUM SULFATE
Description
Magnesium sulfate reduces striated muscle contractions and blocks peripheral
neuromuscular transmission by reducing acetylcholine release at the myoneural
junction. In cardiac patients, it stabilizes the potassium pump, correcting repolarization.
It also shortens the Q-T interval in the presence of ventricular arrhythmias due to drug
toxicity or electrolyte imbalance. In respiratory patients, it may act as a bronchodilator in
acute bronchospasm due to asthma or other bronchospastic diseases. For best results,
it should be used after normal field inhalation therapy has been attempted.
For obstetric cases, it controls seizures by blocking neuromuscular transmission. Also
lowers blood pressure and decreases cerebral vasospasm
Indications
A. Cardiac: Refractory VF and pulseless VT (after amiodarone) Cardiac arrest from
suspected torsade de pointes Wide complex tachycardia with pulse and without
poor perfusion
B. Respiratory: Acute bronchospasm unresponsive to continuous inhaled betaagonists, ipratropium, and epinephrine.
C. Obstetrics: Pregnancy > 20 weeks with signs and symptoms of pre-eclampsia,
defined as:
1. Blood pressure > 180 mmHg systolic or > 120 mmHg diastolic with altered
mental status or
2. Seizures (eclampsia)
Precautions
Heart block
Decrease in respiratory or cardiac functions
Use with caution in patients on digitalis
Adverse Reactions
Reduced heart rate
Circulatory collapse
Respiratory depression
Dosage and Administration
Cardiac Arrest (refractory VF/VT; Torsades de Pointes)
2 gm, IV bolus.
Wide complex tachycardia with a pulse and poor perfusion
2.0 gm, IV bolus, over 2 minutes
Acute bronchospasm
2.0 gm, IV bolus, over 2 minutes
Seizure activity associated with pregnancy:
Mix 6.0 gm, IV drip, diluted in 50 ml of Normal Saline (0.9 NS), over 15-30 minutes.
If no IV access can be obtained, IM injection of 4g in each buttock (8g total)
Protocol
Ventricular Fibrillation/Pulseless Ventricular Tachycardia
Asthma
Chronic Obstructive Pulmonary Disease
Obstetric Complications
Return to Table of Contents
Special Considerations
Principal side effect is respiratory depression
NOT to be used in pediatric patients
Return to Table of Contents
MARK I NERVE AGENT ANTIDOTE KIT
Description
Nerve agents can enter the body by inhalation, ingestion, and through skin. These
agents are absorbed rapidly and can produce injury or death within minutes. The Mark I
Nerve Agent Antidote Kit consists of two auto-injectors for self and/or buddy
administration. One injector contains atropine and another which contains pralidoxime
chloride (2-PAM)
Indications
Suspected nerve agent exposure accompanied with signs and symptoms of nerve agent
poisoning
Injection Sites
Outer thigh – mid-lateral thigh (preferred site)
Buttocks – upper lateral quadrant of buttock (gluteal) in thin individuals
Procedure
A. Utilize appropriate safety precautions including BSI
B. Remove atropine injector (smaller of the two). Once removed, it is now active.
Use caution not to self-inject.
C. Hold securely in one hand and place against injection site on patient.
D. Firmly apply constant pressure against site for at least 10 seconds.
E. Repeat using the 2-PAM injector.
F. Contact receiving hospital to set up appropriate decontamination facilities.
Dosage and Administration
Atropine injector contains 2 mg
2-PAM injector contains 600 mg
No more than three (3) sets of antidote should be administered.
Protocol
WMD exposure
Special Considerations
Within 5-10 minutes after administration, tachycardia and dry mouth may occur. This
indicates the antidote is working and that you should not need another injection
Usage Instructions
Go to Table of Contents
1. Hold the set of auto-injectors with the non-dominant hand and by the plastic clip.
2. Grasp the atropine injector
3. Remove the atropine injector with the thumb and first two fingers.
4. Repeat using the 2-PAM injector
Return to Table of Contents
METERED DOSE INHALER
Medication Name
Generic: albuterol, isoetharine, metaproternol
Trade: Proventil, Ventolin, Bronchosol, Alupent, Metaprel
Pharmacology and Actions
A. These medications are all bronchodilators. These medications have a rapid onset
of action and duration between 2 and 4 hours. All of these agents will have
cardiovascular side effects, including increasing heart rate and increasing blood
pressure.
Indications
A. Wheezing due to bronchial asthma, COPD, or bronchospasm related to an
allergic reaction.
B. Patient has chief complaint of shortness of breath and has a history of bronchial
asthma or COPD.
C. Patient has a physician prescribed bronchial inhaler.
Note: The bronchodilator must be prescribed for this patient. If in doubt, contact medical
control. No over-the–counter medications should be administered.
Precautions
A. If the patient is not breathing adequately on his/her own, the treatment of choice
is ventilation.
B. The patient in need of a metered dose inhaler for wheezing should also be on
supplemental oxygen.
Administration
A. Follow the steps in the standard drug administration protocol.
B. Administer supplemental oxygen.
C. Confirm prescription identification.
D. Ascertain how many times the patient has used the inhaler.
E. Contact on-line medical control for an order to administer.
F. Shake the inhaler vigorously.
G. Have the patient place the actuator two finger breadths away from his/her
mouth.(If the patient has a spacer, use it.) The patient should begin to inhale
deeply as he/she can.
H. Depress the canister shortly after inhalation has begun. Have the patient hold
his/her breath as long as comfortably possible, then exhale. This should be
repeated to accomplish the two puffs.
I. In the event of a prolonged transport and the patient is not getting better, contact
base station for additional orders.
Side Effects and Special Notes
Some common side effects which may be experienced include, hypertension, chest
pain, increased heart rate, nervousness, tremors, nausea, vomiting and sore throat.
Go to Table of Contents
METHYLPREDNISOLONE (SOLU-MEDROL)
Description
Methylprednisolone is a synthetic steroid that suppresses acute and chronic
inflammation and may alter the immune response. In addition, it potentiates vascular
smooth muscle relaxation by beta-adrenergic agonists and may alter airway
hyperactivity. An additional newer use is for reduction of posttraumatic spinal cord
edema.
Indications
Anaphylaxis
Severe asthma
COPD
Contraindications
Hypersensitivity
Adverse Reactions
Gastrointestinal bleeding
Hypertension
Dosage and Administration
Adult: 125 mg, IV bolus, slowly, over 2 minutes
Pediatric: 2 mg/kg, IV bolus, slowly, over 2 minutes
Protocol
Asthma
Chronic Obstructive Pulmonary Disease
Special Considerations
• Must be reconstituted and used immediately
• Be aware that the effect of methylprednisolone is generally delayed for several
hours. Although it is worthwhile to administer methylprednisolone early in the
treatment of a patient with severe respiratory distress or anaphylaxis you may not
see any effect from the drug for several hours.
• Methylprednisolone is not considered a first line drug. Initial effects can be seen
at about 20 minutes but the medication effect will not peak for about 2 hours. Be
sure to attend to the patient’s primary treatment priorities (i.e. airway, ventilation,
beta-agonist neublization) first. If primary treatment priorities have been
completed and there is time while in route to the hospital, then
methylprednisolone can be administered. Do not delay transport to administer
this drug
• Use in Pregnancy: Since adequate human reproduction studies have not been
done with this medication, the use of this drug in pregnancy or with nursing
mothers requires that the possible benefits of the drug be weighed against the
potential hazards to the mother and the embryo or fetus.
Go to Table of Contents
MIDAZOLAM (VERSED)
Description
Midazolam HCl is a water-soluble benzodiazepine that may be administered for sedation
to relieve apprehension or impair memory. It is also used as an anti-convulsant.
Indications
Sedation for cardioversion or transcutaneous pacing (TCP)
Status Epilepticus in adults; as an IM benzodiazepine when two IV attempts have been
unsuccessful. If an IV is obtained, then diazepam should be used. combination
analgesia, combative patients, and severe anxiety states.
Contraindications
Hypersensitivity to benzodiazepines
Acute narrow angle glaucoma
Adverse Reactions
Significant hypotension
Significant respiratory depression
Apnea
Amnesia
Drug Interactions
Sedative effect of midazolam may be heightened by associated use of barbiturates,
alcohol, CNS depressants, or narcotics.
Dosage and Administration
C. ADULT DOSAGES
1. Combination Analgesia
1-2 mg IV after Fentanyl or Morphine administration
2. Status Epilepticus
2.5 mg IV/ 5 mg IM or IN (MAD Device)
3. Combative Patient
2.5 mg IV / 5 mg IM
4. Severe Anxiety State
0.5 - 1 mg IV/IM
Special Considerations
Midazolam should be given slowly. This may be accomplished in different ways.
1. The appropriate dose my be diluted in a 10cc syringe with normal saline and pushed
slowly over 2 minutes.
2. The appropriate dose may be placed in a 50cc bag of normal saline and administered over
2 minutes via a microdrip administration set.
3. The appropriate dose may be administered Intra Nasally via the MAD device in Status
Seizure
Go to Table of Contents
D. PEDIATRIC DOSAGES
1. Combination Analgesia
a. 0.05 mg/kg IV
b. Maximum dose 2 mg
2. Status Epilepticus
a. 0.10 mg/kg IV/IM/IO/IN
b. Maximum dose 2 mg
Protocol
Bradycardia with a pulse
Combination Analgesia
Wide Complex Tachycardia
Seizures
Hyperthermia
Pediatric Seizures
Combination Analgesia
Special Considerations
Provide continuous monitoring of respiratory and cardiac function.
Have resuscitation equipment and medication readily at hand.
Consider lower doses for elderly patients
MORPHINE SULFATE
Description
Morphine sulfate is a natural opium alkaloid that increases peripheral venous
capacitance and decreases venous return. It promotes analgesia, euphoria, and
respiratory and physical depression. Morphine sulfate is a schedule II drug.
Onset & Duration
Onset: Immediate
Duration: 2-7 hr
Indications
Chest pain of a likely cardiac origin
Severe burns
Cardiogenic pulmonary edema
Isolated extremity injuries
Pain management
Contraindications
Hypersensitivity
Hypovolemia
Hypotension (relative)
Head injury or undiagnosed abdominal pain
Side effects
Hypotension
Nausea and/or vomiting
Vasodilation (Tachycardia or bradycardia)
Respiratory depression
Dosage and Administration
Adult:
Cardiac Chest Pain
Initial dose 1 – 4 mg. Repeat doses of 2.0 mg, up to 10 mg. IV only
Injuries / Burns
Initial dose 0.1 mg/kg slow IV/IM/IN, up to 10 mg.
Pediatric:
0.1-0.2 mg/kg, IV/IM SLOWLY. Maximum single dose is 5.0 mg.
Protocol
Chest pain
Hypertension
Pulmonary Edema
Abdominal Pain
Extremity Injuries
Burns
Special Considerations
Go to Table of Contents
IV is the preferred route for all indications. IM or IN should only be used for pain if an IV
cannot be obtained and should NOT be used for cardiac indications.
Vital signs, including pulse oximetry and EKG when available, should be monitored
regularly
Naloxone and resuscitation equipment should be readily available
Return to Table of Contents
Seizures
Poisoning/Overdose
Psychiatric/Behavioral
Infant and Child Resuscitation
Pediatric Altered Mental Status
Special Considerations
Patients receiving Naloxone must be transported to a hospital
If dose is given endotracheally, double the dose. This should be an absolute last resort.
Give with extreme caution prior to administering endotracheally as the patient may
awake violently and the endotracheal tube placement may be displaced.
Return to Table of Contents
NITROGLYCERINE (NITROSTAT, NITROQUICK, etc)
Description
It was originally believed that nitrates and nitrites dilated coronary blood vessels, thereby
increasing blood flow to the heart. It is now believed that atherosclerosis limits coronary
dilation and that the benefits of nitrates and nitrites result from dilation of arterioles and
veins in the periphery. The resulting reduction in preload and to a lesser extent in
afterload decreases the work load of the heart and lowers myocardial oxygen demand.
Nitroglycerin is very lipid soluble and is thought to enter the body from the Gl tract
through the lymphatics rather than the portal blood.
Onset & Duration
Onset: 1-3 min.
Duration: 20-30 min.
Indications
Angina
Chest, arm, or neck pain caused by coronary ischemia
Patients with 12-lead evidence of acute MI, with or without chest pain
Control of hypertension in angina, acute MI, or hypertensive encephalopathy without
evidence of CVA
Cardiogenic pulmonary edema: to increase venous pooling, lowering cardiac preload
and afterload
Contraindications
Blood Pressure under 90 mmHg
Precautions
Hypersensitivity
Use with caution in patients with EKG evidence of right ventricular infarction
Hypotension
Patients taking erectile dysfunction drugs should not receive nitroglycerine in any form
Adverse Reactions
Transient headache
Postural syncope
Hypotension
Nausea and vomiting
Flushing
Dizziness
Burning under the tongue
Dosage and Administration
• 0.4 mg (1/150 gr) sublingually or spray, every 5 minutes. Vital signs must be reassessed after each administration.
• Nitropaste 1 inch (if available)
Protocol
Premature Ventricular Contractions (PVCs)
Chest Pain
Hypertension
Go to Table of Contents
Pulmonary Edema
Special Considerations
Susceptibility to hypotension in older adults increases.
Nitroglycerin loses potency when exposed to light or heat.
Must be kept in airtight, dark containers.
Because nitroglycerin causes generalized smooth muscle relaxation, it may be effective
in relieving chest pain caused by esophageal spasm
Return to Table of Contents
ODANSETRON (ZOFRAN)
Description
Odansetron is a selective 5-HT3 receptor agonist. Mechanism of action has not been
fully characterized. It is not certain whether odansetron’s antiemetic action is mediated
centrally, peripherally, or in both sites.
Indications
Nausea with concern for potential vomiting
Vomiting
Contraindications
Patients with a known hypersensitivity to odansetron.
Precautions
Odansetron is listed as a category B with regard to use in pregnancy.
Dosage and Administration
Adult:
4 mg undiluted SLOW IV push over 2 to 5 minutes or IM. Repeat dose 4mg.
CONTACT BASE for cumulative dose above 8mg.
Pediatric (1 to 12 years of age):
under 40 kg: 0.1 mg/kg SLOW IV push over 2 to 5 minutes or IM or SL**
over 40 kg: 4 mg SLOW IV push over 2 to 5 minutes or IM or SL**
**(For SL administration, the IV solution may be used, simply remove the
needle and administer under the tongue)
Protocol
Antiemetic situations
Go to Table of Contents
ORAL GLUCOSE (GLUTOSE, INSTA-GLUCOSE)
Description
Glucose is the body's basic fuel and is required for cellular metabolism. A sudden drop
in blood sugar level will result in disturbance of normal metabolism, manifested clinically
as decrease in mental status, sweating, and tachycardia. Further decreases in blood
sugar may result in coma, seizures, and cardiac arrhythmia. Serum glucose is regulated
by insulin, which stimulates storage of excess glucose from the body's blood stream, and
glucagon, which mobilizes stored glucose into the blood stream. The oral glucose paste
is rapidly absorbed into the oral mucosa, thus elevating the body's blood glucose level.
Indications
Hypoglycemia
Altered Mental Status with a history of (hypoglycemia) diabetes
Contraindications
Inability to swallow
Patient who may experience an airway obstruction from administration
Administration
The dosage of oral glucose is one full tube.
Follow the standard drug administration protocol.
Squeeze a small portion of the tube (approximately 1/3) into the patient's mouth between
the cheek and gum. Or, utilizing a tongue depressor, deposit a small portion of the tube
(approximately 1/3) onto the tongue depressor and slide it into the patient's mouth
between the cheek and gum. Repeat the procedure until one full tube of glucose has
been administered.
Reassess the vital signs and the patient's condition
Protocol
Altered Mental Status
Special Notes
There are few, if any, side effects with this medication.
Be aware of possible airway obstruction. Have suction available.
Go to Table of Contents
OXYGEN
Description
Oxygen added to the inspired air increases the amount of oxygen in the blood, and
thereby increases the amount delivered to the tissue. Tissue hypoxia causes cell
damage and death. Breathing, in most people, is regulated by small changes in the
acid-base balance and CO2 levels. It takes relatively large decreases in oxygen
concentration to stimulate respiration.
Indications
Suspected hypoxemia or respiratory distress from any cause
Acute chest or abdominal pain
Hypotensive states from any cause
Trauma
All acutely ill patients
Any suspected carbon monoxide poisoning
Pregnant females
Precautions
• If the patient is not breathing adequately, the treatment of choice is assisted
ventilation, not just oxygen.
• A small percentage of patients with chronic lung disease breathe because they
are hypoxic. Administration of oxygen will inhibit their respiratory drive. Do not
withhold oxygen because of this possibility. Be prepared to assist
ventilations if needed.
• When pulse oximetry is available, titrate Sa O2 to 90% or greater. This may take
some time. Be patient within reason.
• In the COPD patient: increase oxygen in increments of 2 liters/minute every 2 3
minutes until improvement is noted (color improvement or increase in mental
status).
Administration
Flow
Low Flow
Moderate Flow
High Flow
LPM dosage
1-2 LPM
3-9 LPM
10-15 LPM
Indications
Minor medical / trauma
Moderate medical / trauma
Severe medical / trauma
Special Notes
Restlessness may be an ominous sign of hypoxia.
Some people become more agitated when a nasal cannula is applied, particularly when
it is not needed. Acquiesce to your patient if it is reasonable.
Nasal prongs work equally well on nose and mouth breathers, except babies.
Non humidified oxygen is drying and irritating to mucous membranes.
Oxygen toxicity is not a hazard of short term use.
Do not use permanently mounted humidifiers. If the patient warrants humidified oxygen,
use a single patient use device.
During long transports for high altitude illness, reduce oxygen flow from high to low, to
conserve oxygen.
Go to Table of Contents
METHOD
Room Air
Nasal Cannula
Simple Face Mask
Non-rebreather Mask
Mouth to Mask
Bag/Valve/Mask (BVM)
OXYGEN FLOW RATES
FLOW RATE
1 LPM
2 LPM
6 LPM
8 - 10 LPM
10 LPM
10 LPM
15 LPM
Room Air
12 LPM
10-15 LPM
hand-regulated
OXYGEN INSPIRED AIR
(approximate)
21%
24%
28%
44%
40-60%
90%
80%
50%
21%
40%
90-100%
100%
Bag/Valve/Mask with Reservoir
OXYGEN -powered breathing
device
NOTE:
Most hypoxic patients will feel more comfortable with an increase of inspired oxygen from
21% to 24%.
Return to Table of Contents
PHENYLEPHRINE (INTRANASAL)
Description
Used for topical nasal administration, phenylephrine primarily exhibits alpha adrenergic
stimulation. This stimulation can produce moderate to marked vasoconstriction and
subsequent nasal decongestion.
Indications
Prior to nasotracheal intubation to induce vasoconstriction of the nasal mucosa
Pain related to middle ear congestion or infection
Epistaxis without hypertension
Contraindications
Known Hypersensitivity
Precautions
Avoid administration into the eyes, as it will cause dilation of the pupils
Dosage and Administration
Instill two drops of 1% solution in the nostril prior to attempting nasotracheal intubation
In epistaxis moisten gauze and place in affected nare
Side Effects
Headache, dizziness, insomnia, sedation, hypertension, mydriasis
Protocol
Nasotracheal Intubation
Go to Table of Contents
PROMETHAZINE (PHENERGAN)
Description
Promethazine is a first-generation H1 receptor antagonist antihistamine and antiemetic
medication which acts centrally and has sedative properties. It is related to the
phenothiazine family and may cause extrapyramidal and anticholinergic symptoms.
Indications
Nausea with concern for potential vomiting
Vomiting
Contraindications
Patients in a comatose state
CNS depression from alcohol or drug usage
Pediatric patients 2 years old or younger
Precautions
Promethazine does not eliminate the need to monitor the airway.
Respiratory depression may occur if the patient has used alcohol or drugs.
Extrapyramidal effects are more likely to manifest in pediatric patients with acute illness
or dehydration
Side Effects
Hypotension if administered too quickly. Give Normal Saline to reverse the hypotension.
Extrapyramidal effects. Give Benadryl 25 mg to reverse these effects.
Dry mouth
Dilated pupils
Incontinence/Constipation
Dosage and Administration
Adult: 12.5 mg, IV bolus slowly over 1-2 minutes.
Consider 6.25mg dosing for patients that have:
1. Consumed alcohol
2. Been given narcotic analgesics
3. Present with signs/symptoms of CHI
Pediatric (3-8 years of age): 0.25 mg/kg IV bolus slowly or IM.
Geridatric: 6.25mg Slow IVP
FOR REPEAT DOSES consider use of Ondansetron (Zofran) or a repeat dose of
6.25mg after 15 min.
Protocol
Nausea/Vomiting
Return to Table of Contents
RACEMIC EPINEPHRINE (VAPONEPHRINE)
Description
Racemic epinephrine is an epinephrine preparation in a 1:1000 dilution for use by oral
inhalation only. Effects are those of epinephrine. Inhalation causes local effects on the
upper airway as well as systemic effects from absorption. Vasoconstriction may reduce
swelling in the upper airway, and beta effects on bronchial smooth muscle may relieve
bronchospasm.
Onset & Duration
Onset: 1-5 minutes
Duration: 1-3 hours
Indications
Life threatening airway obstruction suspected secondary to croup or epiglottitis
Laryingeal Edema
Side Effects
Tachycardia
Anxiety
Palpitations
Dosage and Administration
Do NOT delay transport to begin administration
0.5 ml racemic epinephrine (acceptable dose for all ages) mixed in 2 ml saline, via
nebulizer at 6-8 LPM to create a fine mist
If racemic epinephrine is not available plain L-epinephrine may be used:
Place 5 mg (5.0 ml of a 1:1,000 solution) undiluted in a nebulizer at 6-8 LPM to create a
fine mist
For infants <10 kg, the recommended dose is 0.5 mg/kg undiluted (0.5 ml/kg of 1:1,000
solution) of L-epinephrine.
Protocol
Pediatric Respiratory Distress
Special Considerations
Always try to utilize the parents help as the mask may frighten children
Is heat and photo-sensitive and needs to be protected from heat and light sources
Do not confuse the side effects with respiratory failure or imminent respiratory arrest.
If respiratory arrest occurs, it is usually due to patient fatigue or laryngeal spasm.
Complete obstruction is not usually present. Ventilate the patient, administer oxygen,
and transport rapidly. If you can ventilate and oxygenate the patient adequately with
mouth-to-mask, pocket mask, or BVM, intubation is best left to a specialist in a controlled
setting
Try to differentiate croup from epiglottitis by history. Cough is usually present in croup.
Do not use a tongue blade to examine the back of the throat. The diagnosis is
frequently difficult in the field, but a critical patient deserves a trial of racemic epinephrine
during transport. Although used as specific therapy for croup, it may also buy some time
in patients with epiglottitis
Go to Table of Contents
SODIUM BICARBONATE
Description
Sodium bicarbonate is an alkalotic solution, which neutralizes acids found in the body.
Acids are increased when body tissues become hypoxic due to cardiac or respiratory
arrest.
Indications
Tricyclic overdose with arrhythmias, widened QRS complex, hypotension, seizures
Consider in patients with prolonged cardiac arrest.
Consider in dialysis patients with cardiac arrest (presumed secondary to hyperkalemia)
Contraindications
Metabolic and respiratory alkalosis
Hypocalcemia
Hypokalemia
Adverse Reactions
Metabolic alkalosis
Hyperosmolarity may occur, causing cerebral impairment
Drug Interactions
May precipitate in calcium solutions.
Alkalinization of urine may increase half-lives of certain drugs.
Vasopressors may be deactivated.
Dosage and Administration
A. STANDING ORDER in cardiac arrest
B. CONTACT BASE for all other indications.
C. Solutions:
1. Adult / Pediatric: 8.4% = 1.0 mEq/ml
2. Neonatal: 4.2% = 0.5 mEq/ml
a. (Either prepackaged or adult solution diluted 1:1 with sterile NS or water)
D. For cardiac arrest / Tricyclic Overdose:
1. Adult: 1 mEq/kg (1 ml/kg)
2. Pediatric: 1 mEq/kg (1 ml/kg)
3. Neonatal: 1 mEq/kg (2 ml/kg)
Protocol
Asystole
Poisoning/Overdose
Special Considerations
• Sodium bicarbonate administration increases CO2 which rapidly enters cells,
causing a paradoxical intracellular acidosis.
• Each ampule of sodium bicarbonate contains 44-50 mEq of sodium. This
increases intravascular volume, which increases the workload of the
heartSodium bicarbonate's lack of proven efficacy and its numerous adverse
effects have lead to the reconsideration of its role in cardiac resuscitation.
Effective ventilation and circulation of blood during CPR are the most effective
treatments for acidemia associated with cardiac arrest
Go to Table of Contents
•
•
•
•
Administration of sodium bicarbonate has not been proven to facilitate ventricular
defibrillation or to increase survival in cardiac arrest. Metabolic acidosis lowers
the threshold for the induction of ventricular fibrillation, but has no effect on
defibrillation threshold.
The inhibition effect of metabolic acidosis on the actions of catecholamines has
not been demonstrated at the pH levels encountered during cardiac arrest.
Metabolic acidosis from medical causes (e.g. diabetes) develops slowly, and field
treatment is rarely indicated.
Sodium bicarbonate may be considered for the dialysis patient in cardiac arrest
due to suspected hyperkalemia.
Return to Table of Contents
TOPICAL OPHTHALMIC ANESTHETICS (TETRACAINE)
Description
Used for topical administration as a pain reliever for eye irritation. Only proparacaine
and tetracaine are approved for use.
Indications
Used to provide topical ophthalmic anesthesia during transport of patients with actual or
potential serious eye injuries that present with a "foreign body sensation"
Contraindications
Known allergy to local anesthetics (Novacaine, Lidocaine, Xylocaine, etc.)
Eyelid lacerations
Global lacerations or rupture
Discoloration of medication
Precautions
Occasional burning/stinging can occur when initially applied, although this is usually
transient
Dosage and Administration
Instill two drops into affected eye. Repeat only with Base Contact and physician consult
Protocol
Eye injury
Special Considerations
This is single patient use. Unused portions are to be discarded and only new bottles are
to be used.
Do not administer until patient consents to transport and transport has begun
Topical ophthalmic anesthetics should never be given to a patient for self-administration
Go to Table of Contents
Inter-Facility Drug Protocol
Antibiotics
Description
Due to the vast number of antibiotics available, it is not practical to develop a written
protocol for every antibiotic. Therefore, this protocol shall serve as a general guide to
the inter-facility maintenance of antibiotic drips.
Indications
Treatment and prevention of Bacterial Infections
Contra-Indications:
Hypersensitivity
Precautions:
Adverse Reactions
Allergic or Anaphylactic reactions
Dosage and Administration
• The Paramedic shall consult drug reference guide for proper dosage and
administration information.
Protocol
1. For inter-facility transport only when initiated by a sending facility.
2. Must be maintained on an IV pump
3. Paramedic must familiarize him/herself with proper dosage and administration
information utilizing appropriate drug guide or manufacturer information as well as
general information regarding the particular antibiotic.
4. The Paramedic shall consult with Nursing staff or Medical control to obtain any
specific instructions for transport.
5. Signs and Symptoms of anaphylaxis should be watched for at all times.
6. Treatment of allergic or anaphlaxtic reactions shall be per normal ALS protocol.
7. In the event of allergic or anaphlaxtic reaction the antibiotic shall be stopped and
disconnected from the patient, and medical control should be advised.
Return to Table of Contents
Reference Material:
Antibiotics[6]
Generic Name
Brand Names
Common Uses
Possible Side Effects
Aminoglycosides
Amikacin
Amikin
Gentamicin
Garamycin
Kanamycin
Kantrex
Neomycin
Netilmicin
Netromycin
Streptomycin
Tobramycin
Nebcin
Paromomycin
Humatin
Infections caused by
Gram-negative
bacteria, such as
Escherichia coli and
Klebsiella particularly
Pseudomonas
aeruginosa. Effective
against Aerobic
bacteria (not
obligate/facultative
anaerobes).
Hearing loss
Vertigo
Kidney damage
Ansamycins
Geldanamycin
Experimental, as
antitumor antibiotics
Herbimycin
Carbacephem
Loracarbef
Lorabid
Carbapenems
Ertapenem
Invanz
Doripenem
Finibax
Imipenem/Cilastatin
Primaxin
Meropenem
Merrem
Bactericidal for both
Gram-positive and
Gram-negative
organisms via
inhibition of cell wall
synthesis and
therefore useful for
empiric broadspectrum antibacterial
coverage. (Note
MRSA resistance to
this class.)
Gastrointestinal
upset and diarrhea
Nausea
Seizures
Headache
Rash and Allergic
reactions
Cephalosporins (First generation)
Cefadroxil
Duricef
Cefazolin
Ancef
Cefalotin or Cefalothin
Keflin
Cefalexin
Keflex
Return to Table of Contents
Gastrointestinal
upset and diarrhea
Nausea (if alcohol
taken concurrently)
Allergic reactions
Cephalosporins (Second generation)
Cefaclor
Ceclor
Cefamandole
Mandole
Cefoxitin
Mefoxin
Cefprozil
Cefzil
Cefuroxime
Ceftin, Zinnat
Gastrointestinal
upset and diarrhea
Nausea (if alcohol
taken concurrently)
Allergic reactions
Cephalosporins (Third generation)
Cefixime
Suprax
Cefdinir
Omnicef
Cefditoren
Spectracef
Cefoperazone
Cefobid
Cefotaxime
Claforan
Gastrointestinal
upset and diarrhea
Cefpodoxime
Nausea (if alcohol
Ceftazidime
Fortaz
Ceftibuten
Cedax
taken concurrently)
Allergic reactions
Ceftizoxime
Ceftriaxone
Rocephin
Cefdinir
Cephalosporins (Fourth generation)
Gastrointestinal
upset and diarrhea
Cefepime
Maxipime
Nausea (if alcohol
taken concurrently)
Allergic reactions
Glycopeptides
Teicoplanin
Vancomycin
Vancocin
Macrolides
Azithromycin
Zithromax,
Sumamed,
Zitrocin
Clarithromycin
Biaxin
Dirithromycin
Erythromycin
Return to Table of Contents
Streptococcal
infections, syphilis,
respiratory infections,
mycoplasmal
infections, Lyme
disease
Nausea, vomiting,
and diarrhea (especially
at higher doses)
Jaundice
Roxithromycin
Troleandomycin
Telithromycin
Ketek
Pneumonia
Visual Disturbance, LIVER
TOXICITY. This medication's
approval in the U.S. was
controversial, and one doctor
went to jail in followup
attempts to ascertain its
safety because she falsified
the results of her part of the
testing precisely because it
seemed to cause liver
problems, including liver
failure, to a greater extent
than would be expected of a
common-use antibiotic.[7]
Antimetabolite,
Anticancer
Spectinomycin
Monobactams
Aztreonam
Penicillins
Amoxicillin
Novamox
Ampicillin
Azlocillin
Gastrointestinal
Carbenicillin
Cloxacillin
Wide range of
infections; penicillin
used for streptococcal
infections, syphilis,
and Lyme disease
Dicloxacillin
Flucloxacillin
Mezlocillin
Nafcillin
upset and diarrhea
Allergy with serious
anaphylactic reactions
Brain and kidney
damage (rare)
Penicillin
Piperacillin
Ticarcillin
Polypeptides
Bacitracin
Eye, ear or bladder
infections; usually
applied directly to the Kidney and nerve damage
(when given by injection)
eye or inhaled into
the lungs; rarely given
by injection
Colistin
Polymyxin B
Quinolones
Ciprofloxacin
Enoxacin
Ciproxin,
Urinary tract
CiploxESTECINA infections, bacterial
prostatitis,
Return to Table of Contents
Nausea (rare), tendinosis
(rare)
Gatifloxacin
Tequin
Levofloxacin
Levaquin
Lomefloxacin
Moxifloxacin
Avelox
Norfloxacin
NOROXIN
Ofloxacin
Ocuflox
Trovafloxacin
Trovan
community-acquired
pneumonia, bacterial
diarrhea,
mycoplasmal
infections, gonorrhea
Sulfonamides
Mafenide
Nausea, vomiting,
Prontosil (archaic)
and diarrhea
Sulfacetamide
Sulfamethizole
Urinary tract
infections (except
sulfacetamide and
mafenide); mafenide
is used topically for
burns
Sulfanilimide (archaic)
Sulfasalazine
Sulfisoxazole
Trimethoprim
TrimethoprimSulfamethoxazole (Cotrimoxazole) (TMPSMX)
Allergy (including
skin rashes)
Crystals in urine
Kidney failure
Decrease in white
blood cell count
Bactrim
Sensitivity to sunlight
Tetracyclines
Demeclocycline
Doxycycline
Vibramycin
Minocycline
Minocin
Oxytetracycline
Terracin
Tetracycline
Sumycin
Gastrointestinal
upset
Syphilis, chlamydial
infections, Lyme
disease,
mycoplasmal
infections, acne
rickettsial infections
Sensitivity to sunlight
Staining of teeth
(especially in children)
Potential toxicity to
mother and fetus during
pregnancy
Others
Arsphenamine
Salvarsan
Chloramphenicol
Chloromycetin
Clindamycin
Cleocin
Lincomycin
Return to Table of Contents
Spirochaetal
infections (obsolete)
acne infections,
prophylaxis before
surgery
acne infections,
prophylaxis before
surgery
Ethambutol
Antituberculosis
Fosfomycin
Fusidic acid
Fucidin
Furazolidone
Isoniazid
Antituberculosis
Linezolid
Zyvox
Metronidazole
Flagyl
Mupirocin
Bactroban
Nitrofurantoin
Macrodantin,
Macrobid
Giardia
Platensimycin
Pyrazinamide
Antituberculosis
Quinupristin/Dalfopristin Syncercid
Rifampin or Rifampicin
Tinidazole
Return to Table of Contents
Binds to the β subunit
of "RNA polymerase"
to inhibit transcription Reddish-orange sweat, tears,
of mostly "Gramand urine
positive" and
"mycobacteria"
Heparin
Inter-Facility Drug Protocol
Description
Heparin is an anticoagulant (blood thinner)
Indications
Treatment and prevention of blood clots often associated in treatment of:
• Acute Coronary Syndrome
• Pulmonary Embolus
• Pre-Operatively
• A-Fib
• DVT
Contraindications
• Known Hypersensitivity
• Active Bleeding Disorder
Precaution for Patients with:
• Liver Disease
• Menstrual period
• Hypertension
• GI Problems
• Endocarditis
Side Effects
• Bleeding
• Bruising
• Allergic Reaction
Dosage and Administration
• The following is provided for information and reference purposes only.
• Traditional regimen calls for Bolus dose followed by maintenance infusion.
• Normal Bolus 50-100 units/kg (70units/Kg average)
• Normal Infusion 15-25 units/kg/hr (Typically around 20ml/hr)
Protocol
1. For inter-facility transport only when initiated by a sending facility.
2. Heparin infusions must be maintained on an IV pump at all times during transport
at facility initiated maintenance dosage.
3. Heparin dosage may not be titrated in the interfacility environment.
4. Heparin Bolus may not be given.
5. Heparin infusion should be stopped if life threatening bleeding develops. (CVA,
GI Bleed, etc.)
6. If infusion is stopped, medical control or the receiving facility should be consulted
for further instructions and consultation.
Return to Table of Contents
Inter-Facility Drug Protocol
Nitroglycerin Drip
Description
It was originally believed that nitrates and nitrites dilated coronary blood vessels, thereby
increasing blood flow to the heart. It is now believed that atherosclerosis limits coronary
dilation and that the benefits of nitrates and nitrites result from dilation of arterioles and
veins in the periphery. The resulting reduction in preload and to a lesser extent in
afterload decreases the work load of the heart and lowers myocardial oxygen demand.
Nitroglycerin is very lipid soluble and is thought to enter the body from the Gl tract
through the lymphatics rather than the portal blood.
Indications
Angina
Chest, arm, or neck pain caused by coronary ischemia
Patients with 12-lead evidence of acute MI, with or without chest pain
Control of hypertension in angina, acute MI, or hypertensive encephalopathy without
evidence of CVA
Cardiogenic pulmonary edema: to increase venous pooling, lowering cardiac preload
and afterload
Contra-Indications:
Hypersensitivity
Hypotension
Patients taking erectile dysfunction drugs should not receive nitroglycerine in any form
Precautions:
Use caution in patients with Right Ventricular Infarct patterns.
Adverse Reactions
Transient headache
Postural syncope
Hypotension
Nausea and vomiting
Flushing
Dizziness
Burning under the tongue
Dosage and Administration
• Continue Nitroglycerin drip at the rate begun at the transferring hospital
• Refer to dosing chart below based on 25mg or 50mg Nitro in 250ml solution.
• Be advised that varying concentrations for Ntiroglycerin exist, please refer
to facility specific concentration guidelines
• Typical dosing starts a 5-10mcg/min (typically 3-6ml/hr)
• Typical titration increases or decreases in 5-10mcg increments q 5-10 minutes
titrated to cessation of pain and Systolic BP >90
Return to Table of Contents
Protocol
1. For inter-facility transport only when initiated by a sending facility.
2. Nitro infusions must be maintained on an IV pump at all times during transport.
3. Blood Pressure Monitoring must be maintained on q 5-10 minute intervals
depending on stability of patient. (q 5 when titrating, q 10 if stable)
4. Maintain continuous EKG and Pulse Oximetry monitoring
5. Nitro Dosage may be titrated downward in 5mcg increments at 5-10 minute
intervals to maintain systolic BP >90 or according to facility specific transfer
orders.
6. If systolic BP drops below 90 a 250ml fluid challenge of NS should be given in
addition to lowering titration.
7. If systolic remains below 90 after 250ml fluid challenge and decreasing titration,
Nitro drip should be stopped and medical control contacted for further
instructions.
8. Maximum drip rate should not exceed 200mcg/min
9. Nitroglycerin requires non-polyvinyl tubing and glass or maxide IV bag as Nitro
bonds to certain plastics which can alter dosing accuracy.
Nitro Concentration
25mg/250ml
5mcg
10mcg
15mcg
20mcg
25mcg
30mcg
35mcg
40mcg
45mcg
50mcg
55mcg
Ml per Hour
3ml
6ml
9ml
12ml
15ml
18ml
21ml
24ml
27ml
30ml
33ml
Return to Table of Contents
Nitro Concentration
50mg/250ml
5mcg
10mcg
15mcg
20mcg
25mcg
30mcg
35mcg
40mcg
45mcg
50mcg
55mcg
ML per Hour
1.5ml
3ml
4.5ml
6ml
7.5ml
9ml
10.5ml
12ml
13.5ml
15ml
16.5ml
BANDAGING
Indications
A. To stop external bleeding by application of direct and continuous pressure to
wound site
B. To protect patient from contamination to lacerations, abrasions, burns
Precautions
A. Although external skin wounds may be dramatic, they are rarely a high
management priority in the trauma victim.
B. Do not use circumferential dressings around neck. Continued swelling may block
airway.
Technique
A.
B.
C.
D.
E.
F.
G.
H.
I.
J.
K.
Use BSI.
Control hemorrhage with direct pressure, using sterile dressing.
Assess patient fully and treat all injuries by priority once assessment is complete.
Remove gross dirt and contamination from wound: clothing (if easily removable),
dirt, gasoline, acids, or alkalis. Use copious irrigating saline or tap water for
chemical contamination.
Evaluate wound for depth, presence of fracture in wound, foreign body, or
evidence of injury to deep structures. Note distal motor, sensory, and circulatory
function prior to applying dressings.
Apply sterile dressing to wound surface. Touch outer side of dressing only.
Wrap dressing with clean gauze or cloth bandages applied just tightly enough to
hold dressing securely (if no splint applied).
Assess wound for evidence of continued bleeding.
Check distal pulses, color, capillary refill, and sensation after bandage applied.
Continue to apply direct hand pressure over dressing, or use air splint if bleeding
not controlled with bandage alone.
For deep or gaping muscle wounds in which bleeding cannot be controlled with
direct pressure, pack the wound with sterile gauze than reapply a sterile dressing
with pressure.
Complications
A. Loss of distal circulation from bandage applied too tightly around extremity; for
this reason, do not use elastic bandages or apply bandages too tightly.
B. Airway obstruction due to tight neck bandages.
C. Restriction of breathing from circumferential chest wound splinting
D. Continued bleeding no longer visible under dressings. (This is particularly
common with scalp wounds that continue to lose large amounts of unnoticed
blood.)
E. Inadequate hemostasis: some wounds require continuous direct manual
pressure to stop bleeding.
Go to Table of Contents
AIRWAY MANAGEMENT
CAPNOGRAPHY
E. Indications
1. All intubated patients REQUIRE continuous end-tidal CO2 monitoring to assess:
a. Proper initial placement of the endotracheal tube and continued airway
patency.
b. Inadvertent displacement of the endotracheal tube.
c. Effectiveness of cardiopulmonary resuscitation
d. Patients requiring mechanical ventilation during transportation. The monitor is
used to determine if the endotracheal tube has become displaced or to detect
the disruption of the ventilator circuit
2. Patients receiving procedural sedation and analgesia (PSA) require continuous
monitoring for hypoventilation.
3. Patients with evidence of hypoventilation for any reason (pain management,
ingestion, seizure, CNS disorders, etc) should receive continuous end-tidal CO2
monitoring.
4. Patients with bronchospasm or CHF should receive continuous end-tidal CO2
monitoring.
F. Precautions
1. Caution should be exercised to ensure that the clinical picture matches the endtidal CO2 reading.
2. Determination of patient status should always involve a combination of end-tidal
CO2 readings, pulse oximetry readings and clinical signs.
G. Technique - End-tidal CO2 Monitor – Lifepak 12
1. Attach the CO2 sensor inline between the
endotracheal tube and
the BVM or mechanical
ventilator.
2. Open the CO2 tubing
connector door and
connect the Microstream
CO2 FilterLine tubing by
turning the tubing clockwise.
3.
4.
5.
6.
Press ON
Verify EtCO2 monitor display is on.
Display CO2 waveform on channel 2 or 3.
(Typically displayed on channel 3, although
shown here on channel 2)
7. Pridemark preselected lead group #2 is II, III,
CO2
Go to Table of Contents
H. Evaluate the capnograph waveform and numerical value.
1. It is important to evaluate both the numerical value (capnometry) and the
waveform (capnography). Evaluating the numerical value alone may lead to
erroneous interpretations. There are multiple sita etations i whichg the numerical
value isnor waveform isabnormca,e sgnifytinganh ore
ormcaity. .
Return to Table of Contents
Cardiac Output
EtCO2
(L)
(mmHg)
2
3
4
5
20
28
32
36
By monitoring the EtCO2 value during cardiopulmonary resuscitation,
efficacy of CPR in relation to cardiac output can be indirectly determined.
EtCO2 can be used as a feedback mechanism to optimize chest
compressions during CPR.
f.
If the shape of the capnogram appears abnormal it indicates an underlying
physiologic abnormal suggestive of different clinical pictures. The following
quick-reference with example waveforms can be used to help identify
underlying clinical disorders:
Bronchospasm
Bronchospasm with hypoventilation
Return to Table of Contents
CARDIOVERSION ALGORITHM (Patient is not in cardiac arrest)
Tachycardia:
With serious signs and symptoms related to the tachycardia
If ventricular rate is > 150 beats/min., prepare for IMMEDIATE CARDIOVERSION. May
give brief trial of medications based on specific arrhythmia algorithms. Immediate
cardioversion is generally not needed for rates < 150 beats/min.
Check
● Ensure adequate oxygenation
● Section Device
● IV Line
● Intubation equipment
Premedicate with midazolam whenever possible
Synchronized
Cardioversion
VT
PSVT
Atrial fibrillation
Atrial flutter
Adult Dose
100j, 200j
300j, 360j
Pediatric Dose
.05j/kg, 1.0j/kg
1.5j/kg, 2.0j/kg
Precautions
A. Precautions for defibrillation apply. Protect rescuers!
B. A patient who is talking to you is probably perfusing adequately.
C. If the defibrillator does not discharge on "synch" with tachycardia, turn off "synch"
button and refire. The waves may not have enough amplitude to trigger the
"synch" mechanism.
D. If sinus rhythm is achieved, even transiently, with cardioversion, subsequent
cardioversion at a higher energy setting will be of no additional value. Leave the
setting the same; consider correction of hypoxia, acidosis, etc. to hold the
conversion.
E. If the patient is pulseless, begin CPR and treat as cardiac arrest, even if the
electrical rhythm appears organized.
F. People with chronic atrial fibrillation are very difficult to convert, and their atrial
fibrillation is not usually the cause of their decompensation. If you get a history of
"irregular heartbeat," look elsewhere for the problem.
G. Sinus tachycardia rarely exceeds 150 beats/min. in adults (220 beats/min. in
children < 8 years old), and does not require cardioversion. Treat the underlying
cause.
Return to Table of Contents
H. Do not be overly concerned about the dysrhythmias that normally occur in the
few minutes following successful cardioversion. These usually respond to time
and adequate oxygenation, and should only be treated if they persist.
I. Biphasic monitors require different energy doses.
Return to Table of Contents
Combination Analgesia
A. Introduction
1. The appropriate management of anxiety, spasm and pain is an important
component of comprehensive emergency medical care.
2. The American College of Emergency Physicians state that proactively
addressing pain and anxiety will improve quality of care and patient satisfaction
by minimizing patient suffering.
3. Frequently it is necessary to combine a narcotic (analgesic) and a
benzodiazepine (anxiolytic) to provide adequate control of pain in combination
with anxiety and/or spasm.
4. Since combining a benzodiazepine and narcotic in the field is typically used for
treatment of pain in combination with anxiety and/or spasm and not to facilitate a
procedure the term Combination Analgesia will be used.
5. This protocol will address the use of combination narcotic and benzodiazepine
for combination analgesia. See Pain Management protocol for issues related to
patients who receive analgesia for pain management without sedatives.
Additionally, see Diazepam and Midazolam guidelines for treatment of anxiety
and spasm in the absence of pain.
6. Combination Analgesia describes a level of sedation that reduces the degree of
anxiety, spasm, pain or awareness a patient may experience during a pain illness
or injury. The patient retains their ability to maintain a patent airway
independently and continuously. They maintain their protective reflexes and their
ability to respond appropriately to physical stimulation and/or verbal command
and are easily aroused.
7. Combination Analgesia can only be performed by ALS providers who have met
the following requirements:
a. Completed training in the procedure and have met competency requirements
leading to certification.
b. Remain current through continuing education and semiannual skills checkoffs.
c. Only paramedics certified in combination analgesia can perform this
procedure.
B. Indication
Combination Analgesia is indicated for conditions that require pain management in
combination with anxiety and/or spasm management (i.e. shoulder / hip dislocations,
severe back spasms, etc).
I.
Precautions
1. Patients with cardiopulmonary disorders, multiple trauma, head trauma, or who
have ingested a central nervous system depressant such as alcohol are at
increased risk of complications from this procedure and require a high level of
vigilance.
2. Elderly patients (>65) tend to be more sensitive and therefore should always
receive the low end of the dose range. Administration should be slow and titration
with additional doses should be given with extreme care.
J. Technique
1. Equipment:
Go to Table of Contents
a.
b.
c.
d.
e.
f.
g.
h.
Cardiac monitor / defibrillator
Pulse oximeter
Capnography
Oxygen
Advanced airway management equipment
Suction equipment
IV Equipment
Reversal agent: Naloxone
K. Preparation:
a. Place the patient on a cardiac monitor.
b. Place the patient on oxygen
c. Place the patient on a pulse oximeter
d. Place the patient on capnography
e. Insert an intravenous line.
f. Make sure airway equipment, suction and reversal agent are available and
ready.
L. Pre-procedure assessment:
a. Complete an appropriate history and physical examination:
i. Focused exam of heart, lungs and airway evaluation
ii. Vital signs including oxygen saturation
iii. Level of consciousness / Mental status exam
iv. Pain Scale Evaluation
v. Determine patient’s NPO status:
(a) If patient has not been NPO for 6-8 hours for solids and 2-3 hours for
liquids, the risk of the procedure and necessary or anticipated benefit
of the procedure must be weighed.
vi. Obtain Consent:
(a) Inform the patient of the risks and benefits of using combination
analgesia.
(b) If the patient is able to give informed consent after being advised of
the risks and benefits document said consent in narrative.
M. Combination Analgesia Procedure:
The following parameters will be continuously monitored during Combination
Analgesia.
a. Responsiveness to commands
b. Capnography
c. Oxygen saturation
d. Heart rate
e. Respiratory rate
f. Blood pressure
g. Heart rhythm
h. Pain Scale Evaluation
N. Drug administration
1. A key to minimizing complications in Combination Analgesia is the slow titration
of drugs to the desired effect.
2. The combined use of opioids and benzodiazepines increases the risk of
respiratory depression
Return to Table of Contents
3. When both a benzodiazepine and an opioid are used, the opioid, which
possesses the greatest risk for respiratory depression, should be given first and
the benzodiazepine dose titrated.
4. Administer Fentanyl 0.5 – 1.0 mcg/kg IV over two minutes
5. Then administer Midazolam 1-2 mg IV over 2 minutes for anxiety or administer
Valium 1-5 mg IV over 2 minutes for spasm and/or anxiety.
6. Titrate additional drugs to desired effect:
7. If the patient needs additional sedation, use repeat doses of 1 mg IV Midazolam
or 1-2mg IV Valium.
8. If the patient needs additional pain control, use repeat doses of 0.5 – 1 mcg/kg IV
Fentanyl
9. Fentanyl, Midazolam & Diazepam should be given slowly. This may be
accomplished in several ways. (1) The appropriate dose may be diluted in a 10cc
syringe with normal saline and then push slowly over 2 minutes.
(2) The
appropriate dose may be placed in a 50cc bag of normal saline and administered
over 2 minutes via a microdrip administration set.
10. Carry-out procedure and/or transport with continuous monitoring
11. If patient has significant respiratory depression or hemodynamic instability,
consider reversal agent.
a. Reversal agents
vii. Naloxone - An agent used for reversal of narcotics (opioids). Duration of
action is approximately 30 minutes, which may be shorter than the clinical
effect of the agonist agent it is reversing. Use with caution. May
precipitate withdrawal in patients dependent on narcotic agents
viii. Dose: Administer 2 mg IV, Repeat as needed
O. Documentation
1. The procedure shall be documented in the patient care report
2. The opiod should be documented as administered for pain management
3. The benzodiazepine should be documented as administered for anxiety and/or
spasm management.
4. Each of these medications is given to treat a separate condition, the fact that
they are being used in combination only add’s to the risk of the the combination
therapy. Therefore, it is important to document the administration of these
medications for the individual purpose for which they were administered.
5. The following information should be documented in the PCR
a. Equipment Checklist
b. Pre-Procedure Assessment
c. History and Physical Examination
d. Reason for the use of combination analgesia
e. Vital Signs and Mental Status (before, during, and post administration)
f. Informed Consent
g. Medications used
h. Response to medications (Pain Scale Evaluation)
i. Any complications or side effects noted during combination analgesia
j. Patient condition when turned over to the receiving facility
P. Quality Management
1. An audit will be performed on any case in which the patient receives Combination
Analgesia
2. Any case where there is a complication from the procedure will be referred to the
Medical Director within 24 hours.
Return to Table of Contents
3. Any case that is noted to be out-of-protocol will be referred to the Medical
Director within 24 hours.
Q. Complications
1. Altered consciousness, sedation, dizziness and euphoria
2. Respiratory depression
3. Hypotension, bradycardia
4. Nausea and vomiting
5. Allergic reactions and anaphylaxis
6. Bronchospasm
Return to Table of Contents
Continuous Positive Airway Pressure (CPAP)
Indications
A. For consideration in moderate to severe respiratory distress secondary to
asthma/reactive airway disease, near drowning, COPD, CHF, acute pulmonary
edema or pneumonia who present with any of the following:
1. Pulse oximetry < 88% not improving with standard therapy.
2. ETCO2 > 50mmHg
3. Accessory muscle use / retractions
4. Respiratory rate > 25
5. Wheezes, rales, rhonchi
6. Signs of fatigue
Contraindications
A.
B.
C.
D.
E.
F.
G.
H.
I.
J.
K.
Age <12
Cardiac or respiratory arrest
Agonal respirations
Inability to maintain patent airway
Hypotensive, systolic BP (< 90mmHg)
Major trauma (face, neck, chest/abdomen, pneumothorax)
Nausea/vomiting
Inability to sit upright
Upper GI bleeding
Suspected pneumothorax
Unresponsive to speech, and/or unable to follow commands
Procedure
A.
B.
C.
D.
E.
F.
G.
H.
I.
Treat patients underlying condition according to appropriate protocol
Ensure full monitoring in place (EKG, SpO2 ) (ETCO2 if available)
Document breath sounds, ensure no signs or symptoms of pneumothorax
Document adequate BP (>90mmHg)
Have patient sitting up
Carefully explain procedure to patient
Place head strap over occipitoparietal area
Gently hold the delivery device to the patient’s mouth and nose
Attach the straps, loosely at first, gradually tightening as the patient tolerates.
Proceed with tightening the straps until air leaks are eliminated.
J. Progressively increase the pressure to a max of 10 cmH2O (see attached chart
for reference). There is better tolerance with gradual progression of pressure.
K. Repeat and record vital signs every 5min
Considerations and Special Notes
A. Success is highly dependent upon patient tolerance, and EMT-P ability to coach
1. Instruct patient to breath in through nose and exhale through mouth as long as
possible
B. Deterioration on CPAP ⇒ mechanical ventilation/intubation
1. Deterioration of mental status
2. Increase of the EtCO2
3. Decline of SpO2
Return to Table of Contents
4. Progressive fatigue
Monitor closely for development of pneumothorax and or hypotension
Patients should be closely monitored with SpO2, EKG, BP (ETCO2 if available)
Monitor patients closely for vomiting and or gastric distention
Inline nebulization may be used with CPAP and is required if the procedure is being
done to treat bronchospasm.
G. Chemical and physical restraints should never be used to facilitate this procedure
C.
D.
E.
F.
The following charts are for reference and represent flow rates and information
pertaining to the Boussignac CPAP System. They are guidelines only and other
devices necessitate following manufacturer and Medical Director guidelines.
The chart below gives the approximate CPAP/ PEEP in cmH2O based on the flow of O2.
Flow (LPM)
CPAP / PEEP (cmH2O)
10
15
20
25
> 25
2.5 - 3.0
4.5 - 5.0
7.0 - 8.0
8.5 - 10.0
> 10
Minutes of Oxygen by Cylinder Size
All based on full 2200 PSI Cylinders
Flow
(LPM)
D Cylinder
EMS Portable
E Cylinder
EMS Portable
M Cylinder
EMS Ambulances
5
6
8
10
12
15
20
25
70
58
44
35
29
23
16
14
123
102
77
61
51
41
29
23
703
598
498
374
299
199
175
140
Return to Table of Contents
FIELD DRAWN BLOOD SAMPLES
Indications
A. Patients receiving an IV in the field and who, in the judgment of the field
providers, will need blood tests in the emergency department
B. Patients receiving IV dextrose in the field
C. Patients that may have been exposed to carbon monoxide
Precautions
A. Use BSI.
B. Proper identification of the patient and the specimen(s) is mandatory.
C. Improper technique in obtaining the specimen will result in inaccurate or invalid
test results. This wastes critical time and defeats the purpose of drawing
specimens in the field.
Technique
A. After initiating an IV and removing the needle, attach the Vacutainer holder to the
hub of the IV catheter. (This is accomplished using the Luer adaptor attached to
the Vacutainer holder.)
B. Fill all the desired blood tubes in appropriate order per system requirements.
C. Tubes containing anticoagulant should be inverted gently back and forth at least
ten times to insure adequate mixing of blood with the substance in the tube. Do
not shake the tube as this could cause hemolysis, which could interfere with test
results.
D. The tubes should be placed in a small biohazard bag. The bag should be labeled
with the patient's name and time of draw, and taped to the patient's IV bag. The
tubes may also be handed directly to the nurse attending the patient.
Side Effects and Special Notes
A. Any discrepancy in identification must be reported immediately to the emergency
department charge nurse.
B. Pediatrics receiving an IV should have at least a speckled red tube and lavender
top tube drawn. The red top may be filled only halfway and the lavender only 1/4
of the way to do the needed tests. If available, red and lavender pediatric tubes
may be used.
C. The blue top tube must be filled exactly, according to the vacuum.
D. Blood samples should be drawn prior to the administration of IV fluid, in order to
provide a better and less dilute sample for potential “donor” patients.
Go to Table of Contents
IV
BLOOD DRAW FOR LAW ENFORCEMENT
Purpose
A. To meet all requirements of the Board of Health rules relating to chemical tests
for alcohol determination
Indications
A. Request of the law enforcement officer, and
B. Agency authorization
Precautions
A. Blood samples shall be collected only in an appropriate clinical or public safety
facility and in the presence of the officer.
B. In no event shall the collection of blood samples interfere with the provision of
essential medical care.
C. Do not use alcohol or phenolic solutions as a skin antiseptic.
Technique
A.
B.
C.
D.
E.
F.
G.
H.
I.
J.
K.
L.
M.
N.
O.
P.
Assure the patient’s consent to the procedure.
Utilize blood draw supplies provided by the law enforcement agency.
Use BSI.
Apply tourniquet proximal to the proposed site.
Scrub the insertion site with non-alcohol prep provided in blood draw kit.
Put on disposable medical gloves prior to venipuncture.
Hold vein in place by applying gentle traction on the vein distal to the point of
entry.
Puncture the skin and the vein with the bevel of the needle upward.
Once in the vein, collect the sample directly into the sterile blood tubes provided
by the officer.
Remove tourniquet.
Remove the needle from the vein and hold pressure to stop any bleeding.
Give the blood sample to the officer.
Sign any paper work required by the officer.
Ensure all seals and samples are labeled accurately and completely as failure to
do so can result in case dismissal and other legal complications
Obtain Officer’s name, Patient name, and if possible SSN and DOB and
document on the patient care report.
Dispose of contaminated needles appropriately.
Go to Table of Contents
PERCUTANEOUS CRICOTHYROTOMY
P
Introduction
A. Percutaneous cricothyrotomy is a difficult and hazardous procedure that is to be
used only in extraordinary circumstances as defined below. The reason for
performing this procedure must be documented and submitted for review to the
physician advisor or designee within 24 hours. Percutaneous cricothyrotomy is
to be performed only by paramedics trained in the procedure.
Indications
A. When a life threatening condition exists and advanced airway management is
indicated, and you are unable to establish airway by other means.
Precautions
A. Bleeding is possible, even with correct technique. Straying from the midline is
very dangerous and likely to cause hemorrhage from the carotid or jugular
vessels, or their branches.
Technique
A. Using aseptic technique (Betadine/alcohol wipes) cleanse the area.
B. Position the patient in a supine position, with in-line spinal immobilization if
indicated.
C. At this time the scalpel included with the kit may be used to make a ¼ inch
vertical incision through the skin, over the cricothyroid membrane.
D. Using the prepackaged set, insert the needle or over-the-needle-catheter through
the cricothyroid membrane in a caudal direction at a 45-degree angle.
E. If using an over-the-needle-catheter, remove the syringe and needle. Otherwise
remove the syringe.
F. Insert the guidewire through the catheter or needle.
G. Remove the catheter or needle over the wire.
H. Slide the dilator and tracheostomy tube onto the wire into the neck incision.
I. Push the dilator through the cricothyroid membrane with a twisting motion, and
insert the tracheostomy tube into the trachea.
J. Remove the dilator and wire, leaving the tracheostomy tube in place.
K. Ventilate with BVM and 100% oxygen.
L. Confirm tube placement is successful. (Chest rise and fall, breath sounds,
secondary confirmation device). Observe for subcutaneous air, indicating
tracheal injury or improper placement.
M. Secure tube with ties.
N. Transport to appropriate facility.
Go to Table of Contents
PNEUMATIC ANTI SHOCK GARMENT (PASG-formerly MAST)
Indications
The Denver Metropolitan EMS Medical Directors Group does not recommend the use of
this device in the field for the management of shock.
Go to Table of Contents
RESTRAINTS
Indications
A. Use of physical restraint on patients is permissible if the patient poses a danger
to himself or to others. Only reasonable force is allowable, i.e., the minimum
amount of force necessary to control the patient and prevent harm to the patient
or others. CONTACT BASE for physician direction if there is uncertainty as to
whether or not the use of restraints is warranted to transport the unwilling or
uncooperative patient.
B. Restraints are to be applied to patients only in limited circumstances:
1. A patient whose medical or mental condition warrants immediate ambulance
transport and who is exhibiting behavior that the prehospital provider feels
may or will endanger the patient or others
2. The prehospital provider reasonably believes the patient's life or health is in
danger and that delay in treatment and transport would further endanger the
patient's life or health, and there is no reasonable opportunity to obtain the
necessary consent to provide treatment or obtain informed refusal.
3. The patient is being transported under the direction of a mental health hold,
security hold, or police custody.
Precautions
A. Restraints shall be used only when necessary to prevent a patient from seriously
injuring themselves or others (including the ambulance crew), and only if safe
transportation and treatment of the patient cannot be done without restraints.
They may not be used as punishment, or for the convenience of the crew.
B. Any attempt to restrain a patient involves risk to the patient and the prehospital
provider. Efforts to restrain a patient should only be done with adequate
assistance present.
C. Be sure to evaluate the patient adequately to determine the medical condition,
mental status and decisional capacity of the patient. The hostile, angry, unwilling
patient with decision-making capacity may refuse treatment.
D. Be sure that restraints are in good condition (will not break and will not injure the
patient).
E. Do not use "hobble" restraints and do not restrain patient in the prone position.
F. Ensure that patient has been searched for weapons.
Technique
A. Determine that the patient's medical or mental condition warrants ambulance
transport to the hospital and that the patient lacks decision-making capacity, or
there is basis for police custody or a mental health hold to be instituted.
B. Treat the patient with respect. Attempts to verbally calm the patient should be
done prior to the use of restraints. To the extent possible, explain what is being
done and why.
C. Have all equipment and personnel ready (restraints, suction, a means to
promptly remove restraints, and adequate number of personnel).
D. Use assistance such that, if possible, one rescuer handles each limb and one
manages the head or supervises the application of restraints.
E. Consider the patient's strength and range of motion in the need for and method
of applying restraints.
Go to Table of Contents
F. Apply restraints to the extent necessary to subdue the patient. Do not use
restraints to punish the patient.
G. After application of restraints, check all limbs for circulation. During the time that
a patient is in restraints, an assessment of the patient's condition including
assessment of the patients airway, circulation and vital signs shall be made at
least every fifteen minutes, but more frequently if conditions warrant.
H. During transport and pending the arrival at the hospital, the patient shall be kept
under constant supervision.
I. The run report shall include: attempts at verbal persuasion to calm patient;
description of the facts justifying use of restraints; the type of restraints; a
description of the steps taken to assure that the patient's needs, comfort and
safety were properly cared for; the condition of the patient during restraint,
including reevaluations during transport; and the condition of the patient on
arrival at the hospital.
J. Removal of restraints should be done with sufficient manpower and caution for
protection of the patient and healthcare providers.
K. Utilize police assistance if necessary and if possible.
L. Handcuffs or other "hard restraints" are not to be applied by prehospital
providers. If police apply handcuffs, the officer should be requested to stay with
the patient and ride in the ambulance during transport.
M. The use of chemical restraints is limited to the use of Haloperidol, Versed and
Benadryl. If used, cardiac monitoring and intravenous access should be
performed as soon as possible.
Complications
A. Aspiration can occur, particularly if the patient is supine. It is the responsibility of
the attendant to continually monitor the patient's airway.
B. Nerve injury can result from hard restraints.
C. Do not overlook the medical causes for combativeness, such as hypoxia,
hypoglycemia, stroke, hyperthermia, hypothermia, or drug ingestion.
P
D. Contraindications, precautions, and Special Considerations regarding the use of
chemical restraints are found in the appropriate drug protocol, i.e. Haloperidol.
Versed, and Benadryl
Return to Table of Contents
SPLINTING: AXIAL
Indications
A. Pain, swelling, or deformity of spine which may be due to fracture, dislocation, or
ligamentous instability.
B. Neurologic deficit that might be due to spine injury.
C. Prevention of neurologic deficit or further deficit in patients with suspected spine
injury or instability.
D. In all trauma victims who are unconscious or with impaired consciousness due to
head injury or drug ingestion, to protect against damage or further damage in
patients where injury to the spine cannot be ruled out by accurate exam or
history.
Precautions
A. All patients with significant head trauma should be immobilized because of the
potential for unrecognized coexistent neck trauma.
B. Perform and document complete neurologic exam prior to moving the patient.
Reassess and document finding after splinting is completed and after each set of
vital signs (i.e. – every 5 minutes for a critical patient and every 15 minutes for a
non-emergent patient).
Cervical Splinting Technique
A. Perform cervical splinting immediately following initial assessment (if indicated).
If necessary, use assistant to maintain cervical stabilization while completing
initial assessment.
B. Use two people to apply splint if at all possible.
C. Do not use excessive force to straighten. Gently restore normal alignment.
D. Advise patient of procedure and purpose before and during application.
E. Immobilize the cervical spine with a semi-rigid collar of appropriate size for age.
F. Pad behind head in adults to maintain an anatomically neutral position.
G. Use long/short spine board or orthopedic scoop to support patient as situation
dictates.
H. Use tape and/or straps to secure patient effectively and allow turning as a unit for
airway control.
I. Continue to monitor airway and effectiveness of immobilization.
J. Board with an appropriate size collar is preferred to KED in pediatric patients.
Spine Immobilization Technique
A. Splint cervical spine concurrent with the initial assessment. Document neurologic
findings.
B. Complete detailed assessment and splint fractures prior to movement of patient
when possible.
C. Document neurologic findings.
D. In a sitting patient, use short board or Kendrick Extrication Device (KED) may be
beneficial for extrication:
1. Slide short board or KED behind patient.
2. Apply thigh straps snugly as close to groin as possible.
3. Apply shoulder or chest straps.
4. Use padding as needed to keep neck (in cervical collar) in a neutral position.
Go to Table of Contents
a. For pediatrics, use padding as needed to prevent misalignment.
5. Secure head to board.
E. Use long backboard or full body vacuum splint for supine patients.
1. For sitting patients, after short board or KED is applied:
a. Logroll or lift patient as a unit to board. Apply continuous cervical
stabilization during movement. One person should protect neck in collar.
Do not use force to straighten spine.
b. Release leg straps if short board or KED was used.
c. Use padding as needed behind knees to support a neutral axis under
small of back, neck and knees.
d. Use towel rolls or commercially available cervical immobilization device
and tape to secure neck immobilization.
e. Apply straps or tape to secure chest, thighs, and lower legs to allow
turning as a unit in case of vomiting or airway difficulty.
F. Reassess patient status, particularly airway and neurologic findings frequently.
Complications
A. Vomiting is common in head/spine-injured patients. Your splinting must be good
enough to allow turning of the patient for airway protection but must not impede
breathing efforts.
B. It is easy to miss injuries below the level of a neurological deficit. Look carefully
for abdominal and chest injuries, pelvic fractures, and extremity injuries without
symptoms. With loss of sensation below T-8, there will be no guarding, rebound
pain, or tenderness to alert you to internal abdominal injuries.
C. Pelvis fractures are difficult to diagnose in the field. Suspected pelvis injury can
be immobilized by use of the long board during spine immobilization with a
circumferential “pelvic wrap” or by use of a full body vacuum splint.
Side Effects and Special Notes
A. Patients with helmets and shoulder pads (Football, Lacrosse, Hockey)
1. When immobilization is indicated for football players with shoulder pads and
helmets, it should be accomplished with the helmet and pads in place.
2. The only indications for removal of a football helmet during immobilization
are:
a. Airway management cannot be accomplished without removal.
b. Bleeding cannot be controlled without removal.
c. The helmet does not provide adequate control of the head.
3. If the helmet is removed, the provider(s) should ensure adequate padding is
in place behind the head to allow for neutral alignment.
4. If the patient is immobilized with helmet and pads in place, the
facemask/shield must be removed prior to transport.
5. Lacrosse and hockey shoulder pads may not provide enough padding to
prevent hyperflexion. The helmet may need to be removed and head padded
or padding may be placed under the shoulders to accomplish neutral
alignment.
6. EMS responders should utilize the tools and expertise that the athletic
trainers at the scene can provide.
7. A “flat lift” with the backboard introduced from the patients feet is preferred to
a standard roll when the patient has shoulder pads.
8. It is recommended that EMS practice these procedures and become familiar
with athletic training staff tools and policies frequently.
Return to Table of Contents
9. As always, neurologic exam must be done and documented reflecting status
before and after the procedure.
B. Patient with motorcycle, ATV, racing helmets
1. Patients with these types of helmets should usually have them removed early
in the assessment to allow immediate access to the airway, face and
posterior skull.
2. Two providers are required to perform this procedure. One to control the
head and maintain in-line stabilization and one to manipulate and remove the
helmet.
3. As always, neurologic exam must be done and documented reflecting status
before and after the procedure.
C. Axial immobilization should be initiated any time it is indicated. However, the
procedure is not without complications. Research indicates that axial
immobilization may cause back pain, muscle spasm, pressure sores,
claustrophobia or restricted breathing efforts. As such, routine prophylactic axial
immobilization may not be indicated in a patient who meets all the following
criteria:
1. Is conscious, awake, and oriented to person, place and time (Glasgow Coma
Score = 15) and has no pre-existing mental impairment which might hinder
cognitive function (i.e. psychological disorder or mental retardation) and does
not complain of neck pain.
2. No language barrier exists which might hinder the assessment process.
3. Did not experience a loss of consciousness (either documented or
suspected).
4. The mechanism of injury does not warrant activation of a trauma team.
5. Upon physical exam, there is no evidence of tenderness, deformity, or spasm
in the neck, back or paraspinal region.
6. There is no evidence of peripheral sensory or motor deficit or impairment (i.e.
paresthesia, “peripheral tingling”, or decreased motor function following
incident).
7. There are no complaints or evidence of visual disturbances such as diplopia
or blurred vision.
8. There is no evidence of an unstable or staggered gait.
9. There is no evidence that suggests the use of prescribed CNS depressants,
analgesics, ETOH, or other mind-altering substances.
10. The patient has no pre-existing neck, back or neurologic injury.
11. There are no distracting injuries present which might mask an underlying
neurologic or spinal injury.
12. Once a patient has been immobilized by a first responder, the patient may not
have a cervical collar or other immobilization device removed by subsequent
responders. Patient must be transported to a healthcare facility. CONTACT
BASE if questions and/or clearance is desired.
See Also Protocol: Selective C-spine Immobilization
Return to Table of Contents
SPLINTING: EXTREMITY
Indications
A. Pain, tenderness, swelling, or deformity in extremity which may be due to fracture
or dislocation
B. In an unstable extremity injury: to reduce pain; limit bleeding at the site of injury;
and prevent further injury to soft tissues, blood vessels or nerves
Precautions
A. Critically injured trauma victims should not be delayed in transport by lengthy
evaluation of possible non-critical extremity injuries. Prevention of further
damage may be accomplished by securing the patient to a spine board when
other injuries demand prompt hospital treatment.
B. The patient with altered level of consciousness from head injury or drug/alcohol
influences should be carefully examined and conservatively treated, because his
ability to recognize pain and injury is impaired.
C. Make sure the obvious injury is also the only one. It is particularly easy to miss
fractures proximal to the most visible one.
D. In a stable patient where no environmental hazard exists, splinting should be
done prior to moving the patient.
Extremity Splinting Technique
A. Check pulse and sensation distally prior to movement or splinting.
B. Remove bracelets, watches, or other constricting bands prior to splint application.
C. Identify and dress open wounds. Note wounds that contain exposed bone or are
near fracture sites and may communicate with a fracture.
D. To minimize pain and soft tissue damage, avoid sudden or unnecessary
movement of fracture site.
E. Choose splint to immobilize joint above and below injury. Pad rigid splints to
prevent pressure injury to extremity.
F. Apply gentle continuous traction to extremity and support to fracture site during
splinting operation.
G. Reduce angulated fractures (if no pulses), including open fractures, with gentle
axial traction as needed to immobilize properly.
H. Check distal pulses and sensation after reduction splinting. Realign gently if
adequate circulation and sensation is lost.
Traction Splinting Technique (for suspected femur fractures):
A. Use two persons for splint application procedure.
B. Remove sock and shoe and check for distal pulse and sensation (unless you
cannot protect exposed foot from weather; then just ask patient about sensation
and observe movement).
C. Identify and dress open wounds, and note exposed bone or wounds overlying
fractures and potential communicating wounds.
D. Measure splint length prior to application.
E. Apply gentle axial traction with support to calf and fracture site, reducing
angulation of open fractures as necessary for secure traction.
Go to Table of Contents
F. Position ischial pad under buttocks, up against bony prominence (ischial
tuberosity). Empty pockets if necessary for patient comfort and appropriate
splinting.
G. Secure groin strap carefully.
H. Maintain continuous traction and support to fracture site throughout procedure.
I. Adjust support straps to appropriate positions under leg.
J. Apply ankle hitch and tighten traction until patient experiences improved comfort.
(Movement at the fracture site will cause some pain, but if traction continues to
cause increased pain, do not proceed. Splint and support leg in position of most
comfort.)
K. Secure support straps after traction properly adjusted.
L. Recheck distal pulses and sensation.
Complications
A.
B.
C.
D.
Circulatory compromise from excessive constriction of limb
Continued bleeding not visible under splint
Pressure damage to skin and nerves from inadequate padding
Delayed treatment of life-threatening injuries due to prolonged splinting
procedures
Side Effects and Special Notes
A. Traction splints should only be used if the leg can be straightened easily and
patient is comfortable with the traction device on. Particularly with injuries about
the hip and knee, forced application of traction device can cause increased pain
and damage. If this occurs, do not use traction device, but support in position of
most comfort and best neurovascular status.
B. When in doubt and the patient is stable, splint. Do not be deceived by absence
of deformity or disability. Fractured limbs often retain some ability to function.
C. Splinting body parts together can be a very effective way of immobilizing: arm-totrunk or leg-to-leg. Padding will increase comfort. This method can be very
useful in children when traction devices and pre-made splints do not fit.
IN
D. Consider pain management prior to splinting as needed.
Return to Table of Contents
P
TENSION PNEUMOTHORAX DECOMPRESSION
Indications
A. Tension pneumothorax is rare, but when present may rapidly lead to death and
must be treated promptly.
B. Nontension pneumothorax is relatively common, is not immediately life
threatening, and should not be treated in the field.
C. Treatment of tension pneumothorax is not difficult, although complications of the
procedure can be severe, but diagnosis must be accurate and is not always
easy.
D. The following signs are significant. Signs of pneumothorax as well as signs of
tension must be present before treatment is undertaken:
1. Simple Pneumothorax:
a. Respiratory distress - mild to severe
b. Chest pain
c. Decreased or absent breath sounds on affected side to auscultation of
chest
d. Subcutaneous crepitation, and
2. Signs of Tension:
a. Progressive respiratory distress (severe)
b. Tympanitic percussion note on affected side
c. Hyperexpanded chest on affected side
d. Tracheal shift away from affected side
e. Distended neck veins
f. Shock – low BP
g. If patient is intubated, increasing difficulty in bagging
Precautions
A. Accurate diagnosis is paramount. Note that simple pneumothorax has one set of
signs and tension pneumothorax has an additional set of signs.
B. Tension pneumothorax is a rare condition, but can occur both with trauma and
spontaneously. It can also occur as a complication of CPR.
Technique
A. Decompress using one of the following techniques:
1. Needle:
a. Expose entire chest. Clean chest vigorously with alcohol, Betadine, or
soap.
b. Insert an angiocath (14g or larger in adult; 18g in children) with syringe
attached, in the 4th or 5th intercostal space, midaxillary line (horizontal
"nipple line" in children). Alternatively, the angiocath may be inserted
between the 2nd and 3rd intercostal space, midclavicular line.
c. Hit the rib, then slide above it.
d. If air is under tension, barrel will pull easily and "pop" out the back.
Remove syringe, advance catheter and remove needle.
e. Only one attempt to be done per side.
Complications
A. Complications include:
Go to Table of Contents
1. Creation of pneumothorax if none existed previously
2. Laceration of lung
3. Laceration of blood vessels: slide above rib (intercostal vessels run in grove
under each rib)
4. Severe pain: if you're doing this in the field, patient should be sick enough
not to require anesthesia, but they'll let you know when you go through
pleura. Don't let that deter you - move briskly on.
5. Infection: clean rapidly but vigorously. Use sterile gloves, if possible.
Side Effects and Special Notes
A. Sudden onset of chest pain and shortness of breath in a normal individual may
also be caused by a pneumothorax (particularly in patients with COPD or
asthma). These can also progress to a "tension" state.
B. Tension pneumothorax can be precipitated by occlusion of an open chest wound
with a dressing. If, after dressing an open chest wound, the patient deteriorates,
remove the dressing.
Return to Table of Contents
P
TRANSCUTANEOUS CARDIAC PACING
Indications
A. Use cardiac pacing only when there is insufficient cardiac rate to maintain
adequate perfusion, and rate is unaffected by atropine and adequate oxygen and
ventilation.
B. Symptomatic bradyarrhythmias (includes A-V block)
C. P.E.A. (Pulseless Electrical Activity) with bradycardia
D. Patients who convert from a viable rhythm into asystole
Precautions
A.
B.
C.
D.
Capture can be difficult in some patients.
Patient may experience discomfort; consider midazolam.
Use the same precautions as with defibrillation.
Patients in atrial fibrillation may require higher energy settings for capture than
others.
Technique
A. Apply electrodes as per manufacturer specifications: (-) left anterior, (+) left
posterior.
B. Turn pacer unit on.
C. Select pacing rate at 80 beats per minute (BPM)
D. If the patient is awake, consider the use of sedation
E. Start pacing unit.
F. Confirm that pacer senses intrinsic cardiac activity by adjusting ECG size. If not,
pacer may discharge on an existing complex.
G. Set initial current to 40 mAmps.
H. Increase current 10 mAmps every 10-15 seconds until capture or 200 mAmps
(usually captures around 100 mAmps).
I. If there is capture, check for pulses.
J. If there are no pulses with capture, consider a fluid challenge or dopamine.
K. If no capture occurs with maximum output, discontinue pacing and resume
ACLS.
Complications
A. Ventricular fibrillation and ventricular tachycardia are rare complications, but
follow appropriate protocols if either occur.
B. Pacing is rarely indicated in patients under the age of 12 years.
C. Muscle tremors may complicate evaluation of pulses.
D. Pacing may cause diaphragmatic stimulation.
E. CPR is safe during pacing. A mild shock may be felt if direct active electrode
contact is made.
Go to Table of Contents
TRANSPORT OF THE HANDCUFFED PATIENT
Indications
The patient is being transported under police custody and has already been placed in
handcuffs by a police officer.
Precautions
Any attempt to restrain a patient involves risks to the patient and the prehospital
provider. Efforts to restrain a patient should only be done with adequate assistance
present.
At no time should the patient be placed in a prone position for a prolonged time at the
scene or during transport to the hospital.
Ensure that patient has been searched for weapons.
Technique
A. For the patient who does not require spinal immobilization or transport in a
supine position:
1. Maintain restraint via the handcuffs.
2. Escort the patient to the bench seat inside the ambulance.
3. Secure the patient in a sitting position with the seat belt.
4. Treatment and transport should be done with the patient remaining in the
handcuffs.
5. Request that the officer stay with the patient and ride in the ambulance during
transport. Ultimately, we are not responsible for the hold on this patient.
B. For the patient who requires transport with spinal immobilization or in a supine
position and is found in standing or sitting position:
1. Ensure that you have adequate assistance available to maintain restraint of
the patient.
2. Secure the patient's cervical spine with a cervical collar if indicated.
3. Assign one individual to support the patient's head.
4. Bring the stretcher, with backboard or scoop if indicated, to the patient.
5. Have the patient sit down on the stretcher and secure each arm with Kerlix
before having the officer remove the handcuffs.
6. Lie the patient down on the stretcher in a supine position.
7. Secure one arm of the patient to the scoop or backboard with the handcuffs.
If further restraint is required, use Kerlix or Velcro cuffs to restrain other
extremities.
C. For the patient who requires transport with spinal immobilization or in a supine
position and is found in a prone position:
1. Ensure that you have adequate assistance available to maintain restraint of
the patient.
2. Secure the patient's cervical spine with a cervical collar if indicated.
3. Assign one individual to support the patient's head.
4. Secure each arm and both legs with Kerlix prior to having the officer remove
the handcuffs.
5. Roll the patient onto a backboard or scoop.
6. Place the stretcher next to the patient and lift the patient onto the stretcher.
Go to Table of Contents
7. Secure one arm of the patient to the scoop or backboard with handcuffs. If
further restraint is required, use Kerlix or Velcro cuffs to restrain other
extremities.
Note: If the patient remains combative after physical restraints, consider the use of
chemical restraint.
Return to Table of Contents
P
VASCULAR ACCESS DEVICES
Specific Information Needed:
A. Obtain pertinent medical history if possible.
B. Obtain any information possible regarding the type of Vascular Access Device
(VAD), number of lumens, purpose of the VAD, etc.
Indications
A. To obtain rapid venous access for the critical patient when peripheral access
cannot be obtained.
Precautions
A. Obtain information and assistance from family members or home health
professionals who are familiar with the device.
B. Discontinue any intermittent or continuous infusion pumps.
C. Assure placement and patency of the VAD prior to infusing any fluids or
medications.
D. Flush the catheter completely with sterile normal saline.
E. Use aseptic technique.
Central Venous Catheters or PICC Lines
A. Attempt peripheral or external jugular access first unless patient or patient's
family insist on the direct usage of VAD.
B. Identify the location and type of VAD (i.e. central venous catheter, peripheral
inserted central catheter).
C. Utilize knowledgeable family members, significant others or home visiting nurse if
available.
D. Discontinue and/or disconnect any pumps or medications.
E. Clamp the VAD closed to prevent air embolus.
F. If multiple lumen, identify the lumen to be used.
G. Utilize aseptic technique.
H. Briskly wipe the injection cap with an alcohol and/or povidone-iodine pad.
I. Insert the needle (attached to syringe) into the cap. Aspirate slowly for a positive
blood return. Obtain blood samples if necessary. Then flush the line with
solution.
J. Insert the needle (attached to a medication syringe or IV tubing) and infuse
medications or fluids.
K. Secure the IV tubing.
L. Reassess the infusion site.
M. Reassess patient condition.
Implanted Ports
A. Attempt peripheral or external jugular access first unless patient or patient's
family insist on the direct usage of the VAD.
B. Identify the location and type of VAD (e.g. implanted port).
C. Utilize knowledgeable family members, significant others or home visiting nurse if
available.
D. Discontinue and/or disconnect any pumps or medications.
E. Carefully palpate the location of the implanted port.
Go to Table of Contents
F. If multiple ports, identify the port to be used.
G. Using sterile technique, prep the site with alcohol and/or povidone-iodine pad.
Wipe from the center outward three times in a circular motion.
H. Using a sterile gloved hand, press the skin firmly around the edges of the port.
I. Using a syringe filled with solution, insert the needle perpendicular to the skin.
J. Aspirate slowly for blood return, then flush the port prior to infusion. When
aspirating blood from a VAD, use a syringe that is 10cc or less to avoid
complications.
K. Secure the IV tubing.
L. Reassess the infusion site.
M. Reassess the patient.
Complications
A. Patients with VADs are very susceptible to site infection or sepsis. Use sterile
techniques at all times.
B. Sluggish flow or no flow may indicate a thrombosis. If a thrombosis is suspected,
do not utilize the lumen.
C. Rarely, a catheter will migrate. The symptoms may include the following:
1. burning with infusion
2. site bleeding
3. shortness of breath
4. chest pain
5. tachycardia
6. hypotension
D. If a catheter migration is suspected, do not use the VAD and treat the patient
according to symptoms.
E. Catheters are durable but may leak or be torn. Extravasation of fluids or
medications occurs and may cause burning and tissue damage. Clamp the
catheter and do not use.
F. Air embolism may occur if the VAD is not clamped in between infusions. Avoid
this by properly clamping the catheter and preventing air from entering the
system.
Return to Table of Contents
IV
VENOUS ACCESS TECHNIQUE - GENERAL PRINCIPLES
Indications
A. Administer fluids for volume expansion
B. Administer drugs
Precautions
A. Do not start IVs distal to a fracture site or through skin damage with more than
erythema or superficial abrasion.
B. Due to the uncontrolled environment in which prehospital IVs are started, take
extra care to use sterile technique.
C. Due to the high complication rate associated with prehospital IV therapy, use
good judgment when deciding which patients should receive an IV.
Technique
A.
B.
C.
D.
Connect tubing to IV solution bag.
Fill drip chamber one-half full by squeezing.
Tear sufficient tape to anchor IV in place.
Use BSI.
E. For pediatric patients consider applying an arm board or splint prior to
venipuncture.
F. Scrub insertion site with alcohol or iodine pads.
G. Don't palpate, unless necessary, after prep.
H. Perform venipuncture or enter bone marrow as described in the specific
techniques described in this protocol.
I. After the catheter is in place, remove the needle or stylette, draw bloods when
possible and connect tubing.
J. Open full to check flow and placement, then slow to TKO rate unless otherwise
indicated or ordered.
K. Secure tubing with tape, making sure of at least one 180-degree turn in the
tubing when taping to be sure any traction on the tubing is not transmitted to the
cannula itself.
L. Anchor with arm board or splint as needed to minimize chance of losing line with
movement.
M. Recheck to be sure IV rate is as desired.
Complications
A. Pyrogenic reactions due to contaminated fluids become evident in about 30 min
after starting the IV. Patient will develop fever, chills, nausea, vomiting,
headache, backache, or general malaise. If observed, stop and remove IV
immediately. Save the solution so it may be cultured.
B. Local: hematoma formation, infection, thrombosis, phlebitis. Note: the
incidence of phlebitis is particularly high in the leg. Avoid use of lower extremity
if possible.
C. Systemic: sepsis, pulmonary embolus, catheter fragment embolus, fiber
embolus from solution in IV
Go to Table of Contents
Side Effects and Special Notes
A. Antecubital veins are useful access sites for patients in shock, but if possible,
avoid areas near joints (or splint well!).
B. The point between the junction of two veins is more stable and often easier to
use.
C. Start distally, and if successive attempts are necessary, you will be able to make
more proximal attempts on the same vein without extravasating IV fluid.
D. Venipuncture has little morbidity; however, the excess fluids inadvertently run in
when nobody is watching can be fatal!
E. The most difficult problem associated with IV insertion is knowing when to try and
when to stop trying. Valuable time is often wasted attempting IVs when a critical
patient requires blood. IV solutions may "buy time," but they frequently lose time
instead. In critical patients do not delay transport while attempting IV insertion at
the scene. IVs may be placed en route.
F. For the purpose of this protocol, peripheral IV will be defined as extremity or
external jugular vein.
Return to Table of Contents
IV
VENOUS ACCESS TECHNIQUE - SALINE LOCK (Buff Cap)
Indications
A. Prophylactic IV access
B. Drug administration
Precautions
A. Consider the patient, and whether a running IV or a buff cap is needed.
B. For any buff cap established in the prehospital setting, the attendant is
responsible for showing the buff cap to the receiving nurse.
Technique
A.
B.
C.
D.
E.
Assemble the necessary equipment.
Prefill the saline lock with sodium chloride.
Proceed with the technique for extremity IVs.
Remove the needle from the catheter and insert the saline lock.
Flush the saline lock with 2-5 ml of sodium chloride.
Contraindications
A. Any catheter placed in the external jugular vein
B. Any patient who is in need of fluid or is hypotensive
C. The cardiac arrest patient
Go to Table of Contents
IN
P
VENOUS ACCESS TECHNIQUE - EXTERNAL JUGULAR VEIN
Indications
A. Inability to secure extremity IV access
Technique
A. Position the patient: supine, head down (this may not be necessary or desirable
if congestive heart failure or respiratory distress present). Turn patient's head
opposite side of procedure.
B. Align the cannula in the direction of the vein, with the point aimed toward the
ipsilateral shoulder (on the same side).
C. "Tourniquet" the vein lightly with one finger above the clavicle and apply traction
to the skin above the angle of the jaw.
D. Make puncture midway between the angle of the jaw and the midclavicular line,
"tourniqueting" the vein lightly with one finger above the clavicle.
E. Puncture the skin with the bevel of the needle upward; enter the vein either from
the side or from above.
F. Note blood return and advance the catheter over the needle and remove
tourniquet.
Go to Table of Contents
IV
VENOUS ACCESS TECHNIQUE - EXTREMITY
Technique
A. Apply tourniquet proximal to proposed site to venous return only.
B. Hold vein in place by applying gentle traction on vein distal to point of entry.
C. Puncture the skin (with the bevel of the needle upward) about 0.5 to 1 cm from
the vein and enter the vein either from the side or from above.
D. Note blood return and advance the catheter over the needle and remove
tourniquet.
Go to Table of Contents
IN
VENOUS ACCESS TECHNIQUE - INTRAOSSEOUS INFUSION
Indications (Must meet all criteria)
A. Rescue or primary vascular access device when peripheral IV access not
obtainable (see vascular access protocol)
B. Patient with critical illness. Critical illness is defined as:
1. Cardiopulmonary arrest
2. Impending arrest
3. Profound shock with hypotension (SBP<80) and poor perfusion
4. Utilization of IO access for all other patients requires base station contact
C. Adults IOs can be used in children age > 8 years old or weight > 40 kg
D. May be considered prior to peripheral IV attempts in patients without identifiable
peripheral vein
Technique
A. Site of choice – tibial plateau - one finger breadth below the tuberosity on the
anteromedial surface
B. Clean skin with povidone-iodine.
C. Place intraosseous needle perpendicular to the bone.
D. Follow manufacturer’s guidelines specific to the device being used for insertion.
E. Entrance into the bone marrow is indicated by a sudden loss of resistance.
F. Even if properly placed, the needle will not be secure. The needle must be
secured and the IV tubing taped. The IO needle should be stabilized at all times.
A person should be assigned to monitor the IV at the scene and en route to the
hospital.
G. Only one intraosseous attempt is to be done in each tibia.
H. Puncture site should be covered with a dressing and notify hospital staff of all
insertion sites/attempts.
Complications
A. Bone fracture (pushing too hard while not twisting the needle enough)
B. Infection
Contraindications
A.
B.
C.
D.
Fractures
Cellulitis
Osteogenesis imperfecta
Total knee replacement
Side Effects and Special Notes
A. Some authorities recommend aspiration of marrow fluid or tissue to confirm
needle location. This is not recommended for field procedures, as it
increases the risk of plugging the needle.
B. Expect flow rates to be slower than peripheral IV’s. Pressure bags may be
needed. Any drug or IV fluid may be infused.
C. Prior to IO insertion, consider rectal administration of benzodiazepines in patients
8 and under with status epilepticus. Consider IM midazolam for ages 9 and
above for patients in status epilepticus.
Go to Table of Contents
D. Some manufacturers recommend the use of lidocaine for the treatment of pain
associated with fluid administration. Check with your manufacturer and Medical
Director for further guidance.
Return to Table of Contents
PREHOSPITAL PATIENT ASSESSMENT
PATIENT ASSESSMENT ALGORITHM
Scene Size-Up
BSI
Unsafe Scene
Safe Scene
Control Scene
Move Patient
Correct Hazard
Initial Assessment
TRAUMA PATIENT
MEDICAL PATIENT
Focused History and
Physical Exam
Focused History and
Physical Exam
Evaluate Mechanism of
Injury (MOI)
Significant MOI
No Significant MOI
Rapid Trauma
Assessment
Focused Trauma
Assessment for Specific
Injury
Baseline Vital Signs
Baseline Vital Signs
SAMPLE History
Transport
Unresponsive
SAMPLE History
Rapid Medical
Assessment
Focused Medical
Assessment for specific
complaint
Baseline Vital Signs
Baseline Vital Signs
SAMPLE History
Transport
Transport
Components of Detailed
Exam
Detailed Physical Exam
SAMPLE History
Transport
Detailed Physical Exam
Components of Detailed
Physical Exam
Ongoing Assessment
Communication
Documentation
Go to Table of Contents
Responsive
SCENE SIZE UP
A. Recognize environmental hazards to rescuers, and secure area for treatment.
Implement body substance isolation (BSI).
B. Make sure you and your partner are safe. Also make sure the patient and
bystanders are safe. Move the patients and bystanders to safe area if needed.
C. Recognize hazard for patient, and protect from further injury.
D. Identify number of patients. Initiate a triage system if appropriate.
E. Observe position of patient, mechanism of injury, surroundings.
F. Identify self.
G. Initiate communications if hospital resources require mobilization; call for backup
if needed.
Go to Table of Contents
INITIAL ASSESSMENT
A. Form a general impression of the patient (sick/not sick; hurt/not hurt)
B. Determine the chief complaint/apparent life threats
C. Assess mental status (AVPU)
• A----Alert
• V----Responsive to verbal stimulus
• P----Responsive to painful stimulus
• U----Unresponsive
D. Briefly note body position and extremity movement.
E. Airway:
1. Observe the mouth and upper airway for air movement.
2. Open airway if needed: use head tilt chin lift in medical patients; chin lift
(without head tilt) or jaw thrust in trauma victims.
3. Protect cervical spine from movement in appropriate trauma victims. Use
assistant to provide continuous manual stabilization.
4. Look for evidence of upper airway problems, such as vomitus, bleeding, facial
trauma.
5. Clear upper airway of mechanical obstruction with finger sweep or suction, as
needed.
F. Breathing:
1. Expose chest and observe chest wall movement.
2. Note respiratory rate (qualitative), noise, and effort.
3. Auscultate for breath sounds.
4. Treat respiratory arrest with:
a. Pocket mask or bag-valve-mask for initial ventilatory control.
b. Check pulse and begin CPR if no pulse.
IN
c. Intubate after initial ventilation if necessary.
5. Assess for partial or complete obstruction.
6. If respiratory rate < 12/min or breathing appears inadequate:
a. Assist respirations with pocket mask or BVM; administer supplemental
oxygen.
IN
b. Consider tracheal intubation to secure airway if necessary.
c. Transport rapidly.
7. Observe skin color, mentation for signs of hypoxia.
8. Administer oxygen if signs of hypoxia
9. Look for life threatening respiratory problems and briefly stabilize:
a. Open or sucking chest wound: seal.
b. Large flail segment: stabilize.
c. Tension pneumothorax: transport rapidly and decompress chest.
G. Circulation:
1. Pulse
a. Palpate for pulse: radial pulse presence implies BP>80 systolic;
carotid or femoral pulse presence implies BP>60-70. If the patient is
pulseless and apneic, begin CPR
Go to Table of Contents
b. Note pulse quality (strong, weak) and general rate (slow, fast,
moderate).
c. Check capillary refill time in fingertips: 2 sec. is normal. Pediatric
patients only.
2. Major Bleeding
a. Control hemorrhage by direct pressure with clean dressing to wound.
(If needed, use elevation, pressure points; tourniquet if appropriate)
H. Identify Priority of Patients
1. If evidence of medical shock or severe hypovolemia, obtain baseline vital
signs immediately and begin treatment according to protocols: medical
and trauma.
Special notes
A. Initial assessment may take 30 seconds or less in a medical patient or victim of
minor trauma. In the severely traumatized patient, however, assessment and
treatment of life threatening injuries evaluated in the initial assessment may
require rapid intervention, with treatment and further assessment en route to the
hospital.
B. In the awake patient, the initial assessment may be completed by your initial
greeting to the patient. This may make it clear that the ABCs are stable and
emergency intervention is not required before completing assessment.
C. Neck should be immobilized and secured during airway assessment or
immediately following initial assessment if indicated.
D. Vital signs should be obtained during the focused and detailed assessment. If
immediate intervention for profound shock or hypoventilation is required, this may
need to be initiated before numerical vital signs are taken.
Return to Table of Contents
FOCUSED ASSESSMENT
MEDICAL
A focused medical assessment is done on all conscious medical patients. In awake
patients, this may consist only of identifying yourself and noting the patient’s
responsiveness and general appearance. The formal detailed assessment may not need
to be done on patients with a specific complaint, such as “chest pain”. Assessment must
be no less thorough, but it may be limited to the body systems that are pertinent to the
presenting problem.
Based on the information obtained from the initial assessment, perform either a rapid or
focused medical assessment, and a detailed exam.
Focused-Responsive
A. Assess history of present illness
• O---Onset
(When it first began?)
• P---Provocation
(What brings it on or makes it better or worse?)
• Q---Quality
(On scale of 1-10, rate the pain)
• R---Radiation
(Does pain go anywhere & where is the pain?)
• S---Severity
(Compare pain to before, is it worse or same?)
• T---Time
(How long does the pain last, how long did it last
before, what helped before for relief?)
B. Obtain SAMPLE Information:
• S---Signs and Symptoms, chief complaint
• A--- Allergies
• M---Medications
• P--- Pertinent Medical History
• L--- Last oral intake, Last menstrual period
• E--- Events leading to illness
C. Perform a focused Medical Assessment
1. Chief Compliant
2. Signs
3. Symptoms
D. Obtain baseline vital signs: blood pressure, pulse, respirations, skin temperature
and color.
E. Based on the exam findings, initiate proper intervention.
F. Make transport decision.
G. Perform detailed physical exam
H. Transport as soon as possible.
I. Perform Ongoing Assessment
Go to Table of Contents
History
History of Present Illness (HPI)
An essential part of history taking. A proper history can give the provider all the
essential information necessary to diagnose the problem.
Chief Complaint - This is what the patient tells you, in his/her own words, is wrong.
O-P-Q-R-S-T (need to know)
Onset
Provocation
Quality
Radiation
Severity
Time
R-O-A-D-Q-A-L (nice to know, helpful in chest pains)
Radiation
Onset
Aggravating/Alleviating Factors
Duration
Quality
Associated problems
Location
Types of Pain
Focal - Pain that is located in one area and does not travel or move.
Radiating - Pain that originates in one spot and travels away from the focal point.
Diffuse - Pain that can be localized.
S-A-M-P-L-E History
Signs and symptoms
Allergies
Medications
Past history
Last meal eaten
Events leading to incident
Vital Signs
There are four vital signs that are recorded in the field. They are:
Pulse (Heart Rate)
Respiratory Rate
Blood Pressure
Skin Condition
Go to Table of Contents
TRAUMA
A. Focused-No Significant
1. The Focused Assessment is performed on the Specific Injury Site.
2. As you inspect and palpate specific injury, look and feel for the following
examples of injuries or signs of injury:
• D---Deformity
• C---Contusions/Crepitation
• A---Abrasions
• P---Punctures/Penetrations/Paradoxical Movement
• B---Burns
• T---Tenderness
• L---Lacerations
• S---Swelling
3. Assess baseline vital signs: blood pressure, pulse, respirations, skin
temperature, and color
4. Assess SAMPLE history:
• S--- Signs and Symptoms, chief complaint
• A--- Allergies.
• M--- Medications
• P--- Pertinent past medical history
• L--- Last oral intake, last menstrual period
• E--- Events leading to injury, illness
5. Based on the exam findings, initiate proper intervention
6. Transport as soon as possible.
7. Perform Detailed Assessment
8. Perform Ongoing Assessment
Go to Table of Contents
RAPID ASSESSMENT
MEDICAL-Unresponsive
A. Perform a rapid assessment of the specific area of complaint
1. Position the patient to protect the airway
2. Assess the head
3. Assess the neck
4. Assess the chest
5. Assess the abdomen
6. Assess the pelvis
7. Assess the extremities
8. Assess the posterior body
B. Obtain baseline vital signs: blood pressure, pulse, respirations, skin temperature
and color
C. Obtain SAMPLE Information:
• S---Signs and Symptoms, chief complaint
• A---Allergies
• M---Medications
• P---Pertinent medical history
• L---Last oral intake, Last menstrual period
• E---Events leading to illness
D. Based on the exam findings, initiate proper interventions
E. Transport as soon as possible
F. Perform Detailed Assessment
G. Perform ongoing assessment
Go to Table of Contents
TRAUMA
A. Perform a rapid trauma assessment on patients with significant mechanism of
injury (MOI) to determine life-threatening injuries. The rapid trauma assessment
should be performed on responsive and unresponsive patients alike. An integral
part of this assessment is evaluation using the simple mnemonic "DCAP-BTLS".
For each area of the body, you should quickly look for Deformities, Contusions,
Abrasions, Punctures/Penetrations, Burns, Tenderness, Lacerations, and
Swelling. In the responsive patient, symptoms should be sought before and
during the trauma assessment.
1. Continue spinal immobilization.
2. Reconsider transport decision.
3. Assess mental status:
• A----Alert
• V----Verbal
• P----Painful
• U----Unresponsive
B. As you inspect and palpate, look and feel for the following examples of injuries or
signs of injury:
• D----Deformity
• C----Contusions/Crepitation
• A----Abrasions
• P----Punctures/Penetrations/Paradoxical Movement
• B----Burns
• T----Tenderness
• L----Lacerations
• S----Swelling
C. Assess the Head; inspect and palpate for injuries of signs of injury (DCAP BTLS)
D. Assess the Neck; inspect and palpate for injuries of signs of injury (DCAP BTLS)
E. Assess the Chest; inspect and palpate for inures of signs of injury (DCAP BTLS)
F. Assess the Abdomen; inspect and palpate for injuries of signs of injury (DCAP
BTLS)
G. Assess the Pelvis; inspect and palpate for injuries of signs of injury (DCAP BTLS)
H. Assess the Extremities; inspect and palpate for injuries of signs of injury (DCAP
BTLS)
I. Roll patient with spinal precautions and assess posterior body; inspect and
palpate for injuries or signs of injury (DCAP BTLS)
J. Assess baseline vital signs: Blood pressure, Pulse, Respirations, Skin
Temperature, and Color
K. Assess SAMPLE history:
• S---Signs and Symptoms, chief complaint
• A---Allergies
• M---Medications
• P---Pertinent Medical History
• L---Last oral intake, LMP
• E---Events leading to illness
L. Based on the exam findings, initiate proper intervention
M. Transport as soon as possible
N. Perform ongoing assessment
Go to Table of Contents
PEDIATRIC PATIENT ASSESSMENT
Children can be examined easily from head to toe, but lack of understanding by the
patient, poor cooperation, and fright often limit the ability to assess completely in the
field. Children often cannot verbalize what is bothering them, so it is important to do a
systematic survey which covers areas that the patient may not be able to tell you about.
Any observations about spontaneous movements of the patient and areas that the child
protects are very important. In the patient with a medical problem, the more limited set of
observations listed below should pick up potentially serious problems.
A. General
1. Level of alertness, eye contact, attention to surroundings.
2. Muscle tone: normal or increased, weak or flaccid.
3. Responsiveness to parents, caregivers; Is patient playful or irritable?
B. Head
1. Signs of Trauma
2. Fontanelle, if open: abnormal depression or bulging
C. Face
1. Pupils: size, symmetry, reaction to light.
2. Hydration: brightness of eyes; Is child making tears? Is mouth moist?
D. Neck: note stiffness
E. Chest
1. Note presence of stridor, retractions (depressions between ribs on
inspiration) or increased respiratory effort.
2. Ausculate the chest:
a. Breath sounds: symmetrical, rales or wheezing?
b. Heart: rate, rhythm
F. Abdomen: distension, rigidity, bruising, tenderness.
G. Extremities
a. Brachial Pulse
b. Signs of Trauma
c. Muscle tone: symmetry of movement
d. Skin temperature and color, capillary refill
e. Areas of tenderness, guarding or limited movement
H. Neurologic Exam
Go to Table of Contents
SPECIAL ASSESSMENT NOTES
A. Do not let the gathering of information distract from management of lifethreatening problems.
B. Appropriate questioning can provide valuable information while establishing
authority, competence, and rapport with patient. Questions should be objective
and should not “lead” the patient.
C. Two types of information are used to assess medical or trauma conditions.
Subjective information is related by the patient in taking a history, and describes
symptoms. The physical exam provides signs or objective information that may
or may not correlate with the patient’s symptoms.
D. In medical situations, history is commonly obtained before or during physical
assessment. In trauma cases, it may be simultaneous or following the detailed
assessment. An assistant is often used for gathering information from family or
bystanders.
E. In trauma cases, carefully examine all areas where the patient complains of pain,
but realize that the patient’s capacity to feel pain is usually limited to one or two
areas- even if more areas are injured! That is why a systematic survey is
important even in an awake patient.
F. Use bystanders to confirm information obtained from the patient and to provide
facts when the patient cannot. History from the scene is invaluable.
G. Over-the-counter medications including aspirin, homeopathic remedies, and
herbal supplements are frequently overlooked by patient and rescuer, but may be
important to emergency problems. Birth control pills are also frequently
overlooked so be sure to ask.
H. Confidentiality is mandatory. Patients are in need and vulnerable, they deserve
respect, kindness and discretion.
I. Complete legible documentation is critical to convey the information above.
J. Be systematic. If you jump from one obvious injury to another, the subtle injury
that is most dangerous to the patient is easily missed.
K. If the patient has any significant airway or circulatory deterioration, these
problems must be addressed immediately. Otherwise, complete the assessment
before you begin to address the problems that have been identified.
L. Obtain and record two or more sets of vital signs and neurologic observations. A
patient cannot be called “stable" without at least two sets of vital signs giving
similar normal readings. Serial vital signs are an important parameter of the
patient’s physiologic status. Vital signs should be repeated frequently, at least
every 15 minutes in stable patients and at least every 5 minutes in unstable
patients.
Return to Table of Contents
DETAILED ASSESSMENT
Detailed assessment is the systematic assessment of the entire patient. It should be
performed after:
a) Initial assessment
b) Stabilization and initial treatment of life threatening airway, breathing, or
circulatory difficulties
c) Cervical immobilization as needed
The purpose of the detailed assessment is to uncover problems which are not lifethreatening, but which could be injurious or could become life threatening to the patient.
A. Initial vital signs
B. Head and Face:
1. Observe for deformities, asymmetry, bleeding.
2. Palpate for deformities, tenderness, crepitation.
3. Recheck airway for potential obstruction: dentures, bleeding, loose or avulsed
teeth, vomitus, abnormal tooth position from mandible fracture, absent gag
reflex.
4. Eyes: pupils (equal or unequal, responsiveness to light), foreign bodies,
contact lenses
5. Nose: deformity, bleeding, discharge.
6. Ears: bleeding, discharge, bruising behind ears
C. Neck:
1. Recheck for deformity or tenderness if not already immobilized.
2. Observe for wounds, neck vein distention, use of neck muscles for
respiration, altered voice, and medical alert tags.
3. Palpate for crepitation, tracheal shift.
D. Chest:
1. Observe for wounds, chest wall movement, and accessory muscle use.
2. Palpate for tenderness, wounds, fractures, crepitation, unequal rise of chest.
3. Have patient take deep breath: observe for pain, symmetry, air leak from
wounds.
4. Auscultate chest for rales, wheezes, rhonchi, or decreased breath sounds.
E. Abdomen
1. Observe for wounds, bruising, distention.
2. Palpate all 4 quadrants for tenderness, rigidity.
3. Consider orthostatic vital signs for volume status.
F. Pelvis
1. Palpate and compress lateral pelvic rims, symphysis pubis, for tenderness or
instability.
G. Shoulders/Upper Extremities
1. Observe for angulation, protruding bone ends, symmetry.
2. Palpate for tenderness, crepitation.
3. Note distal pulses, color, medical alert tags.
4. Check sensation.
5. Test for weakness if no obvious fracture present (have patient squeeze your
hands).
6. If no obvious fracture, gently move arms to check overall function.
H. Lower Extremities
Go to Table of Contents
1.
2.
3.
4.
5.
I.
Observe for angulation, protruding bone ends, symmetry.
Palpate for tenderness, crepitation.
Note distal pulses, color.
Check sensation.
Test for weakness if no obvious fracture present (have patient push feet
against your hands and pull back against your hands).
6. If no obvious fracture, gently move legs to check overall function.
Back
1. Immobilize if any suspicion of back injury. To the extent immobilization
allows, palpate for wounds, fractures, tenderness.
2. Recheck motor and sensory function as appropriate.
Return to Table of Contents
ONGOING ASSESSMENT
A. Repeat initial assessment for a stable patient, repeat and record every 15
minutes. For an unstable patient, repeat and record at a minimum every 5
minutes.
1. Reassess mental status.
2. Maintain an open airway.
3. Monitor breathing for rate and quality.
4. Reassess pulse for rate and quality.
5. Monitor skin color and temperature.
6. Reassess and record vital signs.
B. Repeat focused assessment regarding patient complaint or injuries.
C. Check interventions:
1. Assure adequacy of oxygen delivery/artificial ventilation.
2. Assure management of bleeding.
3. Assure adequacy of other interventions.
Go to Table of Contents
NEUROLOGIC ASSESSMENT
Management of patients with head injury or neurologic illness depends on careful
assessment of neurologic function. Changes are particularly important. The first
observations of neurologic status in the field provide the basis for monitoring sequential
changes. Therefore, it is important that the first responder accurately observes and
records neurologic assessment, using measures which will be followed throughout the
patient's hospital course.
A. Vital Signs: observe particularly for adequacy of ventilations; depth, frequency,
and regularity of respirations.
B. Level of consciousness:
Glasgow Coma Score
1
Eye opening:
None
2
To pain
3
To speech
4
Spontaneously
1
Best verbal
None
2
response:
Garbled sounds
3
Inappropriate words
4
Disoriented sentences
5
Oriented
1
Best motor
None
2
response:
Abnormal extension
3
Abnormal flexion
4
Withdrawal to pain
5
Localizes pain
6
Obeys commands
Score = Sum of scores in 3 categories: (15 points possible)
C. Eyes:
1. Direction of gaze, extraocular movement.
2. Size and reactivity of pupils.
D. Movement: observe whether all four extremities move equally well.
E. Sensation (if patient awake): observe for absent, abnormal, or normal sensation
at different levels if cord injury is suspected.
Special Notes
A. The Glasgow Coma Scale (GCS) used above has gained acceptance as one
method of scoring and monitoring patients with head injury. It is readily learned,
has little observer to observer variability, and accurately reflects cerebral
function. Always record specific responses rather than just the score (sum of
observations). In areas where numerical assignment of scores is not a formal
procedure, the observations of the GCS still provide an excellent basis for field
neurologic assessment. Note also that the other parameters listed must be
observed to assess fully the neurologically impaired patient.
B. Use your written report to follow and document changes in neurologic findings.
C. At a minimum, gross motor function must be documented before and after
moving a patient with suspected spinal injury.
Go to Table of Contents
D. Sensory deficit levels should be marked gently on the patient's skin with a pen to
help identify any changes.
E. Note what stimulus is being used when recording responses. Applied noxious
stimuli must be adequate to the task but not excessive. Initial mild stimuli can
include light pinch, dull pinprick, or light sternal rub. If these are unsuccessful at
eliciting a pain response, pressure with a dull object to base of nailbed, stronger
pinch (particularly in axilla), or sternal rub will be necessary to demonstrate the
patient's best motor response.
F. When responses are not symmetrical, use motor response of the best side for
scoring GCS and note asymmetry as part of neurologic evaluation.
G. Use of restraints or intubation of patient will make some observations less
accurate. Be sure to note on chart if circumstances do not permit full verbal or
motor evaluation.
H. Remember that a patient who is totally without response will have a score
of 3, not 0.
I.
In small children, the GCS may be difficult or impossible to evaluate. Use an ageappropriate neurological assessment for small children. Children who are alert
and appropriate should focus their eyes and follow your actions, respond to
parents or caregivers, and use language and behavior appropriate to their age
level. In addition, they should have normal muscle tone and a normal cry.
Several observers should attempt to elicit a "best verbal response," to avoid over
or underestimation of level of consciousness.
Return to Table of Contents
PATIENT ASSESSMENT GUIDELINES
APPROACH TO DIFFICULT ASSESSMENTS
A. Background and Philosophy
1. Common difficulties that the care provider encounters are communication barriers. The
care provider frequently depends on effective communications in dealing with patient
evaluations and treatment.
2. Communication means more than the simple spoken word. Communication is the
collaboration of ideas between individuals based on body position, affect, gestures,
sounds, and sensory input. Communication occurs when the care provider palpates the
fractured extremity and the patient moans in response to pain. Communication occurs
when the care provider enters the patient’s residence and the patient’s body language
suggests hostility. Communication also occurs when the care provider asks a question
that evokes fear in the patient, creating a response of denial.
3. The Approach to Difficult Assessments Protocol separates the communication barrier
into five main categories, with suggestions to assist the care provider in overcoming
communication difficulties specific to each category. Suggestions have been separated
into “Reactive” strategies, which may be used by a care provider when confronted with a
current communication barrier, and “Proactive” strategies, which the care provider may
utilize to prepare for future potential communication barriers. The five communication
barrier categories are as follows:
a. Category 1: The patient’s language is foreign to the care provider (sign language,
foreign nationality, etc.):
Reactive troubleshooting techniques:
Quickly attempt to locate an interpreter. Bilingual family members are ideal.
Almost without exclusion, children can be very effective as interpreters.
Situations where there are no immediate family members or bystanders
are more challenging and require creativity on the part of the care
provider. Look for pictures of family members in the immediate vicinity,
point to the picture, and make a gesture of talking on the phone.
Pay close attention to gestures, sounds, and body language. Try to use
gestures similar to those of the patient in order to clarify meaning. The
care provider can generally obtain an idea of the nature of the complaint.
Consider using a pocket handbook for foreign language medical questions
(not highly recommended as the patient usually responds in a language
that you do not understand, causing further frustration). However, the
care provider can show patients a list of symptoms that are translated into
their primary language and have them point out their complaints. This
method may allow the care provider to develop a general impression of
the patient’s condition.
Proactive troubleshooting techniques:
Return to Table of Contents
Consider enrolling in language classes if there is a predominate language in
your response area that you know little about.
Attempt to discover different personnel in the company who know different
languages and utilize them as translational and educational resources.
There are telephone hotlines available in several areas that assist medical
personnel in interpretation of foreign languages. Care providers should
research their area for number listings of this type of hotline.
b. Category 2: The patient has experienced an acute impairment in his/her ability
to communicate or the patient has a chronic sensory deficit that hinders
communication (acute visual disturbances, acute hearing impairment, inability to
speak, etc.):
Reactive troubleshooting techniques:
Attempt to establish an alternative means of communication. For example,
the patient with Broca’s aphasia may not be able to speak to you, but can
understand what you are saying. Establish a hand-squeeze or an eyeblinking system of communication.
Be patient. Impairment to the patient’s normal means of communication can
be incredibly frustrating to the patient. Assuming that the patient cannot
understand what you say because they cannot respond is a false
assumption in many cases.
Proactive troubleshooting techniques:
The care provider should practice establishing alternative means of
communication with their fellow employee, family members, etc.
Research pathology that causes impairment of communication. For example,
understanding different types of aphasia may help in developing
alternative means of communication.
c. Category 3: There is a cognitive barrier between the patient and the care
provider that hinders communication (the patient does not understand your
terminology, etc.):
Reactive troubleshooting techniques:
Physically position yourself at a level equal to the patient. Your body position
alone can help you to communicate more effectively.
Attempt to use phrases that the patient will understand. For example, when
assessing the pediatric patient for mental status, the patient may
understand “Pokemon,” but may not understand “visual disturbance.”
The care provider should consider the use of props or objects that the patient
can understand.
Proactive troubleshooting techniques:
Return to Table of Contents
The care provider can prepare for interaction with patients by taking classes
on communication.
The care provider can expand on their skills in breaking down cognitive
barriers by teaching different topics to people with different levels of
understanding of, or experience with, the subject matter.
d. Category 4: There is an affective barrier between the patient and the care
provider that hinders communication (the patient is angry, upset, or frustrated
about your intrusion into his/her life, is distancing himself/herself from the care
provider, etc.):
Reactive Troubleshooting Techniques:
For the patient with a high need for control and/or authority: Avoid the
creation of conflict. Validate your patients’ input by repeating their
statements back to them. Validate your patients’ complaints—repeating
back their complaints establishes that you are listening to their concerns
and allows your patients to clarify any misinterpretation, adding to their
trust in you as their care provider. Utilize your partner’s input during
conflict. Attempt to get the patient’s family member/s to agree with you,
they can assist in convincing the patient of the need for treatment.
Attempt to identify and address the anxiety-causing agent.
For the patient that does not want to participate in assessment and/or
treatment: Positively reinforce participatory behavior that the patient
exhibits (your body language and dialog should reflect your appreciation
of the patient assisting you or cooperating with assessment and
treatment). Reassure the patient of your intentions. Attempt to find
common ground for initiating dialog (this should segue into dialog about
the patient’s condition). Do not perform procedures on patients without
telling them first—even if the procedure is necessary, the patient has the
right to refuse treatment.
For the patient with an adversarial attitude toward the care provider: Attempt
to find common ground with the patient. Identify and point out the similar
intentions that you share with the patient. This technique should be
performed in a discerning fashion because it can be perceived as
condescending. For example, if the patient tells you that he/she wishes to
harm him/herself and you tell the patient, “I understand that you are
hurting and I want to get you help as well,” the patient may assume your
response is condescending. Be careful to avoid adding your own
interpretation to the patient’s statements. By repeating patients’ words
back to them, you allow them to reflect and help to establish trust. As a
last resort, attempt to resolve the conflict by taking authority of the
situation (for example, with the hostile or violent patient).
e. Category 5: The patient is a poor historian, does not have a clearly defined
complaint, and/or continually sidetracks the dialog.
Troubleshooting techniques:
Return to Table of Contents
Establish a basic approach for every conscious patient. Consider the
following questions: “Why were emergency services activated? Why
were we called?”
If there is no clear reason given, consider “What is bothering you? What is
bothering you the most?” If no clear reason is given, consider “What is
different about right now compared to what is normal?”
If the care provider is still unable to establish a clearly defined complaint,
consider questioning the patient on a linear body systems approach.
Start with the head and make your way down through the rest of the body
systems until a complaint is established. Once a clearly defined
complaint is established, consider using that as a chief complaint until an
additional complaint arises.
The care provider needs to discern a careful balance between pressing the
patient for specific critical information and listening to the patient’s version
of their complaints and concerns. The patients that continually sidetrack
the dialog need to be given direction in the dialog. As the patient gives
you the information that you need, validate the patient by repeating that
information and carefully move the direction of the dialog to the next
question. If the care provider too quickly or forcefully directs the
conversation, trust may be broken and the sidetracking behavior may
increase.
B. Special Considerations
1. Although the Approach to Difficult Assessments Protocol is based on experience and
research, it should only be used as a guideline, not as a rule. There are many different
approaches to dealing with difficult assessment situations and there are many different
situations that are not practical to include in this protocol. Inevitably, the care provider
will have to incorporate the assessment tools that are most effective for him/herself when
approaching difficult patient assessments.
2. The fundamental key to mastering difficult patient assessment is awareness and
effectiveness in communication skills.
Return to Table of Contents
PATIENT CARE REPORT REQUIREMENTS
General Principles
A. The prehospital report is an integral component of patient care, quality
improvement and professional responsibility.
B. The prehospital report must be legible.
C. Vital information should also be immediately communicated to the Emergency
Department (ED) staff for efficient and safe transfer of care.
D. A legible copy of the prehospital report should be given to the ED staff at the time
of transport to the ED. If this is not possible, the report or a facsimile copy must
be received in the ED within 24 hours from the time of transport.
Procedure
A. All prehospital run reports must include the information noted in the EMS Division
policy statement.
B. Additional considerations and information to be included to the extent pertinent.
1. The physical examination should include assessment findings:
a. Head, Ears, Eyes, Nose and Throat (HEENT), including mentation, skin
color and condition, and trauma
b. Neck
c. Chest
d. Abdomen
e. Pelvis
f. Back
g. Extremities
h. Neurologic status
i. Cardiovascular status
j. Respiratory status
2. Treatment rendered should be detailed, including:
a. The reason or assessment findings that were the basis of the treatment,
procedure or medication
b. The effects (including lack of effect)
c. Treatment rendered prior to your arrival or by others
d. Medication administration should include time(s) and dose(s).
3. Facility contact information:
a. Name of physician and facility
b. Orders requested or denied
c. Time of contact
4. Additional documentation should be included, where pertinent to particular
protocols; for example:
a. Resuscitations in the field should document time and effects of all
procedures and medications, and time of pronouncement or termination
of resuscitation.
b. Refusals of transport should include documentation of mental status,
decision-making capacity, warnings given and condition of patient at
termination of contact.
c. Copies of EKG tracings should be affixed to copies of run reports left with
the hospital.
d. The mechanism of injury in trauma should be descriptive, not general.
Go to Table of Contents
5. The prehospital provider who authors the report must include his/her name
and signature on the report.
Return to Table of Contents
Pridemark Paramedic Services
Patient Care Report Requirement
A. Purpose
In addition to the specific requirements of the Denver Metro Protocols, Pridemark
Paramedic Services has a higher expectation of PCR (Patient Care Report) requirements.
These requirement are designed to assure smooth continuity of care. This Process shall
outline Pridemark specific requirements.
B. Process
1. A paper PCR shall be left at the receiving hospital facility for all patients
transported prior to departure from the unit. If utilizing electronic documentation,
this may be accomplished by syncing the completed PCR thus faxing it to the
unit.
2. In the event you are unable to leave a complete PCR either by electronic or
written means you shall complete and leave a PPCR (Preliminary Patient Care
Report) as approved by the Foothills RETAC or Draft Patient Care Report from
the TPCR Toughbook.
3. If you choose to leave a Draft PCR from the Toughbook, it must contain at a
minimum the same information the PPCR requires.
4. If leaving a PPCR or Draft be sure to keep a copy of that record for utilization
later when you complete your full report.
C. General Principles
1. The final and complete patient care report shall serve as the complete medical
record.
2. Draft or Preliminary reports are done to facilitate smooth continuity of care and
as a courtesy to the receiving facility. They may contain partial or incomplete
data.
3. These are provided at the request of the Foothills RETAC and participating
hospital facilities with the full knowledge that these are preliminary or draft
documents.
Go to Table of Contents
REQUIRED RECORDS ON TREATMENT AND TRANSPORTATION
Policy Statement of the Colorado Dept. of Health EMS Division:
REQUIRED RECORDS ON TREATMENT AND TRANSPORTATION
OF PATIENTS FOR PREHOSPITAL CARE EMS ORGANIZATIONS
Section 9.2 of the EMS Rules specifies that each ambulance service shall maintain
records of the treatment and transportation of all patients cared for. Such records shall
include all information determined by the Department of Health to be essential for the
maintenance of adequate minimum records on a patient's condition and medical care
provided. In addition, these records shall be preserved by the ambulance service for a
period of three (3) years.
In compliance with Section 9.2, the Emergency Medical Services Division of the
Department of Health has established the foregoing policy that specifies the essential
information to be recorded and preserved for each patient cared for by an ambulance
service.
The Emergency Medical Services Division of the Colorado Department of Health hereby
determines that the following information shall be recorded and preserved by each
Prehospital care EMS service in the State on each patient cared for:
A. Patient name, if known, as complete as possible and ideally including full first
and last name.
B. Patient residential address, if known, as complete as possible (to allow medical
or public health follow up, if needed).
C. Patient sex (both for purposes of identification and to facilitate diagnosis and
treatment).
D. Patient age, as accurate as possible (both for purposes of identification and to
facilitate diagnosis and treatment).
E. Patient location at time of response and apparent cause of the injury or nature of
illness (to assist in subsequent diagnosis and treatment).
F. Patient condition at time of response, including a preliminary assessment of the
patient based on vital signs, apparent symptoms, and known medical history.
G. Patient vital signs at time emergency medical care is begun, to include
respiratory rate, pulse rate, blood pressure, level of consciousness, and pupil
size and reaction to light. Subsequent vital signs shall be recorded at least every
15 minutes when either treatment or transport time exceed 15 minutes.
H. Known patient history related to the apparent illness or injury, including allergies
and medications. If it is determined that the patient is on medication of any kind,
the prescribing physician should be identified, if possible, so he/she may be
contacted for confirmation, consultation, or actual care of the patient.
I. Treatment rendered to the patient at the scene and during transport, in sufficient
detail to permit the receiving facility (i.e., hospital, clinic, etc.), physician advisor,
and any other reviewing physician or nurse to determine the nature and extent of
treatment rendered.
J. Patient's apparent condition upon delivery to the receiving facility, and any
pertinent comments regarding changes in the patient's condition during transport
(to assist the receiving physician in diagnosis and treatment).
Return to Table of Contents
K. Identity and location of the receiving facility and signature or other indication of
the physician or nurse receiving the patient and assuming responsibility for the
care of the patient.
L. Full name and level of training and certification or licensure of each member of
the EMS crew caring for the patient.
M. Times of dispatch and departure to the emergency scene, time of arrival at the
scene, time of departure from the scene, and time of arrival at the receiving
facility.
N. Indication of whether emergency lights and siren were used enroute to the scene
and/or during transport.
In all cases, a copy of the patient care report should be delivered to the receiving facility
along with the patient.
Return to Table of Contents
COMMONLY ACCEPTED ABBREVIATIONS FOR FIELD USE
a
AAA
A&O x
abd
AB
ABC
ACLS
adm
ALS
am
AMA
AMS
amp(s)
ant
asa
ASCVD
ASHD
asys
ATLS
A&P
a&p
≈
@
BBB
BCLS
BLS
bil
BM
BP
BS
BVM
c
C
Ca
Ca++
CABG
CAD
cath
CBC
cc
CC
CCU
CHF
CHI
circ
before
abdominal aortic aneurysm
alert and oriented times
abdomen
abortion
airway, breathing, circulation
Advanced Cardiac Life Support
admission
Advanced Life Support
morning
against medical advice
altered mental status
ampule(s)
anterior
aspirin
arteriosclerotic cardiovascular disease
arteriosclerotic heart disease
asystole
Advanced Trauma Life Support
anterior and posterior
auscultation and percussion
approximately
at
Bundle Branch Block
Basic Cardiac Life Support
Basic Life Support
bilateral
bowel movement
blood pressure
breath sounds
bag, valve, mask
with
Centigrade
cancer
calcium
coronary artery bypass graft(s)
coronary artery disease
catheter, catheterization
complete blood count
cubic centimeter
chief complaint
coronary care unit
congestive heart failure
closed head injury
circulation
Go to Table of Contents
cm
CMS
CNS
CO
c/o
centimeter
circulation, movement, sensation
central nervous system
carbon monoxide
complaining of/complaint of
CO2
COPD
COR-0
C-spine
C-section
CSF
CSM
CVA
CVP
CPR
d/c
D&C
detox
carbon dioxide
change
chronic obstructive pulmonary disease
cardiopulmonary arrest
cervical spine
cesarean section
cerebrospinal fluid
carotid sinus massage
cerebral vascular accident
central venous pressure
cardiopulmonary resuscitation
discharge/discontinue
dilatation and curettage
detoxification
D5W
dextrose 5% in water
D50W
DOA
DOB
DOE
DOS
Dr.
drsg/dsg
DT
Dx
↓
ea
ED
ECG/EKG
EENT
EMS
ENT
EOA
EOM
et
ET
ETT
ETA
etc
ETOH
exam
=
F
dextrose 50% in water
dead on arrival
date of birth
dyspnea on exertion
dead on-scene
doctor
dressing
delirium tremens
diagnosis
decrease
each
emergency department
electrocardiogram
eye, ear, nose, throat
emergency medical services
ear, nose, throat
esophageal obturator airway
extraocular movement
and
endotracheal
endotracheal tube
estimated time of arrival
and so forth
alcohol (ethyl)
examination
equal
Fahrenheit
Return to Table of Contents
FB
FD
fl
Fx
♀
1o
GB
GC
GCS
GI
g
GPA
gr
GSW
gtt(s)
GU
GYN
→
>
h/hr
HA
HACE
HAPE
HAZMAT
HB
HBV
Hct
HEENT
Hg
Hgb
HIV
H&P
HR
ht
Hx
hypo-
foreign body
fire department
fluid
fracture
female
first degree/primary
gallbladder
gonorrhea or gonococcus
Glasgow coma scale
gastrointestinal
gram
gravida, para, abort
grain
gunshot wound
drop(s)
genitourinary
gynecology
going to/leading to
greater than
hour
headache
high-altitude cerebral edema
high-altitude pulmonary edema
hazardous materials (incident)
heart block
hepatitis B virus
hematocrit
head, eyes, ears, nose, throat
mercury
hemoglobin
human immunodeficiency virus
history and physical
heart rate
height
history
low
H2O
ICS
ICU
I&D
IM
inf
int
IV
↑
J
JVD
water
intercostal space
intensive care unit
incision and drainage
intramuscular
inferior
internal
intravenous
increase
Joule(s)
jugular venous distention
Return to Table of Contents
K+
KVO/ TKO
L/l
L
lac
lat
LBBB
lb
lg
LLL
LLQ
LMP
LOC
L-spine
LUL
LUQ
<
potassium
keep vein open / to keep open
liter
left
laceration
lateral
left bundle branch block
pound
large
left lower lobe
left lower quadrant
last menstrual period
loss of consciousness
lumbar spine
left upper lobe
left upper quadrant
less than
O
lying
/\
♂
MAE
MAST
mcg
MCL
med(s)
mEq
Mg
mg/mgm
MI
misc
ml
mm
MOE x
Male
moves all extremities
medical antishock trousers, military antishock trousers
microgram
midclavicular line, modified chest lead
medication(s)
milliequivalent
magnesium
milligram
myocardial infarction
miscellaneous
milliliter
millimeter
movement of extremities times
MS/MSO4
MVA
N/A
NaCl/NS
morphine sulfate
motor vehicle accident
male
not applicable
normal saline
NaHCO3
NC
neg
NKA
noc/noct
NPO
NSR
NTG
N/V/D
sodium bicarbonate
nasal cannula
negative
no known allergies
night
nothing by mouth
normal sinus rhythm
nitroglycerin
nausea and vomiting and diarrhea
Return to Table of Contents
∅
none
O2
OB
occ
O.D.
OD
OJ
ophth
OPP
OR
Ortho
O.S.
O.U.
oz
P
PAC
PASG
PAT
path
PD
PE
oxygen
obstetrics
occasional
right eye (oculus dexter)
overdose
orange juice
ophthalmology
organophosphate poisoning
operating room
orthopedics
left eye (oculus sinister)
both eyes (oculus uterque)
ounce
after
premature atrial contraction
pneumatic antishock garment
paroxysmal atrial tachycardia
pathology
police department
physical examination/pulmonary edema/pulmonary
embolus
pediatrics
by or through
pupils equal and react to light
pupils equal and react to light and accommodation
pelvic inflammatory disease
paroxysmal nocturnal dyspnea
by mouth
positive
posterior
privately owned vehicle
paroxysmal supraventricular tachycardia
psychiatric
patient
prior to arrival
premature ventricular contractions
psychiatric
every
right
right bundle branch block
red blood cell
respirations
rheumatic heart disease/right hand dominant
right lower quadrant
rule out
range of motion
peds
per
PERL
PERLA
PID
PND
po
pos/ö/+
post
POV
PSVT
psych
pt
PTA
PVC
Ψ
q
®
RBBB
RBC
resp
RHD
RLQ
R/O
ROM
Return to Table of Contents
ROS
RUQ
Rx
s
SAB
SC/sub q
SL
SOB
sol
sm
stat
sup
Sx
surg
SVT
synch
2o
TAB
TB
tbsp
temp
TIA
tid
TKO
TLC
TM
tol
tsp
Tx
∴
3o
U/A
uncons
unk
URI
uro
UTI
≠
vag
VD
VF
via
vol
V/S
VT
WAP
WBC
review of systems
right upper quadrant
take, treatment
without
spontaneous abortion
subcutaneous
sublingual
shortness of breath
solution
small
at once
superior
sign/symptom
surgery
supraventricular tachycardia
synchronous
second degree/secondary
therapeutic abortion
tuberculosis
tablespoon
temperature
transient ischemic attack
three times a day
to keep open
tender loving care, total lung capacity
tympanic membranes
tolerated
teaspoon
treatment
therefore
third degree, tertiary
upon arrival
unconscious
unknown
upper respiratory infection
urology
urinary tract infection
not equal/unequal
vaginal
venereal disease
ventricular fibrillation
by way of
volume
vital signs
ventricular tachycardia
wandering atrial pacemaker
white blood cell
Return to Table of Contents
wc
WNL
WPW
wt
x
y/o
yr
wheelchair
within normal limits
Wolff-Parkinson-White Syndrome
weight
times
year(s) old
year(s)
Return to Table of Contents
COMBINED ADVANCE DIRECTIVES AND CPR DIRECTIVE
ADVANCE MEDICAL DIRECTIVES
A. There are several types of advance medical directives (documents in which a
patient identified the treatment to be withheld in the event the patient is unable to
communicate or participate in medical treatment decisions).
1. Do not resuscitate (DNR) orders are generally intended to be written by a
physician for a patient whose medical condition is such that commencement
of resuscitation efforts would be futile.
2. A Colorado living will ("Declaration as to Medical or Surgical Treatment")
requires a patient to have a terminal condition, as certified in the patient's
hospital chart by two physicians. For the document to become operative, the
patient must be unresponsive because of a terminal condition for a period of
seven days. In most cases, these do not impact prehospital care, but
become effective in the in hospital setting.
3. "Durable Medical Power of Attorney" or "Health Care Proxy" are documents
which can be very complex and require careful review and verification of
validity, and application to the patient's existing circumstances. Therefore,
the consensus is that resuscitation should be initiated until a physician can
review the document or field personnel can discuss the patient’s situation
with the base physician.
4. The Colorado CPR Directive is a specific situation under Colorado law that
provides for CPR to be withheld or withdrawn.
B. Resuscitation may be withheld from or terminated for a patient who has a valid,
written do not resuscitate order or other advanced medical directive only if:
1. The documentation is clear, unequivocally to the prehospital provider that
CPR, intubation and defibrillation are refused by the patient or by the patient's
attending physician who has signed the document, and
2. Base physician has approved of withholding or ceasing resuscitative efforts,
and
3. There is no apparent indication of suicidal gesture or intent by the patient.
4. If there is disagreement at the scene about what should be done, the base
should be contacted immediately for guidance.
5. Prehospital providers presented with equivocal DNR orders or advance
medical directives should proceed with resuscitation and establish base
contact for guidance on treatment and transport.
a. If the directive document is long and detailed, then it is probably more
reasonable for resuscitation to be initiated and the patient to be
transported so that the base physician can review the document and
possibly contact the patient's attending physician.
b. The duration of the resuscitation should be guided by the same factors of
any medical cardiac arrest.
C. Verbal DNR "orders" are not to be accepted by the prehospital provider. In the
event family or an attending physician directs resuscitation be ceased, the
prehospital provider should immediately CONTACT BASE. The prehospital
provider should accept verbal orders to cease resuscitation only from the base
physician.
D. There may be times in which the prehospital provider feels compelled to perform
or continue resuscitation, such as hostile scene environment, family members
adamant that "everything be done", or other highly emotional or volatile
Go to Table of Contents
situations. In such circumstances, the prehospital provider should attempt to
confer with the base for direction and if this is not possible, the prehospital
provider must use his or her best judgment in deciding what is reasonable and
appropriate, including transport, based on the clinical and environmental
conditions, and established base contact as soon as possible. Documentation of
these events must be explicit.
CPR DIRECTIVE PROTOCOL
General Principles
A. This protocol is for the prehospital management of the statutory "CPR Directive,"
which refers to a specifically identifiable, numbered form that is printed on
security paper. The form must be signed by the patient or the patient's
authorized agent. The form must also be signed by the patient's attending
physician.
B. In addition to the written CPR Directive form, the patient or authorized agent may
obtain a CPR Directive necklace or bracelet to be worn by the patient. This
bracelet or necklace will have imprinted on it the same number as the form.
C. CPR shall be withheld or terminated if the original CPR Directive form is readily
accessible with an original signature, or if the necklace or bracelet is worn by the
patient.
D. A CPR Directive may be implemented for a minor only after a physician issues a
"Do Not Resuscitate" order and the parents of the minor (if married and living
together), custodial parent, or legal guardian execute(s) a CPR Directive for the
minor.
E. A CPR Directive does not only apply to patients in full cardiac arrest, but should
also be honored by withholding resuscitation in patients who are seriously ill or
near arrest.
Procedure
A. Upon finding a patient with a CPR Directive (form, bracelet, or necklace):
1. Perform initial patient assessment.
2. Verify that the CPR Directive form is one of the original copies (it should be
light blue color below the title portion of document) and is unaltered (not
defaced or altered physically in some way).
3. Verify that the information on the form or, if present, on the back of necklace
or bracelet, appears to be appropriate for the patient (look at race, sex, date
of birth, eye and hair color). If possible, try to verify identity of patient by an
additional source (e.g., family member, driver's license or other readily
available sources).
4. Upon verification of the CPR Directive, withhold CPR. If CPR has been
started, it should be stopped.
5. If there is any question of the validity of the document or the identity of the
patient, initiate full resuscitation measures and contact the base for guidance.
Be sure to inform the base of the CPR Directive form, bracelet, or necklace,
and the condition and history of the patient.
6. Complete documentation, including attaching a copy of monitor strips on
each copy of the run report (EMT-P or EMT-I). Additional required
documentation is listed in section K below.
7. Provide appropriate emotional support to family if possible.
Return to Table of Contents
8. If the death occurs outside of a health care facility or if tissue donation has
been declared, then the coroner is to be immediately contacted. If the
declarant has indicated on the CPR Directives form a desire to donate any
tissues, appropriate authorities should be notified.
9. The following resuscitation measures are to be withdrawn or withheld from a
person who has a valid CPR Directive:
10. CPR and chest compressions
11. Endotracheal intubation or other advanced airway management
12. Artificial ventilation
13. Defibrillation
14. Cardiac resuscitation measures and medications.
B. The following interventions may be administered or provided:
1. Assist in maintenance of airway (non-advanced airway management, such as
positioning)
2. Suctioning
3. Oxygen
4. Pain medication
5. Control bleeding
C. In addition to the standard documentation, the following information should be
documented when possible by the prehospital provider on the run report:
1. Patient's status (e.g. condition found, medical history obtained)
2. Type of "CPR Directive" found (document, bracelet or necklace)
3. CPR Directive number
4. Name of attending physician, if known
5. Special circumstances which justify initiating resuscitation if this was done
despite the presence of the CPR Directive
6. Monitor strips in at least two leads (EMT-P and EMT-I)
Additional Considerations
A. The patient may revoke the CPR Directive at any time by oral expression of
revocation or by destruction of the CPR Directive form, bracelet or necklace. If a
guardian, agent or proxy decision-maker executed the CPR Directive, then the
guardian, agent or proxy decision-maker may revoke the CPR Directive.
B. CPR is to be initiated if the original CPR Directive form, necklace or bracelet is
not readily available, (i.e., being worn by or physically present with the patient).
The bracelet or necklace is only available to the patient after the form has been
properly executed. Removal of the bracelet or necklace may be construed as
revocation. Therefore, if the bracelet or necklace is readily accessible but not on
the patient, any question as to whether or not the Directive has been revoked
should result in resuscitation until the situation is clarified. Consult with base if
you have questions about terminating CPR and transport. If not in full arrest,
patients with CPR Directives may still be transported to provide comfort
measures.
C. In the absence of the existence of a CPR Directive, a person's consent to CPR
shall be presumed. The statutorily authorized CPR Directive is only one manner
for a patient to document resuscitation preferences. Other "Do Not Resuscitate"
forms and advance directives may be honored but base contact is required.
D. Under Colorado Law, refraining from performing CPR, when there is a CPR
Directive, does not constitute assisting a suicide, and caregivers who honor a
CPR Directive by withholding CPR are protected from legal liability.
Return to Table of Contents
COMMUNICATION
A. The purpose of contacting the receiving hospital is to provide enough data to
allow the Emergency Department staff to decide what preparations they will need
to make for the patient. In addition, a base physician may direct appropriate
treatment to be administered en route.
B. Radio contact should only include essential, relevant information. Remember,
the Emergency Department staff may be busy and radio time is valuable.
C. First, always identify agency, unit, person, and the reason for contact such as a
treatment orders/requests, notification, and/or consultation.
Procedure for Notification to Receiving Facility
A. Report the following, to the extent pertinent, to the receiving facility:
1. Transport status or code
2. Chief complaint
3. Age and gender of patient
4. General status and course of events, stable, improving, deteriorating
5. Past medical history, only if pertinent
6. State of consciousness
7. Vital signs
8. Pertinent localized findings
9. Treatment in progress
10. Estimated time of arrival
Procedure for Requests for Treatment Orders
A. Only a physician may provide authorization to a paramedic to perform a
procedure or administer a medication pursuant to these protocols. The
paramedic should be clear and concise in requesting that a physician be
available for consultation or orders.
B. Request to talk to a physician to obtain an order.
C. Identify yourself to the physician and state the order you are requesting.
D. Provide pertinent information that is the basis of the request, such as:
1. Enroute (emergent or non-emergent, estimated time to destination hospital)
or on scene
2. Chief complaint
3. Course of events, stable, improving, deteriorating
4. Past medical history, only if pertinent
5. General status
6. State of consciousness
7. Vital signs
8. Pertinent localized findings
9. Treatment in progress
10. Order requested, stating dosage and route to be given
11. All allergies the patient has
E. In the event a request is for a field pronouncement, the report should include
information about the responses to resuscitation efforts, mechanism, and
duration of resuscitation efforts. If the pronouncement is made, state the time.
F. Communication with a physician at the base is appropriate if you are not sure
whether or not a treatment, procedure or destination is appropriate for a patient.
Go to Table of Contents
BASE CONTACT should be considered as a consultation, not just as a source of
authorization for medications and procedures.
G. Requests for orders should be made to a hospital's recorded line whenever
possible.
Return to Table of Contents
DESTINATION POLICY
Purpose
A. To provide a set of guidelines to help ensure proper disposition of the various
patients encountered in the field.
Philosophy
A. Critical patients with a special medical need should be taken to the nearest
facility that can best provide for that need.
B. Critical patients without a special need (i.e., cardiopulmonary arrest) should be
taken to the closest emergency department.
C. All other patients should have their request accommodated, consistent with the
ability of that system to meet that request.
Special Needs
A. Burns
1. Patients older than 12 years of age, with second degree or third degree burns
greater than 20% body surface area, should be transported directly to the
University Hospital emergency department. Patients 12 years of age and
younger, with second degree or third degree burns greater than 20% body
surface area, should be transported directly to The Children's Hospital
emergency department.
2. Special Considerations. Complications of airway compromise or
cardiovascular instability, require transport to the nearest appropriate
emergency department. Burns associated with multi-system trauma should
be transported according to the State of Colorado Trauma Triage Algorithm
and RETAC rules.
B. Trauma
1. The destination of trauma patients should always be in accordance with the
Colorado Department of Health approved Rules and Regulations and RETAC
rules.
C. Psychiatric patients
1. Patients placed on a Mental Health Hold (MHH) by the Denver Police
Department or Mental Health Corporation of Denver shall be transported to
DHMC.
2. Patients placed on a MHH by other police departments or other state licensed
providers shall be taken to the nearest emergency department.
3. Patients with psychiatric problems not on an MHH shall be taken to the
closest hospital.
4. Patients with psychiatric problems who have an acute medical or traumatic
concern shall be treated according to the appropriate medical or trauma
protocol.
5. MHH may be placed by a state-certified EMT-P under the auspices of the
receiving physician.
D. Obstetric/Gynecologic
1. For patients in uncomplicated labor:
a. Delivery not imminent:
i.
If the patient has a private obstetrician or gynecologist, then follow the
patient's request for destination, when possible.
Go to Table of Contents
b. If the patient has no private physician, then follow the patient's request for
destination (if expressed), or transport to the closest hospital.
2. Imminent delivery
a. If the patient has a private obstetrician/care giver, then follow the patient's
request for destination, when appropriate. If the requested facility does
not meet these time constraints and the patient still requests the facility,
CONSULT BASE physician.
b. If the patient has no private physician, then transport to the closest
appropriate hospital.
Return to Table of Contents
DIVERT POLICY
(modified with permission from document created by Art Kanowitz, Pridemark Paramedic
Services)
Purpose
A. To provide a standard approach to ambulance diversion that is practical for field
use.
B. To facilitate unobstructed access to hospital emergency departments for
ambulance patients
C. To allow for optimal destination policies in keeping with general EMS principles
and Colorado State Trauma System Rules and Regulations.
General Principles
A. EMSystem, an internet-based tracking system, is used to manage diverts in the
Denver Metro region.
B. The State Trauma Triage Algorithms should be followed.
C. The only time an ambulance can be diverted from a hospital is when that hospital
is posted on EMSystem as being on official divert (RED) status. As of December
15, 2001, Emergency Department divert is the only category recognized in the
Denver Metro region.
D. Overriding factors: the following are appropriate reasons for a paramedic to
override ED divert and, therefore, deliver a patient to an emergency department
that is on ED divert:
1. Cardiopulmonary arrest
2. Imminent cardiopulmonary arrest
3. Unmanageable airway emergencies
4. Unstable “Level I” trauma patients for Level I and Level II trauma centers
E. Prehospital personnel should honor advisory categories, when possible,
considering patient’s condition, travel time, and weather. Patients with specific
problems that fall under an advisory category should be transported to a hospital
not on that specific advisory when feasible.
F. There are several categories that are considered advisory (yellow) alert
categories. These categories are informational only and should alert field
personnel that a hospital listed as being on an advisory alert may not be able to
optimally care for a patient that falls under that advisory category.
G. The following are advisory (yellow) categories:
1. ICU (Intensive Care Unit)
2. OB (Obstetrics)
3. Psych (Psychiatric)
4. Trauma (Trauma Services)
5. Operating Room (OR)
H. Zone saturation is when all hospitals in that zone are on ED Divert.
I. A Zone Master is a hospital contact that is responsible for determining hospital
destinations when the zone is saturated.
J. When an ambulance is transporting a patient that the paramedic feels cannot go
outside the zone due to patient acuity or other concerns, the paramedic should
contact the Zone Master and request a destination assignment.
K. In general, patients contacted within a zone should be transported to an
appropriate facility within the zone. Patients may be transported out of the
Go to Table of Contents
primary zone at the paramedic’s discretion, if it is in the patient’s best interest or
if the transport to an appropriate facility is shorter.
L. The zones, hospitals in each zone, Zone Masters, and the Zone Master contact
phone numbers listed in the following table.
ZONE
HOSPITALS
ZONE MASTER
ZONE MASTER
PHONE NUMBER
Zone 1
North Suburban
St. Anthony’s North
St. Anthony’s Central
Lutheran
St. Anthony’s Central
303-595-6135
Zone 2
SOUTH
Swedish
Porter
Littleton
Sky Ridge
Swedish
303-788-6911
Zone 3
EAST
University
Rose
Aurora
Parker
Aurora AND University*
NORTH/
NORTHWEST
303-695-2946 - Aurora
ALTERNATE every
QUARTER:
1st and 3rd quarter –
Aurora
720-848-5120 University
2nd and 4th quarter University
(*Zonemaster date rollover
occurs at midnight on the
first day of each quarter.)
Zone 4
MIDTOWN
Denver Health
St. Joseph/Kaiser
Presbyterian-St. Luke’s
Return to Table of Contents
Denver Health
303-436-8100
ATAC ADULT PREHOSPITAL TRAUMA TRIAGE ALGORITHM
COLORADO STATEWIDE TRAUMA SYSTEM AREA TRAUMA ADVISORY COUNCILS
ADULT PREHOSPITAL TRAUMA TRIAGE ALGORITHM
The Denver Metro EMS Medical Directors now recommends the use of local RETAC
rules for this protocol.
Go to Table of Contents
COLORADO STATEWIDE TRAUMA SYSTEM
PEDIATRIC PREHOSPITAL TRAUMA TRIAGE ALGORITHM
Triage and transport requirements for pediatric (< 12 years old*) trauma patients
The Denver Metro EMS Medical Directors now recommends the use of local RETAC
rules for this protocol.
See also: Boulder Specific Trauma Activation Protocol
Go to Table of Contents
HAZARDOUS MATERIALS (HAZMAT)
Indications
A. Responding to reported and/or known hazardous materials incident
B. Vapor clouds, fire, smoke, leaking substances, frost lines on cylinders, sick
personnel, dead or distressed animals and noxious odors are present on or near
scene.
Precautions
A. Senses are one of the best ways to detect chemicals, particularly the sense of
smell. If you smell something you are too close.
B. A safe approach to the scene is the first element of any EMS response. Unless
you arrive safely at the site, you will not be able to perform your duties.
C. Observe the site from a distance using binoculars, if possible, before you get too
close. Look for danger signs such as vapor clouds, fire and smoke, placards,
shape of vehicle or container, leaking substances, frost lines on cylinders, injured
personnel, and dead or distressed animals. These are key clues to warn you not
to get too close. Remember that you want to be part of the solution, not part of
the problem.
D. If the fire department is already on the scene, report in to the incident
commander. If you are first on the scene and a hazardous material is
suspected, request a hazardous materials team response. Keep yourself and
your unit at a safe distance. This usually requires your unit to leave the scene,
leaving patients and bystanders in a hazardous situation. Your safety comes
first. Seek a location uphill and upwind from the incident.
E. EMS personnel should not be participating in patient decontamination unless
trained and equipped to do so in a safe manner.
Procedure
A. Your safety is the highest priority. EMS operations should be established in the
cold zone. You should report to the incident commander.
B. Position your vehicle to make a hasty retreat. This may require you to leave the
scene to seek safety.
C. The hazardous materials team should perform the initial assessment, treatment,
and decontamination. Decontaminated patients should then be brought to the
EMS unit.
D. Once the situation has been assessed, notify the receiving hospital of the
following information:
1. Location of the incident
2. Name of chemicals/products involved
3. Number of injured and contaminated
4. Extent of the injuries/contamination
5. Extent that the patients will be decontaminated in the field
6. Your estimated time of arrival
7. Other pertinent information that is available
E. Patient treatment is usually based on signs and symptoms. Specific patient
treatment should be based on information obtained from BASE CONTACT.
Go to Table of Contents
HELICOPTER TRANSPORT
A. Air transport is a useful adjunct to the EMS System. The risks and benefits of the
helicopter transport should be carefully weighed, especially when flying into a
less than optimal landing zone. Benefits of helicopter transport should be
considered when:
1. Rapid transport is desired. An obvious beneficiary of air transport is the rural
trauma victim requiring rapid transport to the trauma center.
2. Multiple victims require multiple unit response/transport.
3. Extrication is complicated by difficult access requiring prolonged scene time.
4. Advanced life support is not available by ground within a reasonable time
period.
B. In order to effect the most expedient use of ground and air ambulance resources,
the following guidelines should be considered:
1. The helicopter should be placed on standby when responding to a scene
which may include any of the elements listed in section A.
2. The helicopter should be dispatched when it is the most appropriate means of
transport.
3. In order to save time, the helicopter should be contacted through your own
dispatched.
4. Please note that an accurate ETA will not be available until the helicopter is
actually airborne. Consider alternative flight services or ground transport if the
helicopter is not immediately available.
5. Generally speaking, the helicopter will stand-down only when so requested
by the agency initiating the original response. Do not forget to stand down or
cancel the helicopter if it is not required.
6. Public safety officers should be informed of the impending arrival of the
helicopter.
7. Patient care in the field is a team response. State statutes dictate that
ultimate responsibility rests with highest trained medical person on the scene.
In this regard, the flight nurse assumes responsibility only for the patients
turned over to him/her by the attending EMS personnel, unless the flight
nurse is the first EMS person on the scene.
Go to Table of Contents
INFECTIOUS and COMMUNICABLE DISEASES
A. Field personnel occasionally come into contact with infectious and communicable
diseases. It is important that a protocol is followed so that the appropriate
persons are notified. Not all diseases require immediate treatment; however,
early awareness will assist those involved to take any necessary precautions and
actions.
B. Contamination by infectious and communicable diseases may be minor or
serious. Field personnel should take precautions to avoid unnecessary exposure.
When dealing with a suspected contagious patient, attempt to avoid direct
contact with the patient's blood, sputum, emesis, urine, feces, or respiratory and
lesion secretions. The provider should wear disposable latex or vinyl gloves and
any other appropriate BSI. Routine practice of good hand washing and
equipment cleaning may help decrease the incidence of contamination.
C. The following guidelines have been provided for reference. Follow your
individual agency infectious and communicable disease exposure policy and
procedure.
1. All healthcare personnel should always practice good hygiene before, during
and after delivering patient care. Each patient contact should be considered
to be a potential source of infection.
2. Persons with significant exposure must report the incident to the designated
Infection Control Officer of his/her agency. All personnel should be advised to
consult with their private physician as well.
3. Agency policy, developed in conjunction with the Physician Advisor, will
dictate procedure with regard to screening, follow-up testing, prophylaxis
and/or treatment.
4. Exposed prehospital care personnel may be counseled and treated according
to established guidelines.
5. Refer to the following website resource for information on diseases, means
and methods of exposure, exposure risks, and recommended precautions,
actions, and treatment: www.cdc.gov
Go to Table of Contents
INTERHOSPITAL TRANSFER
A. Interhospital patient transfers are commonly initiated when definitive diagnostic
or therapeutic needs of a patient are beyond the capacity of transferring hospital.
In these cases the patient may be unstable, and medical treatment must be
continued and possibly even initiated en route. Likewise, patients being
transferred for diagnostic or therapeutic purposes may be stable but on
continuous pharmacological or ventilatory therapy. It is imperative that such
therapies be continued or interruptions in care planned to minimize risk to the
patient. These guidelines encourage orderly transfer of patients with appropriate
continuity of care.
B. All patients should be stabilized, if possible, before transfer.
C. Attending EMT or paramedic should receive a summary of the patient’s
condition, current treatment, possible complications and other pertinent medical
information.
D. Treatment orders should be given to the attending EMT or paramedic. These
orders should be either in writing or by direct verbal order from the doctor who is
initiating the transfer.
E. Any unstable or potentially unstable patients must have at least one IV in place.
Orders for IV fluid and rate should be provided.
F. Transfer papers (summary, lab work, x-rays, etc.) should be given to the
attending EMT or paramedic, rather than the family or friends.
G. The attending EMT or paramedic should confirm that the receiving hospital and
physician have been notified prior to initiation of transfer.
H. The personnel used to transfer a patient should be appropriate to the treatment
needed or anticipated during transfer. EMT-Bs who are not IV approved should
not attend patients who have or may require IV therapy. Paramedics should be
utilized if any advanced resuscitation or treatment is anticipated. In specialized
fields not ordinarily handled by paramedics (i.e. high risk obstetrics, high risk
newborns) an appropriately trained person should accompany the patient.
I. The equipment used to transfer a patient should be appropriate to the treatment
being provided. Example: IV medications being delivered by an IV pump should
be either maintained on an IV pump during the transfer, discontinued, or the IV
tubing be appropriate to the manual control. In order to maintain these standards,
it may be appropriate for the receiving hospital to send an ambulance with more
specifically trained personnel to transfer the patient. This is particularly true in the
case of newborns, but has also been shown to be effective in the treatment of
other critically ill or injured patients
Go to Table of Contents
MENTAL HEALTH HOLDS (MHH)
Indications
A. Any person who appears to be:
1. mentally ill and
2. an imminent danger to others or to him/herself or
3. gravely disabled
Procedure
A.
B.
C.
D.
Restrain if necessary.
Call receiving facility for the physician to place MHH.
Transport to Emergency Department.
Provide appropriate documentation of events so 72-hour MHH can be filled out
by the physician at the receiving facility.
General Principles
A. The paramedic may initiate an MHH only with the permission and online contact
with the receiving physician.
B. The law allows only physicians, trained nurses, and peace officers to place MHH.
C. Paramedics may act as the field representative of the physician when the above
protocol is followed.
Go to Table of Contents
NON-TRANSPORT OF PATIENTS
General Principles
A. A patient who has decision-making capacity may refuse treatment, examination
or transport.
B. A person has decision-making capacity sufficient to refuse treatment/transport if
he/she:
1. Understands the nature of the illness/injury or risk of injury/illness; and
2. Understands the possible consequences of refusing treatment/refusing
transport; and
3. Given the risks and options, the patient voluntarily refuses
treatment/transport.
C. The prehospital provider is responsible for deciding if the patient's refusal is
informed and voluntary. The prehospital provider should consider the nature of
the incident, potential mechanism, obvious actions of the patient, as well as the
verbal statements of the patient. The prehospital provider is responsible for a
reasonable assessment of the patient to determine if there is an injury/illness or
reason for transport or treatment. Only then is a patient's refusal an informed
refusal. Do not attempt to diagnose, do assess carefully.
D. Remember: it is your assessment and advice to the patient, and proper
documentation of it, that are most important in the non-transport.
Procedure for Non-Transports (See Non-Transport/Refusal of Care Algorithm
following)
A. If the patient is 18 years of age or older, has no demonstrable illness or injury,
has no mechanism of injury, demonstrates competency (as defined in the
“Consent” portion of this section), and did not initiate the call for help, then base
contact is not required.
B. For the patient who has only an isolated soft tissue injury and has decisionmaking capacity, treatment and transport should be offered. If the patient
refuses, then warn the patient of the risks of non-transport and delay in
treatment. Agency policy determines base contact requirement.
C. Patients with medical conditions/injuries that may recur or deteriorate, or may
render the patient unable to seek medical care, should be carefully evaluated
and warned to not delay in obtaining medical treatment. High-risk areas in EMS
are head injury, chest pain, abdominal pain, "flu" like symptoms, alcohol-related
illnesses, or injuries.
D. For the patient refusing transport/treatment:
1. Assess patient to the extent possible. Look for objective causes of
injuries/illnesses that may impair decision-making. Evaluate
mechanism/history, scene and potential for unseen injuries/illnesses. Do not
diagnose.
2. Inform patient of findings, possible injuries or illnesses that warrant treatment
and transport, and of the risks of non-transport, delaying treatment, and nonphysician examination.
3. If the patient still refuses treatment/transport, then determine the patient's
ability to understand the immediate medical situation and need for treatment.
Questions asked might include:
a. Why don't you want to go to the hospital?
b. What other means of transport do you have?
Go to Table of Contents
E.
F.
G.
H.
I.
J.
K.
L.
c. What will you do if you get sick again?
d. What are the risks I just explained to you about delaying treatment?
If the patient still refuses transport, CONTACT BASE.
The base physician may:
1. Agree or determine that the patient's decision-making capacity is impaired
and instruct transport of the patient.
a. The patient may be transported under the basis of a medical emergency
(i.e., patient is incapacitated and unable to consent.)
b. The patient may be transported under the basis of a mental health
emergency. Police should be requested to place the patient under a
Mental Health Hold. Appropriate paperwork, such as the Mental Health
Hold, must accompany the patient.
2. Agree or determine that the patient has decision-making capacity, in which
case:
a. The patient may refuse treatment and transport but must be advised of
the risks of non-transport (informed refusal).
b. The prehospital provider must warn the patient that non-transport is
against medical advice (AMA).
c. The patient should be urged to seek medical attention and transport.
For the patient who refuses treatment and transport (against medical advice),
providing the patient with clear instructions and warnings is imperative. Use of an
Information Sheet is recommended.
Minors: CONTACT BASE any time a minor under the age of 18 is not left in the
custody of the parents.
The following must be documented for every patient examined, offered and
refused treatment/transport (in addition to EMS Division guidelines):
1. All assessment findings
2. Description of mechanism or scene factors (damage, environment, etc.)
3. Description of mental status and decision-making capacity
4. Vital signs, unless the patient refused
5. Patient's response to warning about risks of non-transport/non-treatment
6. Base physician's advice
7. Patient's condition at termination of patient contact, such as “ambulatory”,
“with family”
The "AMA" (refusal) patient should be provided with an Information Sheet.
Obtaining a patient's signature on a run report or release form is encouraged
because signing may be evidence of the patient's decisional capacity and
physical stability. However, do not have a patient sign a release or waiver that
you do not understand, and do not expect that a signature relieves you of
responsibility for a reasonable assessment or treatment of the patient.
The role of base contact is to assist in determining or verifying the patient's ability
or inability to make medical treatment decisions and assist when transport should
be done. It is imperative that an accurate, concise report be given for the
physician to give good advice.
Have all AMA forms co-signed by a witness. The witness should not be an
employee of the responding agency.
Return to Table of Contents
NON-TRANSPORT/REFUSAL OF CARE ALGORITHM
(See Non-Transport of Patients protocol)
Determine mental status and extent and history of
injury, mechanism or illness
Pt is alert, oriented and has decisionmaking capacity
• No apparent
injury/illness
• No complaints
• No significant
history
• No MOI
Limited injury
consistent with
mechanism
Injury or illness or has impaired decisionmaking capacity
Pt refuses consent or offer of treatment
and transport
Contact Base
Offer treatment and
transport
Base physician
determines pt does
have decisionmaking capacity
18 years or older
and did not call for
help
Pt still refuses
Pt does not want
help
Refer to agency
policy
Warn pt of risks of
nontreatment/transport
against medical
advice
Document
appropriately
Advise pt and
document
appropriately
Base physician
determines pt does
not have decision
making capacity.
(Treatment/transpo
rt may be
authorized under
MHH, ATH or
implied consent if a
medical
emergency exists
Transport: request
MHH or police if
necessary for
assistance
Base contact
Return to Table of Contents
Document
appropriately
TRIAGE: MULTIPLE PATIENT ASSESSMENT
REFER TO: THE COLORADO STATE UNIFIED DISASTER TAG AND TRIAGE
SYSTEM - A GUIDE TO MCI (multiple/mass causality incident)
Definition
A. MCI: The combination of numbers and types of injuries that goes beyond the
capability of an entity's normal response.
B. Triage: From French - means to sort, sift, or pick out; specifically, the sorting of
and allocation of treatment to patients.
Indications
A. Medical emergency involving more than one patient, interaction between different
agencies, and the need to make choices regarding treatment.
Procedure
A. Park vehicle in safe location.
B. Contact appropriate command personnel and follow instructions.
C. If assigned to triage, do initial assessment of scene; proceed only when safe to
rescuer.
D. Rapidly estimate number of victims and severity of injuries. Do not provide
extensive treatment.
E. Establish communications and request necessary assistance as per department
or agency procedure; this may include contacting the appropriate hospital and
providing initial estimate of number and types of injuries.
F. Designate or ensure designation of:
1. The Incident Command System (ICS) depending on the size of the event and
the number of agencies involved (see Diagram A - Incident Command
System)
2. Medical command: follow departmental and jurisdictional procedures.
3. Medical Triage Team:
a. Categorize patients after brief assessment using the Simple Triage and
Rapid Treatment START) system (see Diagram B - START Algorithm).
b. Update categorizations and provide transport to stabilization area as able.
c. Initiate medical stabilization to patients awaiting transport after triage
duties completed.
4. Transport Team (if necessary):
a. Transport patients in order of priority from field to stabilization area.
b. Establish venous access or perform other stabilization procedures as
needed in support of triage team.
c. If ongoing assessment, categorization, and transport are to be required,
organize the area into an appropriate Triage/MCI format (see Appendix
Section F, Triage/MCI Templates; diagrams C-1, C-2, and C-3)
Precautions
A. Identification of medical charge personnel is extremely important and often
overlooked. Use vests, hats, or other labeled equipment consistent with
departmental or agency procedures.
B. Location of stabilization area is very important. It should fulfill the following
criteria as much as possible:
Go to Table of Contents
1.
2.
3.
4.
Away from objective dangers of scene
Close enough for access from scene for stretchers
Accessible by multiple rescue vehicles, both in and out
Near communications and other command personnel for coordination of
evacuation
C. If triage tags are part of departmental or agency procedures, attach triage tags to
patient, not clothing.
D. Triage assessment and management differs from single patient assessment.
Certain problems recur in major disasters, and should be avoided:
1. Do not use up ambulance space initially transporting class III (green) patients
before more serious injuries have been transported (red and yellow).
2. Do not delay transport to treat patients at the scene.
3. Reassess patients when able and communicate any changes to the medical
command and transport officers.
4. Disaster scenes require discipline within the team. Be sure that the
leadership and individual roles are well identified. It is important that
individuals fulfill their roles as members of the team and in turn give up those
roles appropriately as personnel and officers arrive to the MCI scene.
Special notes
A. The Incident Command Structure developed and disseminated by the National
Interagency Incident Management System (NIIMS) and Federal Emergency
Management Agency (FEMA) provides an excellent overall approach to disaster
management. The structure is designed to allow flexibility and local differences,
as well as incorporation of different training levels (physician, nurse, paramedic,
EMT-B) within Medical Control at the scene. It is important that individuals are
aware of the command structure and follow instructions. (see ICS Flow chart
below).
B. Multiple trauma patients with no vital signs upon arrival of rescue personnel have
a very poor chance of survival even if they are the only victim. If there are
additional victims with any signs of life, attention will be better spent with the
living.
Return to Table of Contents
INCIDENT COMMAND SYSTEM
* Command system with group and branch divisions based on functions
Incident Commander
Operations
Branch
(i.e. fire)
Triage Officer
Triage Group
Medical
Branch
Treatment
Officer
Branch
(i.e. law enforcement)
Transport
Officer
Logistics
Officer
Deputy
Transport
Officer
Area Leaders
Clerk
Leader
Group 0
(Black tags)
Leader
Group I
(Red tags)
Leader
Group II
(Yellow tags)
Leader
Group III
(Green Tags)
Area Staff
Area Staff
Area Staff
Area Staff
Go to Table of Contents
START TRIAGE FLOWCHART
Respirations
No
Yes
Reposition
Airway
No
Yes
NonSalvageable
Black Tag
Immediate
Red Tag
>30 / minute
<30 / minute
Immediate
Red Tag
Assess
Perfusion
Capillary refill >2
seconds OR
No palpable radial
pulse
Capillary refill <2
seconds OR
palpable radial pulse
Immediate
Red Tag
Assess Mental
Status
Fails to follow simple
commands
Able to follow simple
commands
Immediate
Red Tag
Delayed
Yellow Tag
Remember – Patients that can initially ambulate with or without assistance are GREEN
tags. Constant reassessment is necessary and there should be no hesitation in uptriaging when necessary.
Go to Table of Contents
CRITICAL CARE TRANSPORT UTILIZATION GUIDELINES
Revised: January 22, 2008
Purpose
A. To effectively triage and process any request for service in which Critical Care
Transport (CCT) may be utilized.
Policy
A. The Communications Center employees will utilize the standard operating
procedures to process CCT requests and appropriate utilization of CCTs and
ALS resources to manage acute patients. A request of services within the scope
of an Advanced Life Support paramedic-staffed ambulance will be scheduled as
a non-CCT transport unless specifically requested by the transferring physician.
This policy is included as a reference for clarity and support in decision making
for Denver Metro paramedics and other non-CCT staff.
Definition
A. CCT: Transport of a patient whose clinical needs in transport exceed those
procedures and medications included in the acts allowed for paramedics, and for
whom additional care providers are required (RN, RT, etc.).
Procedure
Mandatory Critical Care Utilization
The following situations will result in utilization of a Critical Care Transport:
Patient Origin/Destination
A. Intensive care unit (ICU) to ICU or Cardiac Care unit (CCU) unless the following
criteria are met:
1. Patient on a psychiatric hold in an ICU, with medical clearance completed
(versus mental health clearance)
2. Patients in ICU because of non-ICU overflow or telemetry bed overflow status
at the referring or receiving facility
B. CCU or ICU to Cardiac Cath Lab unless the following criteria are met:
1. Patients with acute myocardial infarctions 36 hours out or greater from
admission who have no ongoing chest pain, malignant arrhythmias, or
cardiovascular instability (non-emergent cath only).
2. Patients with Acute Coronary Syndrome who have been ruled out for
myocardial infarction after 12 hours or more. They should have no ongoing
chest pain, malignant arrhythmias, or cardiovascular instability (non-emergent
cath only).
Monitoring/Equipment/Medication Needs
A. Transports requiring intra-aortic balloon pump
B. Transports requiring invasive treatment modalities including:
1. Non-standard airway management, requiring conscious sedation and/or
anesthetic agents
Go to Table of Contents
2. Intensive care monitoring (condition in which clinical presentation in or is at
risk of being unstable, including: intracranial monitoring devices, arterial lines,
Swan-Ganz catheters, etc).
C. Patients requiring medications and infusions not approved by the Denver Metro
Protocols.
D. Patients on vasoactive infusions initiated or adjusted within two hours of
transport. (“2-hour rule”)
E. Patients requiring fetal monitoring/high risk OB patients
Instability
A. Multi-Systems trauma patient < 24 hours post-injury with a potential for
hemodynamic instability as determined by the transferring physician
B. Patients with known cardio-thoracic compromise (e.g., AAA, dissecting
aneurysms)
C. Hemodynamically unstable patient.
D. Any other patient whom the sending facility indicates is clinically unstable (a
physician or registered nurse must authorize the use of the CCT)
Exceptions
A. Patients may be sent by paramedic ambulance if, in the opinion of the
transferring physician, time consideration outweighs the need for RN presence if
the following criteria are met:
1. Critical Care Transport Services are not available in a reasonable response
time.
2. There is no nurse available from the sending facility to accompany the
transport.
3. The transport requirements are not outside of the acts allowed for
paramedics, or the medications specified by the Denver Metro Protocols.
4. The sending facility will provide additional resources when possible including
other staff, IV pumps, etc.
Medications
A. The following is a complete list of medications that the Pridemark Protocols
authorize Colorado State Paramedics to administer and maintain pursuant to the
scope of practice under Rule 500 Acts Allowed for the State of Colorado.
B. Denver Metro Protocol Pharmacy List:
1. Adenosine (Adenocard)
2. Albuterol Sulfate
3. Antibiotics
4. Amiodarone
5. Aspirin (ASA)
6. Atropine
7. Dextrose 50%
8. Diazepam (Valium)
9. Diphenhydramine (Benadryl)
10. Dopamine (Intropin)
11. Epinephrine
12. Fentanyl
13. Furosemide (Lasix)
Return to Table of Contents
14. Glucagon
15. Haloperidol (Haldol)
16. Heparin
17. Ipratropium Bromide (Atrovent)
18. IV Solutions
19. Magnesium Sulfate
20. Methylprednisolone (Solu-Medrol)
21. Metoclopramide (Reglan)
22. Midazolam (Versed)
23. Morphine Sulfate
24. Naloxone (Narcan)
25. Nitroglycerin
26. Ondansetron (Zofran)
27. Oral Glucose (Glutose, Insta-Glucose)
28. Oxygen
29. Phenylephrine (Intranasal)
30. Promethazine (Phenergan)
31. Racemic Epinephrine (Vaponephrine)
32. Sodium Bicarbonate
33. Topical Ophthalmic Anesthetics
C. Maintenance IV Infusions
D. IV Solutions
1. 0.9% Normal Saline
2. Lactated Ringers
3. D5W
4. Any combination of the above solutions
E. Vasoactive Drips
1. Dopamine (2-hour rule)
2. Epinephrine (2-hour rule)
Medications or infusions not included in this section will most likely require CCT
transfer or, at a minimum, an EMS physician consult and approval.
The Communications Specialist should use the CCT vs ALS Transport Algorithm to assist in the
determination of the Level of Care:
Return to Table of Contents
CCT vs ALS Transport Algorithm
Has the PHYSCIAN REQUESTED that the patient
be transported by CCT.
yes [ ]
CCT
No [ ]
Intensive Care Setting to antoher Intensive Setting
ICU to ICU, PICU to NICU, SICU to CICU, etc.
yes [ ]
CCT
No [ ]
Is the patient being transport from an ICU to a procedure
and then returning to the ICU?
yes [ ]
CCT
No [ ]
Will the patient have any medication drips running
during transport?
yes [ ]
No [ ]
Will the patient have any special equipment needs?
___ Intra-aortic balloon pump
___ Chest tube to drainage
___ Arterial Line
___ Invasive Pressure Monitoring (Arterial, ICP, CVP)
yes [ ]
List Medications: __________________________________________
_________________________________________________________
_________________________________________________________
_________________________________________________________
_________________________________________________________
CCT
yes [ ]
Are any of these medications outside
of the (BME / Metro Protocols defined)
paramedic scope of practice? (See Back)
No [ ]
If any question whether CCT Vs ALS
Call Director of Clinical Medicien 720-641-4093
Date:
Time:
Patient Name:
No [ ]
Run Number:
Ordering MD:
Assigned Unit:
Receiving MD:
ALS Ambulance
All patients requiring CCT transport should be referred to Flight for Life of Colorado unless
another service is specifically requested by the caller.
Return to Table of Contents
Appendix F TRIAGE/MCI TEMPLATES
Simple Triage Template
OMCI
Triage Area
Green
Black
Yellow
Red
Landing
Zone
Ingress / Egress
Go to Table of Contents
Moderate Triage Template
OMCI
Green
Black
Triage Area
Yellow
Red
Supply
Ingress /
Egress
Landing
Zone
Staging
Go to Table of Contents
Complex Triage Template
OMCI
Bus
Coroner
Green
Black
Triage Area
Yellow
Red
Supply
Landing Zone
Egress
Staging
Go to Table of Contents
Ingress
Egress
Staging
PEDIATRIC PATIENT ASSESSMENT
Children can be examined easily from head to toe, but lack of understanding by the
patient, poor cooperation, and fright often limit the ability to assess completely in the
field. Children often cannot verbalize what is bothering them, so it is important to do a
systematic survey which covers areas that the patient may not be able to tell you about.
Any observations about spontaneous movements of the patient and areas that the child
protects are very important. In the patient with a medical problem, the more limited set of
observations listed below should pick up potentially serious problems.
A. General:
1. Level of alertness, eye contact, attention to surroundings
2. Muscle tone: normal, increased, or weak and flaccid
3. Responsiveness to parents, caregivers; is the patient playful or irritable?
B. Head:
1. Signs of trauma
2. Fontanelle, if open: abnormal depression or bulging
C. Face:
1. Pupils: size, symmetry, reaction to light
2. Hydration: brightness of eyes; is child making tears? Is the mouth moist?
D. Neck: note stiffness.
E. Chest:
1. Note presence of stridor, retractions (depressions between ribs on
inspiration) or increased respiratory effort.
2. Auscultate the chest:
3. Breath sounds: symmetrical, rales, wheezing?
4. Heart: rate, rhythm
F. Abdomen: distention, rigidity, bruising, tenderness
G. Extremities:
1. Brachial pulse
2. Signs of trauma
3. Muscle tone, symmetry of movement
4. Skin temperature and color, capillary refill
5. Areas of tenderness, guarding or limited movement
H. Neurologic exam
NORMAL VITAL SIGNS IN THE PEDIATRIC AGE GROUP
AGE
PULSE
RESPIRATIONS
BLOOD PRESSURE
avg./min.
breaths/min.
40-60
40-60
140
Premature
60-80
40-60
150
Newborn
65-105
25-40
140
6 mo
70-110
20-30
135
1 yr
80-110
20-30
110
3 yr
80-110
20-30
100
5 yr
90-115
12-25
90
8 yr
Go to Table of Contents
LAB VALUES
HEMATOLOGY - Red Blood Cells
RBC (Male)
4.2 - 5.6 M/µL
RBC (Female)
3.8 - 5.1 M/µL
RBC (Child)
3.5 - 5.0 M/µL
HEMATOLOGY - White Blood Cells
WBC (Male)
3.8 - 11.0 K / mm3
WBC (Female)
3.8 - 11.0 K / mm3
WBC (Child)
5.0 - 10.0 K / mm3
HEMOGLOBIN
Hgb (Male)
Hgb (Female)
Hgb (Child)
Hgb (Newborn)
14 - 18 g/dL
11 - 16 g/dL
10 - 14 g/dL
15 - 25 g/dL
HEMATOCRIT
Hct (Male)
Hct (Female)
Hct (Child)
MCV
MCH
MCHC
neutrophils
bands
lymphocytes
monocytes
eosinophils
basophils
39 - 54%
34 - 47%
30 - 42%
78 - 98 fL
27 - 35 pg
31 - 37%
50 - 81%
1 - 5%
14 - 44%
2 - 6%
1 - 5%
0 - 1%
CARDIAC MARKERS
troponin I
troponin T
myoglobin (Male)
myoglobin (Female)
GENERAL CHEMISTRY
acetone
albumin
alkaline phosphatase
anion gap
ammonia
amylase
AST,SGOT (Male)
AST,SGOT (Female)
Go to Table of Contents
0 - 0.1 ng/ml (onset: 4-6 hrs, peak:
12-24 hrs, return to normal: 4-7 days)
0 - 0.2 ng/ml (onset: 3-4 hrs, peak:
10-24 hrs, return to normal: 10-14 days)
10 - 95 ng/ml (onset: 1-3 hrs, peak:
6-10 hrs, return to normal: 12-24 hrs)
10 - 65 ng/ml (onset: 1-3 hrs, peak:
6-10 hrs, return to normal: 12-24 hrs)
0.3 - 2.0 mg%
3.5 - 5.0 gm/dL
32 - 110 U/L
5 - 16 mEq/L
11 - 35 µmol/L
50 - 150 U/dL
7 - 21 U/L
6 - 18 U/L
bilirubin, direct
bilirubin, indirect
bilirubin, total
BUN
calcium (total)
carbon dioxide
carbon monoxide
HDL (Male)
HDL (Female)
iron
iron binding capacity
lactic acid
lactate
lipase
magnesium
osmolarity
parathyroid hormone
phosphorus
potassium
SGPT
sodium
T3
thyroglobulin
thyroxine (T4) (total)
total protein
TSH
urea nitrogen
uric acid (Male)
uric acid (Female)
0.0 - 0.4 mg/dL
total minus direct
0.2 - 1.4 mg/dL
6 - 23 mg/dL
8 - 11 mg/dL
21 - 34 mEq/L
symptoms at greater than or equal to 10%
saturation
96 - 112 mEq/L
0.2 - 0.6 mg/dL
0.6 - 1.0 mg/dL
0.6 - 1.5 mg/dL
0 mg%; Coma:
greater than or equal to 400 - 500 mg%
2.0 - 21 ng/mL
65 - 99 mg/dL
(diuresis greater than or equal to 180 mg/dL)
25 - 65 mg/dL
38 - 94 mg/dL
52 - 169 µg/dL
246 - 455 µg/dL
0.4 - 2.3 mEq/L
0.3 - 2.3 mEq/L
10 - 140 U/L
1.5 - 2.5 mg/dL
276 - 295 mOsm/kg
12 - 68 pg/mL
2.2 - 4.8 mg/dL
3.5 - 5.5 mEq/L
8 - 32 U/L
135 - 148 mEq/L
0.8 - 1.1 µg/dL
less than 55 ng/mL
5 - 13 µg/dL
5 - 9 gm/dL
Less than 9 µU/mL
8 - 25 mg/dL
3.5 - 7.7 mg/dL
2.5 - 6.6 mg/dL
LIPID PANEL (Adult)
cholesterol (total)
cholesterol (HDL)
cholesterol (LDL)
triglycerides (Male)
triglycerides (Female)
Less than 200 mg/dL desirable
30 - 75 mg/dL
Less than 130 mg/dL desirable
Greater than 40 - 170 mg/dL
Greater than 35 - 135 mg/dL
URINE
color
specific gravity
pH
Straw
1.003 - 1.040
4.6 - 8.0
chloride
creatine (Male)
creatine (Female)
creatinine
ethanol
folic acid
glucose
Return to Table of Contents
Na
K
C1
protein
osmolality
10 - 40 mEq/L
Less than 8 mEq/L
Less than 8 mEq/L
1 - 15 mg/dL
80 - 1300 mOsm/L
24 HOUR URINE
amylase
calcium
chloride
creatinine
creatine clearance (Male)
creatine clearance (Male)
creatine clearance (Female)
creatine clearance (Female)
magnesium
osmolality
phosphorus
potassium
protein
sodium
urea nitrogen
uric acid
250 - 1100 IU / 24 hr
100 - 250 mg / 24 hr
110 - 250 mEq / 24 hr
1 - 2 g / 24 hr
100 - 140 mL / min
16 - 26 mg / kg / 24 hr
80 - 130 mL / min
10 - 20 mg / kg / 24 hr
6 - 9 mEq / 24 hr
450 - 900 mOsm / kg
0.9 - 1.3 g / 24 hr
35 - 85 mEq / 24 hr
0 - 150 mg / 24 hr
30 - 280 mEq / 24 hr
10 - 22 gm / 24 hr
240 - 755 mg / 24 hr
COAGULATION
ACT
APTT
platelets
plasminogen
PT
PTT
FSP
fibrinogen
bleeding time
thrombin time
90 - 130 seconds
21 - 35 seconds
140,000 - 450,000 /ml
62 - 130%
10 - 14 seconds
32 - 45 seconds
Less than 10 µg/dL
160 - 450 mg/dL
3 - 7 minutes
11 - 15 seconds
CEREBRAL SPINAL FLUID
appearance
glucose
osmolality
pressure
protein
total cell count
WBCs
clear
40 - 85 mg/dL
290 - 298 mOsm/L
70 - 180 mm/H2O
15 - 45 mg/dL
0 - 5 cells
0 - 6 / µL
HEMODYNAMIC PARAMETERS
cardiac index
cardiac output
left ventricular stroke work index
right ventricular stroke work index
mean arterial pressure
2.5 - 4.2 L / min / m2
4 - 8 LPM
40 - 70 g / m2 / beat
7 - 12 g / m2 / beat
70 - 105 mm Hg
Return to Table of Contents
pulmonary vascular resistance
155 - 255 dynes / sec / cm to the negative 5
pulmonary vascular resistance index 255 - 285 dynes / sec / cm to the negative 5
stroke volume
60 - 100 mL / beat
stroke volume index
40 - 85 mL / m2 / beat
systemic vascular resistance
900 - 1600 dynes / sec / cm to the negative 5
systemic vascular resistance index 1970 - 2390 dynes / sec / cm to the negative 5
systolic arterial pressure
90 - 140 mm Hg
diastolic arterial pressure
60 - 90 mm Hg
central venous pressure
2 - 6 mm Hg; 2.5 - 12 cm H2O
ejection fraction
60 - 75%
left arterial pressure
4 - 12 mm Hg
right atrial pressure
4 - 6 mm Hg
pulmonary artery systolic
15 - 30 mm Hg
pulmonary artery diastolic
5 - 15 mm Hg
pulmonary artery pressure
10 - 20 mm Hg
pulmonary artery wedge pressure 4 - 12 mm Hg
pulmonary artery end diastolic pressure
8 - 10 mm Hg
right ventricular end diastolic pressure
0 - 8 mm Hg
NEUROLOGICAL VALUES
cerebral perfusion pressure
intracranial pressure
70 - 90 mm Hg
5 - 15 mm Hg or 5 - 10 cm H2O
ARTERIAL VALUES
pH
PaCO2
HCO3
O2 saturation
PaO2
BE
7.35 - 7.45
35 - 45 mm Hg
22 - 26 mEq/L
96 - 100%
85 - 100 mm Hg
-2 to +2 mmol/L
VENOUS VALUES
pH
PaCO2
HCO3
O2 saturation
PaO2
BE
7.31 - 7.41
41 - 51 mm Hg
22 - 29 mEq/L
60 - 85%
30 - 40 mm Hg
0 to +4 mmol/L
Return to Table of Contents
12 LEAD EKG LANDMARKS & INFARCT PATTERNS
V1 - 4th ICS, R sternal border
V2 - 4th ICS, L sternal border
V3 - Midway between V2 and V4
V4 - 5th ICS, Left MCL
V5 - Follow V4 in a straight line to
the anterior axillary line.
V6 - Follow V4 and V5 to mid- axillary
line.
RA = Right Arm
LA = Left Arm
RL = Right Leg
LL = Left Leg
Locations of Infarcts
Inferior wall
Anterior wall
Anteroseptal
Anterolateral
Lateral wall
Return to Table of Contents
II, III, aVF
V1, V2, V3, V4, V5, V6
V1, V2, V3, V4
V3, V4, V5, V6
I, aVL, V5, V6
Clinical Division
Standard Operating Procedure
Effective Date: February 01, 2008
DOCM_______HR_______
Approval:
Policy: BLS Transport Utilization
Objective: To provide clear standards for the proper utilization of BLS
ambulances to transport patients in the 911 system.
Scope: Clinical Director, Clinical Manager, Team Leaders, Field
Instructors, Paramedics, EMT-Basics
Procedure: 1. A Pridemark paramedic will respond to all 911 calls as the primary responder
and perform a full ALS examination to determine the type of care that is
required. Certain vital signs will be disqualifiers for BLS transport.
a. Blood Pressure below 100 systolic
b. A heart rate in excess of 108/min.
c. A respiratory rate in excess of 30
d. Altered mental status of unknown etiology
i. AMS due to dementia is acceptable as long as it is not below
patient baseline
ii. AMS due to alcohol is acceptable as long as the patient is not
obtunded or in need of airway support. A good benchmark would
be the ability to ambulate with minimal assistance.
iii. Co-ingestion of drugs and alcohol is a disqualifier for BLS
e. Poor skin signs
2. If the patient is determined to need ALS monitoring, ALS procedures, or has the
potential for deterioration, a Paramedic will attend during transport to the
hospital. If ALS treatment is initiated by the Paramedic, then transport will be
continued by ALS.
3. ALS transport of patients that have been excluded from BLS care can be handled
in one of two ways:
a. If the responding Paramedic is a member of an ALS ambulance, they will
continue to take the patient in their ambulance and initiate transport.
b. If the responding Paramedic responded on a supervisor vehicle, the
paramedic can assume the attendant role in the BLS ambulance which is
possible because all vehicles are equipped as standard ALS units.
4. All attendants from BLS units that can be utilized in the 911 system will have
successfully completed a field instruction program. This will ensure that they
will be able to provide care at the same level as an EMT working on a standard
Pridemark ALS unit.
Return to Table of Contents
5. If during transport the patient deteriorates and develops vital signs that exceed
the initial transport criteria, Base Contact will be initiated and ALS will be called
in to complete transport if appropriate.
6. Use of the BLS transport model will be restricted to urban areas within 15
minutes or less transport time to a hospital and per individual contract
requirements.
Return to Table of Contents
Clinical Division
Standard Operating Procedure
Effective Date: January 31, 2008
Approval: DOCM_______HR_______
Policy: Controlled Substances
Objective: To clearly identify the process and responsibilities for storage,
administration, and restocking of controlled substances as required by
state and federal law
Scope: Clinical Director, Clinical Manager, Team Leaders, Field
Instructors, EMT-Paramedics
Procedure:
General Principles
Controlled substances, drugs that come under the jurisdiction of the Federal Controlled
Substances Act of 1970, are drugs that have a high risk for misuse or abuse by patients,
professionals, and the public. The Drug Enforcement Administration (DEA) administers
The Federal Controlled Substances Act. Because of the high potential for abuse,
controlled substances have special requirements for ordering, receiving, storing, and
administering. Very strict security and record-keeping is mandatory. The Clinical Director
is responsible for overseeing the entire process and ensuring that security remains high.
Anytime there is a suspected breech in security, the Director of Clinical Medicine must
be notified immediately. A thorough investigation is mandatory. If criminal activity is
suspected, law enforcement officials and the DEA must be notified immediately.
Pridemark Paramedic Services/Medical Director must maintain a current DEA license.
The DEA license is registered under Pridemark Paramedic Services with the Medical
Director also listed on the license and shall be held by the Director of Clinical Medicine.
Procedure
Ordering Controlled Substances
Schedule II Controlled Substances
Include Fentanyl and Morphine
Schedule II Substances must be ordered on an Official US DEA Order Form (DEA-222).
The order must be entered on the DEA-222 Tracking Record and a copy of the DEA-222
form must be kept on file and tracked. Include on the tracking record the Form 222 #, the
order form #, the item ordered, quantity ordered, date ordered, date received, and
quantity received.
Schedule IV Controlled Substances
Include Valium (Diazepam), and Versed (Midazolam)
Schedule IV Substances may be ordered directly from the supplier without an Official US
DEA Order Form.
Invoices must be kept on file and tracked.
Storing Controlled Substances
All controlled substances must be handled with the highest security.
All controlled substances will be placed in the Clinical Director’s safe immediately upon
receipt.
Return to Table of Contents
All controlled substances coming into or going out of the Clinical Director’s safe must be
logged on the Clinical Director’s Narcotic Log. The safe count must be reconciled with
every transaction.
The flow of controlled substances shall be as follows:
The Clinical Director will initially secure all controlled substances.
a) Controlled substances will then be distributed to the
appropriate divisions as needed to replace used stock.
Controlled substances shall be kept in the Team Leaders’ safe. All controlled substances
coming into or going out of the Team Leaders’ safe must be logged. The safe count
must be reconciled with every transaction.
iv. Using Controlled Substances during the shift:
a. At the beginning of the shift, the paramedic or RN shall access the
controlled substances cabinet and sign out an intact box.
b. At the end of the shift, or during the shift if call volume requires, the
box is returned to the cabinet with the appropriate documentation if
substances have been used and the box appropriately handled. A
witness must verify the procedure.
c. Should a narcotic box be used or unsealed, it shall be placed in the
lower locker cabinet with proper documentation rubber banded around
box.
v. The sealed controlled substances boxes must be kept in a locked cabinet
in each ambulance. Each ALS provider shall be issued a combination
lock which can be custom coded for this purpose. This code shall not be
shared with others.
e. Tamper controls
i. The controlled substance box should remain in the heat-sealed plastic
until use, and the plastic unique lock should remain attached to the box.
ii. Each individual controlled substance container, vial or pre-load, also has
a tamper seal. As soon as the tamper has been broken, the entire
contents of the container should be drawn up and prepared for use.
a) Should no controlled substance be given, the medication should be
wasted and properly documented with a witness signature. Said
witness may be EMT partner.
b) Should a container be discovered with the tamper seal missing, the
Team Leader shall be notified as soon as possible and the container
not used.
i) An IR regarding the circumstances surrounding the missing
tamper shall be filed.
Administration of Controlled Substances
Controlled substances must be administered according to Pridemark Protocols, Policies,
and Procedures.
The only time that a controlled substance may be administered out of compliance with
the protocols is when a direct order is given from a base hospital physician (see
Operational Guidelines—Base Physician Consultation).
Any time a paramedic administers a controlled substance, the paramedic must complete
a Patient Care Record and a “Controlled Substance Storage and Administration
Record.”
Documentation of Controlled Substance Usage
All controlled substance usage shall be documented in the PCR. The controlled
substance may be documented using either the generic or trade name. Initials or
abbreviations should not be used.
A Controlled Substance Storage and Administration Record (SAR) shall also be filled out
for every usage or waste.
Return to Table of Contents
The original SAR should be attached to the narc box with a rubber band and placed with
the box in the lower locked cabinet for Team Leader restock.
Exchange of Controlled Substances
After any usage or waste, the box and documentation shall either be turned in directly to
the Team Leader, or returned to the controlled substances cabinet.
The Team Leader will restock used controlled substances by turning over all Patient
Care Records/Administration Record Forms to the Director of Clinical Medicine once per
month. The Director of Clinical Medicine will also keep records of all controlled
substances used and related information to include:
Date Replaced
Substance
Trip Number
Patient Name
Patient Date of Birth
Dosage Administered
Dosage Wasted
Administered By
Employee Number
Serial Number
Return to Table of Contents
EMT
Field Instruction
Program
Purpose: To outline the field orientation process in an effort to create an
effective and consistent training program for new Pridemark EMT’s.
Scope: Team Leaders, Field Instructors, & EMT’s
Description: The EMT Field Instruction program shall consist of five stages.
The following is merely a guide and may at the discretion of the Clinical Manager
or Administration be custom tailored to meet individual employee or operational
needs.
Phase I:
Classroom Orientation
Phase II:
Third Rides
Phase III:
Para-transit
Phase IV:
Operations
Phase V:
Medical
Details:
Phase I: Phase I shall consist of general classroom orientation to Pridemark.
This includes but is not limited to Human Resource policies, benefits, and
mandatory new employee training. It shall also include system specific training in
mapping, radios, and paperwork. Phase I will be managed and administered by
the Human Resources Staff, in coordination with the Directors of Operations,
Risk, Customer Service, and Clinical Managers.
Phase II: Phase II shall consist of 3rd rides with Pridemark Paramedic EMT’s.
This phase in intended to introduce the new employee to Pridemark Para-transit
operations and prepare them for Phase III where they will operate as the sole
crew member on Para-transit. During Phase II, the new employee shall be
oriented on radio operations, mechanical wheel chair lift usage, securing
patients, mapping, and general Para-transit operations and expectations. The
Return to Table of Contents
new EMT should also be oriented on all patient care equipment and van
inventory.
Phase III: While working independently on Para-transit, the new EMT should
focus on mastering general operational aspects of working at Pridemark to
prepare them for future BLS and eventually ALS roles. Specifically, the new
EMT should learn the system specific street rotations, mapping, hospital and
SNF locations around the district, radio etiquette, and general operational
expectations such as proper care of vehicles and equipment. Questions and
help during this phase should be solicited from peers, Team Leaders, Field
Instructors, and management as needed.
It is expectation that time on Para-transit will allow the new EMT to learn partially
thru the example of others, and partially thru self study. Some self initiative and
motivation are required during this phase to be successful. Historically, the best
EMT’s and Medics in the company have started in Para-transit. Most all will tell
you that it was a valuable learning opportunity.
At regular intervals thru out the year, which shall be available by going to the
education calendar on line at www.Pridemark.net Pridemark shall offer EMT FI
testing. This testing process shall serve to rank EMT’s for entry into the BLS and
ALS systems and further Field Instruction. The testing will be based on much of
what is expected during Phase III. A prerequisite to this testing shall also be the
completion of an approved IV therapy course. Basic EKG class is also strongly
recommended.
It is the goal that people transition from Para-transit to BLS only after going thru
Field Instruction with an EMT FI. However, at times, operational needs may
necessitate moving people sooner. In such cases every attempt will be made to
FI EMT’s as soon as possible. It may at times also be necessary to place people
in FI out of ranking order, as may be necessary to facilitate scheduling or
operational needs of the company or individual employees who may not be able
to participate in FI due to schedule conflicts, etc.
Phase IV: Once selected and placed into Field Instruction with an EMT or
Paramedic Field Instructor you will be given one week to complete phase IV.
Phase IV shall introduce the aspects of scene management and operations.
Additional time may be granted at the discretion of the Clinical Manager and
Operations.
During this phase emphasis shall be placed on the following:
• Customer Service & Communication (Pt’s, Fire, Hospital, everyone we
meet)
• Scene Management & Safety
• Driving & Vehicle operations
• Radio Operation & Etiquette
• Mapping and Routing
• Working as a team
Return to Table of Contents
•
•
Observation of how the EMT functions in ALS
Protocol Review
Phase V: Phase V shall focus on your Medical roles as an EMT with Pridemark
and build on what was learned in Phase IV. This phase shall be completed
within one week. Additional time may be granted at the discretion of Clinical
Management and Operations.
During this phase emphasis shall be placed on the following skills:
• Assessment of the BLS and ALS patient.
• Obtaining accurate Vital Signs
• Developing BLS treatment plans
• IV Therapy (Canulation, proper priming of various IV tubing such as Micro,
Macro, Blood tubing, & Buretrols, and knowing when each is appropriate)
• Monitor usage (4 & 12 lead EKG placement)
• Documentation of Patient Care
The EMT will successfully pass this phase and be cleared for ALS with the
approval of the Field Instructor or Clinical Manager and successful completion of
the Final EMT Protocol test. The Field Instructor will then complete the
recommendation for action form and return it to the Clinical Manager for
processing.
While the EMT is now clear to work in the BLS and ALS system, this does not
guarantee scheduling in the BLS or ALS system. Scheduling shall be based
solely on operational needs and policy.
Return to Table of Contents
Clinical Division
Standard Operating Procedure
Effective Date: January 31, 2008
Approval: DOCM_______HR_______
Policy: Paramedic FI Process
Objective: To clearly identify the training process for Paramedics to
function independently in the Pridemark system.
Scope: Clinical Director, Clinical Manager, Team Leaders, Field
Instructors, EMT-Paramedics
Description: The Paramedic Field Instruction program shall consist of five
stages. The following is merely a guide and may at the discretion of the Clinical
Manager or Administration be custom tailored to meet individual employee or
operational needs.
Phase I:
Classroom Orientation
Phase II:
3rd Rides
Phase III:
Medical
Phase IV:
Driving/Operations
Phase V:
Independent Probation
Return to Table of Contents
Details:
Phase I: Phase I shall consist of general classroom orientation to Pridemark.
This includes but is not limited to Human Resource policies, benefits, and
mandatory new employee training. Phase I will be managed and administered
by the Human Resources Staff, in coordination with the Directors of Operations,
Risk, Customer Service, and Clinical Managers.
Phase II: Phase II shall consist of 3rd rides with Pridemark Paramedic Field
Instructors. This phase in intended to introduce the new employee to Pridemark
operations and prepare them for Phase III where they will operate as the 2nd crew
member on a two person ambulance (2 UP). During Phase II, the new employee
shall be oriented on radio operations and mapping. The new Paramedic should
also be oriented on all patient care equipment and ambulance inventory.
During this phase the new Paramedic should successfully pass the mapping and
radio test. The new Paramedic should also be proficient in map reading. While
not being expected to know the entire district at this point, it is expected they be
able to locate calls and provide effective verbal navigation cues to the partner
driving. This phase is also designed to evaluate the new employees learning
style and develop and effective plan for 2 Up Field Instruction.
The new Paramedic shall also attend on all Calls. However, the goal of this
phase is to prepare for 2 up Field Instruction. Fine tuning of Medicine shall be
the goal of Phase 3. During phase 2 we merely want to assure that the new
Paramedic is competent to practice medicine under indirect supervision. The
focus should be on global type medical issues, for instance the things we won’t
be able to observe in the two up phase.
Phase III: Phase 3 is the medical phase. The Probationary Paramedic will be
tasked with attending to all patient care (ALS & BLS) and developing treatment
plans. Such treatment plans shall be verbally discussed with the Field Instructor
and agreed upon prior to departure from the scene. Changes enroot should be
verbally discussed with the FI and/or medical control and appropriate changes
made as needed to the original care plan. All trips should be constructively
critiqued after the call.
Phase 3 shall also serve to allow the new Paramedic to learn the geography of
the district, locations and best routes to all hospitals served. It shall be the
discretion of the FI as to whether or not to allow driving to calls and around the
district. The new Paramedics learning style should be taken into account when
making this decision. The new Paramedic should also work on mapping,
developing skills to find the quickest route to calls and facilities.
During this phase the new Paramedic shall successfully complete the Cardiology,
and Procedural Sedation tests.
Return to Table of Contents
*The new Paramedic, being Colorado State Certified, shall be presumed to be
capable of attending any and all patients during this phase unless the Paramedic
consistently performs to the contrary, in which case consultation with the Clinical
Manager is advised.
Phase IV: Phase 4 shall concentrate on driving and Pridemark operations.
During this phase the new Paramedic should be able to safely and effectively
navigate to and from calls. Additionally, the Field Instructor should attempt to
function at the BLS level to simulate what the new Paramedic can expect once
cleared. During this portion, the new Medic shall attend on all ALS calls and
determine which calls are appropriate to delegate to the FI acting in a BLS role.
The FI shall continue to critique each call after it’s conclusion to assure continued
learning and evolution in the program.
The new Paramedic should successfully complete the operations and final
protocol test during this Phase.
Phase V: The new Paramedic is cleared for independent duty. The new
Paramedic shall continue to be considered in orientation until the completion of
the 90 day probationary Period. During this phase the new Paramedic will
undergo 100% chart review via the Clinical Manager, be assigned self study
modules and also participate and present at M&M’s.
The 90 day probationary period may be extended at the discretion of Human
Resources and Administration if needed. The new Paramedic may also be
partnered with an EMT FI if additional operational orientation is needed.
Return to Table of Contents
Target Timeline:
In an effort to set motivational goals for the new Paramedic, the following
timelines shall be used as targets to complete each phase. For the purpose of
these timelines each new Paramedic shall be placed in one of three categories.
New Paramedic
Any Paramedic with less than one year experience running as a Paramedic in a
911 system.
New Company Paramedic
Any new Paramedic who was working for Pridemark full-time as an EMT prior to
completion of Paramedic School. These individuals should have at least 6
months experience with Pridemark to fall into this category or be ALS cleared.
Experienced Paramedic
Any Paramedic with more than one year experience running as a Paramedic in a
911 System.
Phase I Timeline:
New Medic:
5Days
Company Medic:
5Days
Experienced Paramedic: 5Days
Phase II Timeline:
New Medic:
4 Weeks
Company Medic:
4 Week
Experienced Paramedic: 2 Weeks
Phase III Timeline:
New Medic:
8 Weeks
Company Medic:
6-8 Weeks
Experienced Paramedic: 3 Weeks
Phase IV Timeline:
New Medic:
2 Weeks
Company Medic:
1 Week
Experienced Paramedic: 1-2 Weeks
Phase V Timeline:
New Medic:
Completion of 90 Days
Company Medic:
Completion of 90 Days
Experienced Paramedic: Completion of 90 Days
Return to Table of Contents
Clinical Division
Standard Operating Procedure
Effective Date: August 29, 2007
Approval: DOCM_______HR_______
Policy: Certifications
Objective: To clearly identify the process and responsibilities of
employees as it relates to the obtaining, maintaining, and tracking of all
required certifications.
Scope: Clinical Director, Clinical Manager, Team Leaders, Field
Instructors, RN’s, EMT-Paramedics, EMT-Basics
Procedure:
A. It is the responsibility of all clinical employees’ (EMT-B, EMT-I, EMT-P,
RN’s) to maintain all required certifications.
a. Required Certifications/license:
i. State EMT-B, I, Paramedic, or RN License
ii. NREMT (EMT’s and Medics only) certification with 12
months of hire date
iii. CPR (AHA or ASHI)
iv. ACLS ( AHA or ASHI) for RN’s and Paramedics
v. PALS or PEPP for RN’s and Paramedics with 6 months of
hire
vi. NIMS ICS 100,200, 300, 400, 700, & 800 as appropriate for
position. ICS 100 & 700 are required at a minimum for all
clinical employees
B. Two copies (front and back) of all required certifications shall be provided
to the Clinical Director.
a. The Clinical Director shall provide one copy to the Communication
Center for entry into CAD.
b. The Clinical Director shall maintain the other copy for placement in
the employees’ clinical file.
c. To avoid lapses, all certifications shall be turned in prior to the
expiration date to allow adequate time for entry into CAD. 1 week
minimum
C. All clinical employees seeking continuing education and in house
certifications must have a current Clinical Education Application on file.
(Available from Clinical Manager)
D. Employees seeking assistance with re-certification shall abide and agree
with the following:
a. As a courtesy, Pridemark Paramedics will assist employees who
participate in our Clinical Education Program with re-certification of
State and National Registry certifications. Such assistance shall be
limited to providing guidance on the application process, providing
Return to Table of Contents
copies of CE records, and signing of required documents for recertification should the employee meet the requirements.
b. All such requests for assistance with recertification must be made
in writing or via email to the Director of Clinical Medicine well in
advance of expiration dates. In general, it can take three months to
process some re-certifications for in state candidates and in some
cases longer from the date the application is submitted to the state.
i. Applicants shall allow one month for processing of requested
assistance and preparation of applications for submittal.
ii. Once the above is processed, applicants shall be
responsible for submittal of certification applications to the
State or National Registry.
iii. In summary, as a general rule of thumb all requests for recertification should be submitted four months prior to
expiration.
1. Example: If your National Registry expires March
31st, 2008, you should request assistance from the
Director by December 1st, 2007 and they will have
their portion of your application completed by
December 31st, and returned to you to deliver.
c. Employees seeking such assistance shall obtain at least 50% of CE
in house by PPS.
i. The Clinical Division shall offer regular monthly CE and
annual re-certification classes in BLS, ACLS and PALS or
PEPP
ii. Such CE shall be posted on www.Pridemark.net on the
education calendar.
iii. Application and RSVP may be required for certain courses.
d. Pridemark Paramedics shall assume no responsibility for lapses in
certifications and any assistance provided is done strictly as a
courtesy. Ultimately, the responsibility of maintaining required
certification is that of the employee.
e. Pridemark Paramedic Services has no control over issues related
to the States handling or processing of certification applications. At
times, the state may take longer than the above timelines to
process applications.
E. The Clinical Manager shall maintain an accurate record of all in house
continuing education and maintain such records for a minimum of four
years in an electronic data base.
a. To obtain copies of CE records, individuals should make a request
in writing or via email to the Clinical Manager and allow up to two
weeks processing time.
F. When attending any in house continuing education, employees must sign
a continuing education roster.
a. The Clinical Manager shall enter rosters in a data base within one
week or receipt.
Return to Table of Contents
b. All rosters along with copies of course outlines must be kept on file
for a minimum of four years. This is in addition to the data base
records.
c. Certificates of Completion for individual courses shall be provided
on specific request only.
Return to Table of Contents
Clinical Division
Standard Operating Procedure
Effective Date: January 31, 2008
Approval: DOCM_______HR_______
Policy: Quality Improvement Guidelines
Objective: To establish guidelines for the routine evaluation of patient care in an
effort to monitor and improve patient care.
Scope: Medical Director, Director of Clinical Medicine, Clinical Manager, Team
Leaders, Field Instructors, EMT-Paramedics, EMT-Basics
Procedure:
A. General Principles
a. The Quality Improvement (QI) process is designed to be a constructive
process.
b. The QI process is the ultimate responsibility of the Medical Director.
c. The Medical Director will work in cooperation with the Director of Clinical
Medicine.
d. The process shall include objective and quantitative tools to track overall
quality of patient care.
e. The process shall generate monthly reports
f. The QI process is a tiered collaborative system that shall include peer
review, management review, and Medical Director review. It shall also
allow for care provider feedback and loop closure.
g. The Medical Director shall have physical and Electronic Access to all
Patient Care Reports (PCR).
B. Process
a. All patient care shall be documented according to Documentation
Requirements.
b. Documentation shall be reviewed for general compliance by the Clinical
Managers.
c. The Clinical Managers will distribute all PCR’s to the Field Instructor
group and/or Medical Director for review.
d. These PCR’s will be distributed via electronic means on flash drives.
e. Each Field Instructor shall be given a flash drive for rotational use, and
each Field Instructor shall be assigned set individuals to monitor on a
continual basis. The purpose of this assignment is to allow the FI’s the
ability to watch for patterns that may develop with individuals.
f. Field Instructors shall review all assigned PCR’s for compliance with
Pridemark Protocols and overall quality of patient care and
documentation.
g. The Field Instructors should follow up directly with individuals on a face to
face basis to provide positive as well as any corrective feedback on
routine QA/QI matters. This should be a constructive process and allow
for two way communication that enables professional growth and
education. This shall not be a disciplinary role.
h. If the Field Instructor notes patterns of deficiencies with an individual or
out of the ordinary protocol violations, the Field Instructor shall report said
cases to the Clinical Manager for further follow up.
Return to Table of Contents
i.
The Field Instructors should report all level I-IV protocol violations to the
Clinical Manager for tracking and possible follow up.
j. The Clinical Managers shall track all Level I-IV protocol violations for
quarterly review.
k. The Clinical Mangers shall report all Level III-IV violations to the Director
of Clinical Medicine as soon as practical.
l. The Director of Clinical Medicine shall review all Level III-IV violations
with the Medical Director as soon as Practical.
m. All Protocol violations will be evaluated on a quarterly basis to review the
need for additional education of protocol changes.
C. The following procedures or events shall be reported to the Director of
Clinical Medicine within 24 hours via email and telephone. The Director shall
then consult with the Medical Director regarding these cases as soon as
possible.
a.
b.
c.
d.
e.
f.
g.
Cricothyroidotomy
Chest Decompression
Esophageal Intubation
Medication errors
Iatrogenic events
Pediatric Cardiac Arrest
Major MCI’s or cases that draw media attention
D. The following qualitative reviews shall be performed on a quarterly basis.
a. Intubation success rates
b. IV success rates
c. Matrix Report
(a) A random sampling of 50 ALS trip reports from each division shall be
reviewed by a minimum of 3 Field Instructors. These charts shall
contain no identifying information regarding the patient or crew
involved.
(b) These trips shall be placed in one of two categories (Agree with care)
or (Disagree with Care) Majority rule will apply to decide which final
category chart shall be placed in.
(c) The Clinical Manager shall facilitate this process and provide the
Director of Clinical Medicine a % of Agree with Care and Disagree
with Care breakdowns.
(d) The Director of Clinical Medicine will compare the reports from all
divisions and provide the Medical Directors, CEO and BOD with the
findings.
(e) This tool will be used to monitor overall quality of care over long
periods.
Return to Table of Contents
Clinical Division
Standard Operating Procedure
Effective Date: January 31, 2008
Approval: DOCM_______HR_______
Policy: Out of Protocol Incidents
Objective: To provide guidelines for situations when out-of-protocol incidents
occur related to Pridemark Protocols, Policies, and Procedures.
Scope: Clinical Director, Clinical Manager, Team Leaders, Field Instructors, EMTParamedics, EMT-Basics.
II. General Principles
Adherence to medical and procedural protocols is paramount to providing optimal patient
care. Initial education and ongoing training help to ensure the knowledge of, and
therefore compliance with, protocols. Our Quality Management Program, Quality Audit
System and Field Evaluation and Training Program are designed to ensure compliance
with the protocols.
There are four levels of Out-of-Protocol Incidents:
Level I Out-of-Protocol Incident: Out-of-protocol incidents that are determined to be
appropriate and are cleared by a physician order and appropriate documentation
Level II Out-of-Protocol Incident: Out-of-protocol incidents that are determined to be
appropriate however it is not cleared by a physician order but appropriate documentation
as to why there was not physician order is included in the Patient Care Record
Level III Out-of-Protocol Incident: Out-of-protocol incident that is determined to be
inappropriate medical care or the omission of appropriate medical care but is non-lifethreatening
Level IV Out-of-Protocol Incident: Out-of-protocol incident that is determined to be
inappropriate medical care or the omission of appropriate medical care and is potentially
life-threatening
Procedure
Anytime field personnel are aware they have operated out-of-protocol, they must fill out
an Incident Report documenting their out-of-protocol incident and the reasons for going
out-of-protocol. The Clinical Manager will review these and route these to the Director of
Clinical Medicine as appropriate.
Out-of-protocol incidents will be monitored via the Quality Management Program/Quality
Audit System and by feedback from hospital or field personnel. In those cases where an
out-of-protocol incident is discovered via the Quality Management Program, the
individuals involved will be asked to write an Incident Report to describe their reasoning
for going out-of-protocol.
The out-of-protocol level will be determined and disposition, including education,
trending, and/or discipline will be handled according to the level.
Level I Out-of-Protocol
Return to Table of Contents
there was not physician order is included in the Patient Care Record) will be handled in
the following manner:
The case will be discussed with the personnel involved and appropriate education will be
given.
The out-of-protocol incident will be trended.
No discipline is indicated.
Level III Out-of-Protocol (out-of-protocol incident that is determined to be inappropriate
medical care or the omission of appropriate medical care but is non-life-threatening) will
be handled in the following manner:
The case will be handled via the standard quality management process,
however, must be reported to the Director of Clinical Medicine and Clinical
Manager. Appropriate education and trending are necessary to ensure
personnel learn from the situation and repeat episodes are minimized.
Discipline will be handled on a case by case basis but may include
suspension and/or termination depending on severity and/or history of similar
violations at the discretion of the Director of Clinical Medicine in consultation
with the Director of Operations, Human Resources, and Medical Director.
Level IV Out-of-Protocol (out-of-protocol incident that is determined to be inappropriate
medical care or the omission of appropriate medical care and is potentially lifethreatening) will be handled in the following manner:
The case will be referred to the Director of Clinical Medicine who will meet
with the personnel involved. Appropriate education and follow up evaluation
prior to return to duty is necessary to ensure personnel learn from the
situation and repeat episodes are minimized. Discipline will be handled on a
case by case basis but may include suspension and/or termination depending
on severity and/or history of similar violations at the discretion of the Director
of Clinical Medicine in consultation with the Director of Operations, Human
Resources, and Medical Director.
Return to Table of Contents
Clinical Division
Standard Operating Procedure
Effective Date: January 31, 2008
Approval: DOCM_______HR_______
Policy: Paramedic School Sponsorship
Objective: To provide guidelines for the sponsorship and recommendation
of Pridemark EMT-Basics to attend Paramedic School.
Scope: Clinical Director, Director of Operations, Clinical Manager, Human
Resources, Team Leaders, EMT-Basics.
Process:
General Principles
A. Pridemark Paramedic Services, when possible, will sponsor 2 EMT-Basics
per division per year to attend Paramedic School.
B. Sponsorship shall allow the individual to be eligible for financial
reimbursement, remain eligible for certain benefits without loosing seniority, and
scheduling assistance to continue working on a limited basis or take time off to
attend school without loss of seniority.
1. Sponsored employees shall be responsible for full payment of health
insurance premiums while in school should they choose to continue
coverage.
2. Such payments shall be for the full premium amount (both employee
and company contribution)
3. Full payment shall be made the first of each month to remain on
benefits.
C. Financial tuition reimbursement shall be paid in two installments at one year
intervals following successful completion of Paramedic school and Pridemark
Paramedic Field Instruction. To be eligible, the sponsored employee must
maintain uninterrupted full time status for two years following graduation. Current
total reimbursement is $5000, paid as above in $2500 installments.
D. This program is intended to encourage continued full time employment with
Pridemark Paramedic Services after completion of paramedic school. It is also
the intent of this program to encourage all EMT-Basics to attend Paramedic
School.
E. Those individuals not eligible for sponsorship may qualify for
recommendation.
F. Recommendation shall allow the employee to obtain written recommendation
as may be required for certain Paramedic programs. However, recommendation
does not guarantee a Paramedic Position will be available upon graduation, not
does it guarantee the maintenance of seniority or assistance with scheduling.
II. Sponsorship Process
A. Bi-Annually, two sponsorship positions will be posted utilizing the internal job
posting process.
B. Minimum preferred qualifications will include:
1. One year of experience in ALS system
2. Team Leader and employee recommendation letter
3. IV & EKG certification
I.
Return to Table of Contents
C. The selection process will consist of: (Selection will be based on a
combination of the below process as well job performance. Seniority will only be
taken in to account in the event of a tie.)
1. Panel Interview Process consisting of representatives from:
a) Operations
b) Clinical Department
c) Team Leader Group
2. Written Test
3. Practical Test
III. Recommendation Process
A. Submit written request via email to the Director of Clinical Medicine.
1. You should submit your request at a minimum of two weeks prior to
when it is needed.
2. Enclose the below items and verification with your letter.
B. Obtain a letter of recommendation from your Team Leader as well as one
other employee whom you have worked with.
C. Have one year experience on an ALS ambulance, or one year experience as
an EMT with Pridemark.
Return to Table of Contents
Firefighter Rehab Protocol
Purpose of Firefighter Rehab:
To ensure that the physical and mental condition of personnel operating at a scene of an
emergency or training exercise does not deteriorate to a point that affects the safety of
each member or that jeopardizes the safety and integrity of the operation.
PPS Role:
PPS plays an important role in the rehab process. When an incident occurs – (fire,
hazmat, or clandestine lab breakdown), FD may depend on us to staff and/or operate a
rehab unit for them. To enable us to smoothly integrate with FD and maintain coverage
for the county, the following policies will be followed:
Rehab Group Establishment:
Staff officers will establish a rehab group at any time during an emergency response.
Conditions that will be considered will include: climatic or environmental conditions that
result in heat stress index above 90*F or wind chill index below 10*.
The rehab group has a rehab officer (RO) who is appointed by the Incident Commander
(IC). The RO may be PPS personnel or a firefighter. If you are asked to be the RO, call
the TL to come and take over for you. You will then staff the rehab group.
The RO is in communication with IC and PPS to request additional EMS personnel,
ambulances, request periodic relief for EMS stand-by/rehab crew and other resources as
deemed necessary. RO will obtain forms, equipment and supplies form the IC vehicle.
Those supplies include: Thermometer, fluids and nourishment. Forms and examples are
included in this protocol.
Responsibilities of the RO:
• Obtain rehab materials from the command vehicle
• Establish a rehab area and location
• Check in companies as they arrive, check out companies as they leave rehab
• Be in communication with the IC and PPS to request additional EMS personnel,
ambulances, and other resources as deemed necessary by the situation
• Return completed EIRR and Company Check In/Out sheets to IC
Selecting a rehab site: It should…
• Be far enough away from the scene that personnel may safely remove their
turnout gear and SCBA
• Provide protection form the environment
• Be free of exhaust fumes
• Be large enough to accommodate multiple crews
• Be easily accessible by EMS units
• Allow prompt entry back into the emergency operation
Resources: Supplies for the rehab include the following:
• Fluids (water, sport drinks, etc.)
• Nourishment (broth, soup, granola bars, energy bars, fruit, etc.)
• Medical supplies (thermometers, IV fluids, etc.)
Return to Table of Contents
ED
Return to Table of Contents
Return to Table of Contents
Return to Table of Contents
Tuberculosis Screening Policy Overview
Introduction
Who to Test
Targeted tuberculin testing for latent TB infection (LTBI) is a strategic component of tuberculosis
(TB) control for purposes of identifying persons at high risk for latent TB infection (LTBI) or TB
disease who would benefit from treatment. Targeted tuberculin testing should be conducted only
among groups at high risk and discouraged in those at low risk. Public Health agencies in
Colorado can only provide targeted testing as TB Program resources allow, or if the agency has
alternate funding resources. All testing activities should include a plan for follow-up care of
persons with LTBI or disease and periodic program evaluation.
A local chief medical health officer may conduct required targeted screening programs of
populations who are at increased risk of developing tuberculosis or having LTBI, as defined by
the Centers for Disease Control and Prevention, and offer treatment as appropriate. Such
screening programs shall not be implemented without the prior approval of the local board of
health, state board of health and the state chief medical health officer.
The Mantoux tuberculin skin test (TST), intradermal injection of purified protein derivative
(PPD) is the standard method of identifying persons infected with Mycobacterium tuberculosis
(MTB). Multiple puncture tests (MPTs), such as the Tine test, should not be used. The MPTs
are not reliable because the amount of tuberculin injected intradermally cannot be precisely
controlled. TB skin testing is both safe and reliable throughout the course of pregnancy and
during breastfeeding.
If previous TST results cannot be provided (measured in mm, not “positive” or “negative”), repeat
the test unless there was a severe reaction (e.g. blistering, ulceration, or necrosis) at the
previous site of injection. TB skin retesting should NOT be done if there is appropriate
documentation of a previous positive TST and/or previous treatment for LTBI or active TB.
In general, high-risk groups that should be tested for TB infection include:
• persons with HIV infection/AIDS
• recent close contacts to persons with infectious pulmonary TB disease
• persons with fibrotic lesions on chest x-ray consistent with healed TB
• persons who inject drugs or use other high risk substances, such as crack cocaine, and
alcoholics
• persons with medical conditions which increase the risk of TB disease
• residents and employees of high risk congregate settings such as correctional
institutions, long-term residential care facilities (nursing homes, mental institutions, etc.),
hospitals and other health care facilities, and homeless shelters.
• health care workers and volunteers who serve high risk clients who undergo
employment screening and cannot provide documentation of a previous TST or
information about appropriate follow-up for a “positive” skin test
• mycobacteriology laboratory personnel
• foreign-born persons who have arrived within five years from countries that have a high
TB incidence or prevalence (most countries in Africa, Asia, Latin America, Eastern
Europe, and Russia)
• children less than 4 years of age, or children and adolescents exposed to adults in high
risk categories adult contacts to children with TB infection
• persons with a history of inadequately treated TB
Return to Table of Contents
Pridemark TB Testing Overview
Protocol Overview
1. All Pridemark Employees must provide proof of TB testing within 6 months of their
annual performance evaluation.
2. All new employees must provide proof of TB testing within 12 months prior to
employment and submit to TB testing at time of hire.
3. Any employee that has not had a test within a 12 month period must submit to a 2
stage test.
4. Any employee with a history of previous positive TB test must provide records of the
treatment and be willing to submit to a risk assessment screening and if indicated, an
additional chest x-ray. (see flow chart at the end of this section)
5. Employees with a history of BCG vaccination must also be skin tested and if positive,
referred to employee health for follow up. Subsequent to the initial employee health
referral, risk assessments must be done on an annual basis 6 months prior to
performance evaluation.
6. Any employee that has a positive skin test must submit to appropriate treatment as
deemed necessary by our occupational health provider.
7. Pregnancy does not exempt employees from testing.
8. Failure to comply with these standards poses an unacceptable risk to our patients
and the public at large and may result in suspension from duty or other disciplinary
action.
How to Apply the Tuberculin Skin Test
1. Administer the tuberculin skin test using the Mantoux technique; intradermal injection of
purified protein derivative (PPD). NOTE: Some PPD vial stoppers contain 41.6% latex, which
could pose a concern for those with latex allergy. For those persons who have a latex allergy,
use vials without latex stoppers or remove the stopper prior to drawing up PPD.
Mantoux test procedure
1. Equipment needed: gloves, sharps container, PPD tuberculin (Tubersol or Aplisol),
tuberculin syringe and safety needle, and alcohol pads. NOTE: Opened PPD tuberculin
vials must be dated and discarded after 30 days. Also see package insert for
appropriate storage information.
2. Obtain written consent as per agency requirements
3. Follow infection control procedures, including the use of gloves and a sharps container.
4. Clean the injection site, the upper, outer, lateral aspect of the left forearm 1-2 inches
below the antecubital fossa, with an alcohol pad or alternative skin cleanser (for those
allergic to alcohol). The left forearm is the standard site for TB skin testing.
5. Using a disposable safety needle and syringe, inject 0.1 ml of PPD tuberculin containing
5 TU between the layers of the skin (intradermally) with the needle bevel facing upward.
6. The injection should produce a discrete, pale elevation of the skin (a wheal) 6-10
millimeters (mm) in diameter. NOTE: Repeat the test on the opposite arm or the same
arm, 3 inches from the original site, if a 6-10 mm wheal is not produced.
7. Document location of injection, time and date of injection, dose, name of person who
administered the test, name and manufacturer of tuberculin product used, lot number,
expiration date, and the reason for testing.
How to Read/Measure/Record Test Results
Return to Table of Contents
9. Read the tuberculin skin test 48 to 72 hours after the injection.
10. If the individual fails to show up for the scheduled reading, positive reactions may still
be measurable up to one week after testing.
11. If the results appear negative and more than 72 hours have passed, the test should
be repeated. It can be repeated immediately, or after 1 week if two-step testing is
required (see page 12, “Two Step Tuberculin Skin Testing”).
12. TST results should be read by designated, trained personnel. Do not accept selfreading of TST results.
13. Measure the tuberculin skin test site crosswise to the axis of the forearm.
14. Measure only induration (swelling that can be felt) around the site of the injection. Do
NOT measure erythema (redness). A tuberculin skin test with erythema but no
induration is non-reactive.
15. Record the test result in mm, not as “positive” or “negative.” An exact reading in mm
may be necessary to interpret whether conversions occur on a subsequent test.
Record a tuberculin skin test with no induration as “0 mm.”
16. Adverse reactions to a TST (e.g. blistering, ulcerations, necrosis) should be reported
to the Food and Drug Administration’s Med Watch Program at 1-800-FDA-1088 or via
the Internet at www.fda.gov/medwatch.
17. All licensed hospitals and nursing home facilities must maintain a register of the TST
results of health care workers in their facility, including physicians and physician
extenders who are not employees of the facility but provide care to or have face-toface contact with patients in the facility. The facility must maintain such TST results
as confidential.
In addition:
For persons previously skin tested, an increase in induration of 10 mm within a 2-year period
is classified as a conversion to positive.
1. False negative reactions may be due to:
a. Anergy (see “Anergy Testing”)
b. Recent TB infection (within the past 10 weeks)
c. Very young age (< 6 months of age-because their immune systems are not fully
developed)
d. Overwhelming TB disease
e. Live virus vaccination (see below)
f. Some viral infections (measles, mumps, chickenpox, and HIV)
g. Corticosteroids and other immunosuppressive agents at doses of 2 mg/kg/day or
greater for 2 or more weeks
2. False positive reactions may be due to:
a. Non-tuberculous mycobacteria
b. BCG vaccination
c. Local latex allergic reactions
d. Vaccination with live viruses (e.g. Measles, Mumps, Rubella, Varicella, Oral
Polio, and Yellow Fever) may also interfere with TST reactivity and cause false
negative reactions.
Two-Step Tuberculin Skin Testing (Booster
Phenomenon)
Introduction
Return to Table of Contents
Delayed type hypersensitivity (a skin test reaction) may wane over the years in some people who
are infected with TB. When these people are skin tested many years after infection, they may
have a negative reaction. However, this negative skin test may stimulate (boost) their ability to
react to tuberculin, causing a positive reaction to subsequent tests. This boosted reaction may be
interpreted as new infection. Two-step testing is used to establish a true baseline skin test.
Thus, it is recommended that a baseline two-step tuberculin skin test be performed on workers in
health care facilities, correctional institutions and jails, long term care facilities for the elderly,
homeless shelters, drug treatment centers, residents of long-term care facilities, and other adults
who will be re-tested periodically. Two-step tuberculin skin testing should be performed on these
individuals who cannot document a history of a negative tuberculin skin test within the past year.
Protocol:
1. Apply the tuberculin skin test.
2. If the initial skin test is positive, consider person infected and refer to “What to do After
Interpreting the Skin Test.”
3. If the initial tuberculin skin test is negative: It should be repeated within 1-3 weeks using
the same dose and strength of tuberculin.
4. An individual who can provide documentation of a TST by the Mantoux technique within
the preceding year should have an initial skin test performed, and should be managed
on the basis of that result. There is no need for a second test because the earlier test is,
in effect, the first of a two-step test.
5. If the second test is negative, the individual is classified as uninfected and retested at
routine intervals (two-step testing is not required for subsequent tests unless one or more
years have elapsed since the last test).
6. If the second test is positive, consider person infected and refer to “What to do After
Interpreting the Skin Test”.
BCG (Bacillus Calmette-Guerin) Vaccines
BCG vaccines are live vaccines derived from a strain of Mycobacterium bovis (M. bovis).
Because their effectiveness in preventing infectious forms of TB is uncertain, they are not
recommended as a TB control strategy in the U.S. except under rare circumstances (see below).
They are, however, used commonly in other countries.
Tuberculin Skin Testing of an Individual with a History of BCG
Vaccination
1. A history of BCG vaccination is not a contraindication to tuberculin skin testing if the person is
at risk of exposure to TB.
2. A false positive reaction may occur in persons vaccinated with BCG. However, tuberculin
reactivity caused by BCG vaccination wanes with time and is unlikely to persist > 10 years.
3. A diagnosis of LTBI and the use of therapy should be considered for any BCG-vaccinated
person who has a TST reaction of >10 mm induration, especially if:
•
•
•
the vaccinated person is exposed continually to populations in which the prevalence of TB is
high (e.g., some health care workers, employees and volunteers at homeless shelters, and
workers at drug-treatment centers)
the vaccinated person was born or has resided in a country in which the prevalence of TB is
high; or
the vaccinated person is a contact of another person who has infectious TB, particularly if the
infectious person has transmitted TB to others
Return to Table of Contents
Tourniquet Procedure
Indications
A tourniquet should be used to control potentially fatal hemorrhagic extremity
wounds only after other means of stopping blood loss have failed.
Precautions
1. A tourniquet applied incorrectly can increase blood loss and lead to death or
loss of limb.
2. Applying a tourniquet can cause nerve and tissue damage whether applied
correctly or not.
3. Use on appropriate patients only is of utmost importance.
4. Damage is unlikely if the tourniquet is removed within an hour. Low risk to
tissue is acceptable over death secondary to hypovolemic shock.
5. A commercially made tourniquet is the standard of care as improvised
tourniquets can increase the risk of harm.
Technique
1. Use BSI.
2. Attempt to control hemorrhage using direct pressure, elevation and indirect
pressure on pressure points prior to considering the application of a
tourniquet.
3. If unable to control hemorrhage using above means, apply a tourniquet using
the steps below:
•
•
•
•
•
Cut away any clothing so that the tourniquet will be clearly visible.
The tourniquet should NEVER be obscured by clothing or
bandages.
Apply tourniquet proximal to the wound and not across any joints.
Tighten tourniquet until bleeding stops. **Note: Applying a
tourniquet loosely will only increase blood loss by inhibiting
venous return.
Mark the time and date of application on the patient’s skin next to
the tourniquet. Use a permanent marker.
Keep tourniquet on for full duration of transport. A correctly placed
tourniquet should only removed by the receiving hospital.
Complications
The possibility of the loss of limb, permanent circulatory, and/or neurological damage to
the extremity is very real and should be weighed against the risk of loss of life.
Return to Table of Contents
Therapeutic Induced Hypothermia (TIH)
Overview:
For several decades out of hospital cardiac arrest survival rates have
remained stagnant despite numerous changes in pre-hospital care. Research
published in the New England Journal of Medicine in 2002 as well as the
ILCOR statement in 2003 now show strong statistical evidence that
therapeutic cooling of medical patients of non-hemorrhagic cardiac arrest is
beneficial increasing neurologically intact patient survival rates by 16-23%.
Inclusion Criteria
1. Cardiac arrest secondary to suspected medical causes with no
evidence of traumatic or hemorrhagic causes.
2. Age >16
3. Initial temperature >34c.
Exclusion Criteria
1. Traumatic or hemorrhagic arrest
2. Pregnancy
3. Lack of an advanced airway
Protocol:
1. Patients who meet criteria should receive all traditional treatments as
per existing cardiac arrest protocols & AHA guidelines.
Implementation of the TIH protocol should not delay other therapies.
2. Assure and verify advanced airway (ET tube)
3. Establish two large bore IV’s or IO
4. Remove clothing
5. Obtain temperature if possible
6. Infuse cooled 2-4deg. Celcius saline 40ml/kg rapid IV push with Infuser
if available as soon as inclusion criteria are met. (80 kg patient =
3200ml’s)
7. Upon ROSC
a. MIDAZOLAM (VERSED) 2mg prn, q. 5minute intervals to
control any shivering
b. Maintain hemodynamic stability per current protocols
i. Consider Dopamine/Epi drips
ii. Consider Cordarone
8. Transport to nearest medical facility that supports continuation of TIH
and interventional cardiology.
9. Target patient temperature is 32-34 deg. Celsius
10. Document in PCR to include meeting inclusion criteria
Return to Table of Contents
ETOH Disposition Policy
Overview
The purpose of this policy is to give field crews a guideline to help them ensure for the proper
disposition of calls involving intoxicated parties.
The term intoxicated does not simply mean that an individual has had some alcohol at some point
in the last 24 hours. Tolerance levels differ by age, body type, underlying medical conditions, food
intake, and the amount ingested over time. There are set blood alcohol levels that have proven to
impair judgment and reaction time and are generally accepted by the legal system to determine
the level of intoxication. A blood alcohol level of .05% is considered to be impaired under
Colorado law and .08% is enough for a DUI conviction. In the pre-hospital setting we are not privy
to these types of tests and therefore must make our decision based on clinical assessment and
the use of sound judgment. The point at which a person can be taken against their wishes is
when they have become “Incapacitated by Alcohol”. The legal definition of this condition is
defined as:
C.R.S. 25-1-302 (9) “Incapacitated by alcohol”: means that a person, as a result of the use of
alcohol, is unconscious or has his judgment otherwise impaired that he is incapable of realizing
and making a rational decision with respect to his need for treatment or is unable to take care of
his basic personal needs or safety or lacks sufficient understanding or capacity to make or
communicate rational decisions concerning his person.
Some basic assessment clues for determining the level of intoxication:
Nystagmus
Ataxia (loss of muscle coordination/balance)
Odor of alcohol
Slurred Speech
Irrational behavior
Loud boisterous speech
Understand that apart from the odor of alcohol finding, all of the assessment clues can have a
metabolic cause. Some causes can include hypoglycemia, CVA, hypoxia, hyper/hypothermia,
and hypo-perfusion. ETOH intoxication should be a diagnosis of exclusion in which you are left
with no other reasonable diagnosis.
Protocol
If a patient is found to have ingested alcohol but is not intoxicated, the normal disposition rules
apply. The patient is able to consent to, or refuse treatment or transport.
If a patient is found to be intoxicated there are two possible dispositions:
1. Transport to closest appropriate hospital
2. Turn custody of patient over to someone for transport to a detox facility*
*Note- Transport to a detox facility will only be done by Pridemark units if the call originates from
an emergency department. We DO NOT transport directly to these facilities from the field.
If a patient is determined to be intoxicated and has any of the following the disposition should be
transport to the closest appropriate ED:
1. Visible signs of injury
2. Involvement with high energy transfer event (accident, fall 2x height, assault, etc.)
3. Abnormal vital signs (BP <90 >180, pulse rates <60 or >100, abnormal ecg, abnormal
pulse ox, etc.)
4. New complaints of pain
5. New onset of illness
6. Complaint of exacerbation of current underlying medical condition (COPD worse than
usual, old back problems hurting more than usual, etc.)
7. Unable to stand or walk with minimal assistance
8. Obtunded
Return to Table of Contents
9. Co-ingestion of Rx medication or recreational drugs
10. Psychiatric component (mania, suicidal ideation, hallucinations, etc)
In the absence of these findings in association with the determination that the patient is
intoxicated, the patient may be released for transport to a detox facility like Denver CARES,
Arapahoe House, or the ARC in Boulder. Most often the police are asked to transport patients to
these facilities. If the police cannot or will not transport the patient to a detox facility, the
Pridemark unit will initiate transport to the closest appropriate medical facility. BLS may perform
these transports provided the patient has been cleared by ALS (and only when appropriate for
system status). Outright release of patients that have been determined to be intoxicated is not
appropriate.
Return to Table of Contents