Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
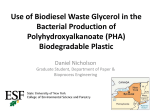
Volume 7 | Issue 5 | May/June 2015 Clinical Consults What’s Your Diagnosis? PATIENT HISTORY SIGNALMENT: “Autumn”, 17 year old spayed female domestic longhair, 6 pounds/2.7 kg. PERTINENT PAST HISTORY: “Autumn” has generally been a healthy geriatric cat. She has received regular annual examinations for the past 3 years and routine preventative care as recommended by her veterinarian. During these past 3 years her owner has reported gradual weight loss despite a good appetite and one pound of weight loss (from 7 to 6 pounds) had been documented by her veterinarian. A heart murmur has also been documented at each annual visit but no further diagnostics had been pursued. During this same time period, “Autumn’s” owner has expressed concerns about her declining vision. See Table 1 for “Autumn’s” laboratory trends and blood pressure measurements over the past 2 years. In May 2012, “Autumn’s” veterinarian documented decreased to absent menace OU and lack of a direct pupillary light response (PLR) in her right eye. A fundic exam revealed a possibly detached retina with floating fibrin strands. “Autumn’s” blood pressure was taken at that time and was within normal limits using an oscillometric device. Clinical Note: Oscillometric devices in cats are less accurate when compared to direct or Doppler measurements. It is easy to obtain inaccurate readings if patient restraint or cuff size and placement are not correct. Table 2 outlines proper blood pressure measurement technique and differences between devices. CRITICAL THINKING ABOUT HYPERTENSION AND HYPOKALEMIA— Chronic Kidney Disease or something more? Donna J. Spector, DVM, DACVIM, Internal Medicine Case materials and images contributed by Dr. Anya Gambino, DVM, DACVECC; VCA Veterinary Specialty Center of Seattle, Lynnwood, Washington PERTINENT PAST HISTORY CONTINUED: “Autumn’s” minimum database was fairly unremarkable but her renal parameters classified her as IRIS Stage 2 CKD. No further follow up was recommended at this time. Clinical Note: Given the presence of renal disease and retinal findings, a recheck blood pressure should have been scheduled (ideally using a Doppler or appropriate cuff and technique) and her bloodwork should have been rechecked in a minimum of 6 months. At her annual exam in May 2013, “Autumn” was found to have an absent menace OU and her left eye had a diminished direct PLR. The fundic exam revealed retinal hemorrhages OU. Her minimum database was repeated and a mild increase of her azotemia was noted with a creatinine increase to 2.2 mg/dL. Her blood pressure was measured again using an oscillometric device but this time she was noted to be hypertensive. Clinical Note: Notice the wide range of blood pressure readings obtained at this visit. This alludes to the inaccuracy of the oscillometric device in small cats like “Autumn.” Referral for both cardiology and ophthalmology consultations was recommended to “Autumn’s” owner in order to further define the status of her vision abnormalities and to identify the nature of her cardiac disease, however, the owner declined referral at this time. Clinical Note: Despite the owner’s unwillingness to seek referral, antihypertensive therapy should have been started to address “Autumn’s” marked hypertension at this time. Thoracic radiographs should have also been performed to obtain general information about cardiac enlargement and the need for additional therapy. No specific therapy or follow up was performed. “Autumn” returned for her annual examination in May 2014 with a history of progressive weight loss and intermittent vomiting. She lacked both menace and PLRs OU. Her fundic examination revealed attenuation of her retinal vessels. Her blood pressure was obtained on a Doppler unit 2014 visits. Clinical Note: A reminder system of doctor and technician follow up calls can help keep owners on track with their recommended recheck schedule. Eight months later “Autumn” presented as an emergency for evaluation of marked weakness and ataxia. On examination, she weighed 5.9 pounds (2.7 kg), her temperature was 97.2 degrees F, a III/VI parasternal systolic heart murmur was noted and blood was detected in the anterior chamber of her left eye. She had significant neurologic abnormalities characterized by marked ventroflexion of the neck, truncal ataxia, head tilt to the right, horizontal nystagmus with fast phase to the left, and right-sided conscious proprioceptive deficits in both thoracic and pelvic limbs. Her and she was noted to be markedly hypertensive with a systolic blood pressure of approximately 220 mmHg. Although her serum creatinine concentration was stable at 2.2 mg/dL, she had a progressive decrease of her urine concentrating ability and her potassium and magnesium were markedly decreased (2.7 and 1.0 mEq/L respectively) which were felt to be consistent with declining renal function. Clinical Note: Serum creatinine is a relatively insensitive marker to monitor progression of early renal disease. The presence of declining urine specific gravity and progressive hypokalemia and hypomagnesemia was thought to be consistent with primary renal failure with excess electrolyte losses. TABLE 1. “AUTUMN’S” ANNUAL MINIMUM DATABASE TRENDS AND ABNORMALITIES Clinical Note: Monitoring trends in laboratory work is critically important! Note the following trends in “Autumn” over 2 years: • Gradually increasing creatinine and decreasing urine specific gravity (IRIS stage 2) • Proteinuria as an early indicator of renal disease • Gradually decreasing potassium and magnesium • Gradually increasing blood pressure 5/2012 5/2013 5/2014 BUN (ref. range: 14-36 mg/dL) 26 28 34 Creatinine (ref. range: 0.6-2.4 mg/dL) 1.8 2.2 2.2 Potassium (ref. range: 3.4-5.6 mEq/L) 3.8 3.5 2.7 Magnesium (ref. range: 1.5-2.5 mEq/L) 1.5 1.4 1.0 CPK (ref. range: 56-529 IU/L) 342 269 663 T4 (ref. range: 0.8-4 ug/dL) 1.7 2.6 2.4 1.040 1.037 1.023 1+ 1+/5.5 mg/dL 1+ Urine specific gravity Proteinuria/Microalbuminuria Blood pressure Systolic 91-130 Systolic 120-263 Diastolic 40-79 Diastolic 75-196 Mean 48-119 Mean 92-217 Oscillometric device Oscillometric device “Autumn” was started on oral potassium supplementation (Tumil-K® tablets, 2 mEq PO BID) to address her severe hypokalemia. Her potassium was rechecked one week later and it had increased to 3.3 mEq/L so she was maintained on this dosage of Tumil-K®. Amlodipine was recommended as an antihypertensive; however, the owner desired a more natural initial approach. A Feliway® pheromone diffuser was instituted and the owner agreed to start amlodipine the following week if “Autumn” remained hypertensive. CURRENT HISTORY “Autumn” was lost to follow up after the May Systolic 218-220 Doppler regular veterinarian referred her immediately to VCA Veterinary Specialty Center of Seattle for further evaluation. “Autumn” was seen through the Neurology Service due to her initial presenting clinical signs and her neuro-anatomic localization was central vestibular. There are many differentials for feline central vestibular disease (see Table 3). After the neurologist reviewed “Autumn’s” medical record with her history of chronic renal failure, untreated hypertension, hypokalemia and hypomagnesemia, a metabolic derangement was suspected to be the most likely etiology of her neurologic signs. “Autumn” was admitted to the hospital and transferred to the Critical Care Service for further evaluation and treatment. DIAGNOSTICS AND ASSESSMENT Upon admission, “Autumn’s” systolic blood pressure was 250-260 mmHg. Bloodwork (see Table 4) was compared to her May 2014 values and revealed progression of her azotemia and further decrease of urine specific gravity. She was markedly hypokalemic, hypomagnesemic, and her CPK was markedly elevated. Together with her clinical signs of cervical ventroflexion, these values were consistent with hypokalemic polymyopathy. Although “Autumn’s” marked hypertension and metabolic derangements could have explained her neurologic signs, a thorough evaluation was warranted due to the severity of her neurologic presentation. Appropriate infectious disease testing was performed. FeLV, FIV and FCV antibody titers were negative. A toxoplasma IgM antibody titer was negative but an IgG antibody titer was positive at 1:128. The elevated IgG titer was suspected to reflect chronic exposure and since the IgM titer—which tends to be positive in cases of active clinical infection—was negative, “Autumn” was not treated for active toxoplasmosis. Clinical Note: Cats presenting with neurologic abnormalities should ideally have a cryptococcus latex antigen sample submitted. Due to “Autumn’s” long-standing heart murmur and hypertension, THREE-VIEW THORACIC RADIOGRAPHS were obtained as an initial evaluation for cardiac disease and to serve as an evaluation for metastasis. The films revealed moderate to marked cardiomegaly (see Figure 1). The cardiac silhouette had a valentine-like appearance with biatrial enlargement on the ventrodorsal view. The cardiac silhouette was tilted cranially on the lateral views and the aortic arch was prominent. No cranial mediastinal masses, FIGURE 1. pulmonary infiltrates or pleural effusion were noted. Mild multifocal spondylosis deformans was noted and there was a mild amount of air and fluid in the esophagus. A follows-up ECHOCARDIOGRAM revealed marked enlargement of the left atrium with no spontaneous echo-contrast noted. There was concentric thickening of the ventricle that was felt to be consistent with hypertension or primary hypertrophic cardiomyopathy. Clopidogrel (Plavix® 18.75 mg PO q day) for clot prevention was the only recommended therapy. The cardiologist recommended extreme caution in regards to fluid administration. TABLE 2. BLOOD PRESSURE MEASUREMENT Systemic hypertension is defined as sustained, high arterial blood pressure • Normal systolic arterial blood pressure (SAP) ranges from 110-160 mmHg • Normal diastolic arterial blood pressure (DAP) ranges from 60-90 mmHg • Normal mean arterial pressure (MAP) ranges from 85-120 mmHg Hypertension is classified based on the risk of target organ (e.g., brain, kidney, eye, heart) damage. The four risk categories developed and set forth in the 2007 ACVIM guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats are as follows: • Risk Category I (minimal): systolic BP <150 mmHg, diastolic BP <95 mm Hg • Risk Category II (mild): systolic BP 150-159 mmHg, diastolic BP 95-99 mmHg • Risk Category III (moderate): systolic BP 160-179 mmHg, diastolic BP 100-119 mmHg • Risk Category IV (severe): systolic BP >180 mmHg, diastolic BP >120 mmHg Diagnosis of systemic hypertension requires measurement of either DIRECT or INDIRECT blood pressure • The gold standard measurement is a DIRECT blood pressure measurement • Made by inserting a needle or catheter into an artery • This provides a highly accurate reading but requires specialized equipment, experience and is not practical for the repetitive measurements necessary for monitoring • Used more in the surgical setting • Due to these limitations, the INDIRECT method of blood pressure measurement is used more commonly • The equipment is readily available and affordable • Experience is necessary to make this technique accurate and repeatable • The DOPPLER and OSCILLOMETRIC methods are most commonly used to measure indirect blood pressure • Regardless of method used, the following criteria must be met for an accurate blood pressure measurement: • Pressure cuff should have a width of 40% of the circumference of the limb or tail • Position the animal so the artery is at the same height as the heart • Patient acclimation for 5-10 minutes in order to reduce anxiety • Discard the first measurement and average 3-7 subsequent readings Doppler Method • Uses ultrasound to detect blood flow through an artery. As the moving blood passes the piezoelectric crystal of the unit a sound is generated • Technique: A piezoelectric crystal transducer is placed over a peripheral artery (e.g., dorsal pedal, palmar, plantar, coccygeal) and ultrasound gel is used to achieve close contact with the skin. A pressure cuff is wrapped around the limb/tail proximal to the transducer and inflated until the audible signal of blood flow is lost. The cuff is slowly deflated until the first sound of blood flood is heard which is recorded as the systolic blood pressure • Diastolic measurements are inaccurate using this method • This technique works very well and many feel is superior to other techniques for blood pressure measurement in cats Oscillometric Method • Measures oscillations in the arterial wall caused by the flow of blood through the artery as a pressure cuff is deflated • Technique: Cuffs have an arrow indicator that should be placed over the artery to be used (e.g., brachial, dorsal pedal, palmar, plantar, coccygeal). The machine is automated and the cuff will be inflated and provide a systolic blood pressure measurement • Diastolic and mean pressure are calculated values. The machine also records pulse rate • Oscillometric readings do not correlate as well as Doppler readings with direct measurements of blood pressure in cats DISCUSSION TABLE 3. COMMON DIFFERENTIALS FOR FELINE CENTRAL VESTIBULAR DISEASE Vascular Ischemic injury—caused by hypertension or thromboembolic disease Non-ischemic or hemorrhagic injury Neoplasia Lymphoma, meningioma, etc. Infectious disease Toxoplasmosis, cryptococcosis, feline infectious peritonitis, bacterial otitis interna to brain stem, etc. Inflammatory disease Granulomatous meningoencephalitis, etc. Metabolic disease Uremia Hypertension Thiamine deficiency Hypokalemia and other electrolyte derangements Primary Hyperaldosteronism Etiology An ABDOMINAL ULTRASOUND was also performed to more fully evaluate “Autumn’s” renal disease and as a metastasis check. Both kidneys were markedly hyperechoic with decreased cortico-medullary distinction and the left kidney was mildly decreased in size. The urinary bladder appeared normal. The gastrointestinal tract, liver, gallbladder, spleen and pancreas were all considered normal. A multi-lobulated hypoechoic mass measuring 2 cm in length x 1.5 cm thick x 2 cm in width was identified in the right cranial abdomen adjacent to the vena cava and encircling the portal vein (see Figure 2). Margins of this mass could not be clearly differentiated from the liver or the right adrenal gland. The right adrenal could not be conclusively identified. The left adrenal was found and felt to be normal in size and shape. This was felt to be consistent with an aldosterone-secreting adrenal mass; with adenoma or carcinoma both being considerations. ADDITIONAL DIAGNOSTICS Hypokalemic polymyopathy Given “Autumn’s” history of hypertension, marked hypokalemia and the abdominal mass found in the area of the right adrenal gland, an aldosterone-secreting mass was suspected. An aldosterone level was submitted for evaluation. The aldosterone level returned one week later and was markedly elevated at >4,572 pmol/L (ref. range 194-388 pmol/L). FIGURE 2. DIAGNOSIS Chronic renal failure Hypertension—with end-organ damage present in eyes, CNS and heart Cardiomegaly—suspect secondary to hypertension or hypertrophic cardiomyopathy Primary Hyperaldosteronism— presumptive aldosteronesecreting adrenal mass TABLE 4. “AUTUMN’S” LABORATORY ABNORMALITIES ON EMERGENCY PRESENTATION 1/2015 BUN (ref. range: 14-36 mg/dL) 55 Creatinine (ref. range: 0.6-2.4 mg/dL) 3.1 Potassium (ref. range: 3.4-5.6 mEq/L) 2.4 Magnesium (ref. range: 1.5-2.5 mEq/L) 1.1 CPK (ref. range: 56-529 IU/L) Urine specific gravity Proteinuria/Microalbuminuria Detailed discussions of chronic renal failure and hypertension are beyond the scope of this article and the reader is referred to the listed references. This report will focus on primary hyperaldosteronism as an increasingly common diagnosis in hypertensive cats. 4,091 1.013 1+/14.3 mg/dL Primary hyperaldosteronism (PHA) has previously been considered a rare endocrine disorder in cats, however, it has likely gone under-recognized in veterinary patients because routine measurement of blood pressure is not performed. Additionally, chronic renal disease is presumed to be the underlying etiology for most cats diagnosed with hypertension and hypokalemia and further diagnostic testing is not pursued. In fact, PHA is the most common adrenocortical disorder in cats and is likely to be an important cause of arterial hypertension in cats just like it is in humans. With improved screening for hypertension and more thorough evaluations, PHA is being diagnosed more commonly in cats. PHA is characterized by excess autonomous secretion of aldosterone from one or both adrenal glands. Aldosterone secretion is normally regulated by changes in extracellular fluid volume and/or pressure (via the reninangiotensin-aldosterone system), as well as potassium concentrations in blood. When physiologically required—such as in response to decreased renal blood flow—aldosterone is secreted from the adrenal gland. Through its actions in the kidney, aldosterone acts to retain sodium and water resulting in volume expansion and increased blood pressure. Aldosterone also enhances excretion of potassium and hydrogen when necessary. Autonomous aldosterone secretion—when there is not a physiologic demand—results in clinical signs referable to systemic hypertension and hypokalemia and is called primary hyperaldosteronism or Conn’s syndrome. PHA may be caused by either adrenal hyperplasia (usually bilateral disease) or benign or malignant adrenal neoplasia (usually unilateral disease). In humans, the most common cause of PHA is bilateral adrenal hyperplasia and it is rare for humans to develop adrenal carcinomas as a cause of PHA. In cats, the most common cause of PHA is an approximately equal incidence of unilateral adrenal adenomas or carcinomas. TABLE 5 DIAGNOSTIC TESTING FOR PHA A diagnosis of PHA is ideally made based on the following criteria: • Hypertension • +/- Hypokalemia (may be a late stage finding) • Elevated plasma aldosterone levels (6x higher than normal) • Increased urinary potassium excretion (6x higher than normal) • Elevated aldosterone:renin ratio. The gold standard finding in PHA is an elevated aldosterone with very low renin activity which indicates persistent aldosterone synthesis in the absence of normal stimulation from the renin-angiotensin-aldosterone system. Clinical Note: Plasma renin measurement is technically difficult and not widely available as a commercial assay therefore the diagnosis of PHA often hinges on the other criteria together with advanced diagnostic imaging. • Adrenal mass or bilaterally enlarged adrenal glands identified on abdominal ultrasound. Clinical Note: The absence of adrenal changes does NOT rule out PHA as some masses are too small to be detected by ultrasound. A fludrocortisone suppression test has recently been evaluated (2013) and appears to be a practical method of confirming most cases of PHA in cats and of substantiating the absence of PHA with otherwise questionable diagnostic results. • The urinary aldosterone-to-creatinine ratio (UACR) was determined before, during and after 4 days of fludrocortisone (0.05 mg/kg PO BID) administration • Findings: • All cats with PHA had UACR >7.5 x 10-9 • Fludrocortisone failed to suppress or resulted in <50% suppression in 6/9 PHA cats • In non-PHA cats with UACR >7.5 x 10-9 fludrocortisone resulted in >50% suppression Clinical Signs and Physical Examination Findings PHA most commonly affects older cats with a median age of 13 years. Common presenting clinical signs include weakness, neck ventroflexion, stiffness, collapse, plantigrade stance or other signs related to hypokalemic polymyopathy. Ocular abnormalities are a common owner complaint and physical exam findings of anisocoria, anterior/posterior chamber hemorrhage, retinal hemorrhage, retinal detachment, and blindness are regularly identified as a result of systemic hypertension. Affected cats will often present with varying degrees of polyuria, polydipsia, and abdominal distention and heart murmurs are commonly detected. Diagnosis There are no specific CBC findings associated with PHA in cats. The chemistry panel will frequently reveal hypokalemia and hypomagnesemia (often severe), hypophosphatemia, elevated CPK, and varying degrees of azotemia. If blood gas analysis is performed, affected cats may have metabolic alkalosis due to the excess excretion of hydrogen ions in PHA. Clinical Note: Any cat presenting with hypertension and/or hypokalemia should be screened for the presence of PHA. Keep in mind, hypokalemia may represent a much later development in the natural course of PHA. Failure to suspect PHA because of normal potassium levels may result in underdiagnosis of PHA in the hypertensive feline population and delay identification and management of this treatable disease. Plasma aldosterone levels are readily available (and not prohibitively expensive!) and are required to establish the diagnosis of PHA. The presence of marked hyperaldosteronism— typically 6 times higher than normal—is supportive of a diagnosis of PHA. Clinical Note: Cats with chronic renal failure present a diagnostic dilemma as they may be hypertensive, hypokalemic and if measured, their aldosterone levels may be elevated. Generally aldosterone will only be elevated 2 to 3 times normal in cats affected by chronic renal failure as opposed to at least 6 times normal in cats affected by PHA. See Table 5 for available diagnostic testing for PHA. Abdominal ultrasound imaging remains part of the gold standard for diagnosis of PHA. Ultrasound commonly confirms the presence of a unilateral adrenal mass in affected cats, however, failure to find a mass DOES NOT exclude neoplasia as a differential as some lesions are very small and may not be visualized for months after the diagnosis. CT can be performed and may be particularly helpful for identifying small lesions and vascular invasion. The ability to use contrast enhancement is also potentially advantageous for challenging cases. Treatment and Prognosis As most cats with PHA are affected by unilateral adrenal neoplasia, adrenalectomy is the treatment of choice. Adrenalectomy offers a chance of a complete cure—resolution of hypertension and hypokalemia should be expected if resection is complete and no metastatic disease is present. In one recent (2014) study, none of the surviving cats required continued medical management after surgery. In other studies, over 80% of cats do not require additional therapy for hypertension. While adrenalectomy may be a technically challenging surgery and peri-operative complications such as hemorrhage, hypotension and cardiac arrhythmias have been reported, it can be a very successful surgery. Additionally, laparoscopy provides a minimally invasive means of performing an adrenalectomy with a shortened procedure time and post-procedural morbidity. Laparoscopy is a viable option for the treatment of affected cats if diagnostic imaging has ruled out intravascular invasion of the adrenal tumor or overt metastatic disease. Laparoscopy is a very good option to consider for the right patient and in a location where an experienced surgeon is available. The overall median survival time for cats undergoing unilateral adrenalectomy was reported to be 1,297 days (2-1,582 days). The 2014 study found anesthesia time to be strongly correlated with prognosis; cats with <4 hours of anesthesia time had a MST of 1,329 days and cats with >4 hours of anesthesia time had a MST of 10 days. Survival did not depend on the presence of an adenoma versus carcinoma or sidedness of the tumor. Medical management is a viable option for cats whose owners will not consider surgery, who have advanced or metastatic disease, bilateral adrenal hyperplasia, or who are poor anesthetic or surgical candidates. Clinical Note: Medical management can also be instituted in order to metabolically stabilize a patient prior to surgery. The cornerstones of medical management include control of systemic hypertension and weakness associated with hypokalemia by the use of the following therapies: • Amlodipine 0.625-1.25 mg/cat q day up to BID • Spironolactone 2-4 mg/kg/day • Potassium gluconate 2-6 mEq/day The MST of cats with PHA treated solely with medical management has been reported to be 50-984 days. Many cats treated with medical management will have marked clinical improvement—like “Autumn”—but are unlikely to have full resolution of hypokalemia and hypertension. The underlying mass and associated complications such as tumor hemorrhage or distant metastasis are obviously also not addressed with this approach. “AUTUMN’S” TREATMENT AND OUTCOME Upon admission, immediate control of “Autumn’s” blood pressure and marked hypokalemia were pursued. She received amlodipine (1.25 mg PO) and her blood pressure improved within 4 hours to 140 mmHg. Due to the severity of her cardiac chamber enlargement, “Autumn” was unable to tolerate maintenance intravenous fluids so her potassium and magnesium supplementation was administered as ultra-low volume continuous rate infusions. Potassium was given at 1.35 mEq/hr (0.5 mEq/kg/hr) and magnesium sulfate at 0.25 mEq/hr (0.1 mEq/ kg/hr) to address her severe electrolyte deficiencies. Clinical Note: When potassium chloride is given intravenously, the infusion rate is more critical than the total amount administered. The rate should generally not exceed 0.5 mg/kg/hr. Slow increases in her serum potassium were noted but exceedingly high dosages (up to 0.8 mEq/kg/hr) were required to increase her potassium to 2.9 mEq/L over the first 24 hours. Spironolactone was started at 6.25 mg PO BID (approximately 2.5 mg/kg PO BID) as another means to increase her serum potassium levels. Clinical Note: Spironolactone works by antagonizing aldosterone receptors in the distal renal tubules and as such will increase serum potassium concentrations. It is commonly used in cats with primary hyperaldosteronism. Within 24 hours “Autumn’s” neurologic status had improved dramatically. She began eating on her own and Tumil-K® (2 mEq PO BID) was added as an oral potassium supplement. By 48 hours after presentation, “Autumn” had a normal serum potassium concentration of 4.39 mEq/L. Her continuous IV potassium infusion was gradually decreased to 0.7 mEq/kg/hr and then to 0.3 mEq/kg/hr. Oral Tumil-K® was increased to 3 mEq PO BID to maintain her serum potassium concentration. Magnesium sulfate was gradually decreased (0.2 mEq/hr to 0.1 mEq/hr) as her serum magnesium concentrations became normal. “Autumn” required a decrease of her amlodipine to 0.625 mg PO q day to best address her blood pressure. By the third day of hospitalization, “Autumn’s” intravenous potassium and magnesium were discontinued and her potassium remained stable at 4.18 mEq/L. Unfortunately her magnesium decreased when off intravenous supplementation to 1.27 mEq/L and she required oral supplementation with Milk of Magnesia®. “Autumn” was monitored for an additional 24 hours and serum potassium and magnesium concentrations remained stable on oral supplementation. Her renal parameters were stable (BUN 37, creatinine 3.1) and blood pressure was well controlled. “Autumn” was discharged to her owner with instructions to give the following at home: spironolactone (6.25 mg PO BID), amlodipine (0.625 mg PO q day), Tumil-K® (3 mEq PO BID), Milk of Magnesia® (1ml PO BID) and prednisolone acetate eye drops (1 drop OS x 7 days) to address her anterior chamber hemorrhage. The plan was to institute clopidogrel therapy once “Autumn’s” anterior chamber hemorrhage resolved and her hypertension remained well controlled. “Autumn” continued to improve clinically at home and her neurologic signs resolved. At her first recheck one week after release from the hospital, her blood pressure was stable between 130 and 160 mmHg on the lower dosage of amlodipine but her potassium had declined to 2.8 mEq/L. Her magnesium was not rechecked. Unfortunately, the owner had been relying on “Autumn’s” appetite for administration of her medication. Clinical Note: Cats commonly develop food aversions when owners attempt to hide medication within their food. In a patient like “Autumn” who requires multiple life-saving medications, it is imperative to teach owners how to directly pill their cat. The aldosterone level was reported at the time of “Autumn’s” first recheck and confirmed the presumptive diagnosis of PHA. Additional therapeutic options for PHA were discussed with the owner, including abdominal exploratory for adrenalectomy/mass resection in order to best control “Autumn’s” electrolyte abnormalities and hypertension. However, given the appearance of the mass on ultrasound, surgery was considered potentially high risk and a CT scan was advised to determine the relationship of the mass to the vena cava and portal vein for surgical planning purposes. “Autumn’s” owner declined surgery and has continued to see her RDVM. Her owner has more consistently been able to administer the spironolactone and amlodipine although the potassium supplement is a bit more sporadic. The Milk of Magnesia® has not been required to maintain her magnesium levels. The owner reports “Autumn” is doing very well at home with great energy and is even able to jump onto the furniture at home. Although a definitive histopathologic diagnosis of “Autumn’s” adrenal lesion was not obtained, her case highlights many important points about feline hypertension and the medical management of cats with primary hyperaldosteronism. COMMENTS The most important take-home message is that we should be screening older cats for the presence of hypertension in order to diagnose systemic hypertension earlier—before target organ damage occurs. If a cat is hypertensive—especially if it is refractory— keep primary hyperaldosteronism on your list of differentials as it is more common than once thought. While PHA should certainly be considered a differential in cats presenting with systemic hypertension and hypokalemia, using hypokalemia as a definitive criterion for screening is likely to result in under-diagnosis of PHA in the hypertensive feline population. Clinical Note: Idiopathic hypertension is RARE in the cat. While many of these cats have CKD, some of these hypertensive cats may actually have PHA. Aldosterone levels should be measured and the adrenal glands imaged in all cases of apparently “idiopathic” feline hypertension. REFERENCES Polzin, David J. Chronic Kidney Disease, Chapter 311. The Textbook of Veterinary Internal Medicine, Ettinger and Feldman editors, 7th edition, Elsevier, St. Louis, 2014. Stepien, Rebecca L. Pathophysiology of Systemic Hypertension and Blood Pressure Assessment, Chapter 151. The Textbook of Veterinary Internal Medicine, Ettinger and Feldman editors, 7th edition, Elsevier, St. Louis, 2014. Lo, AJ, DE Holt, DC Brown, et al. Treatment of Aldosterone-Secreting Adrenocortical Tumors in Cats by Unilateral Adrenalectomy: 10 cases (2002-2012). J Vet Intern Med 2014, 28: 137-143. Djajadiningrat-Laanen SC, Galac, MH Boeve, etc. al. Evaluation of the oral fludrocortisone suppression test for diagnosing primary hyperaldosteronism in cats. J Vet Intern Med 2013 Nov-Dec 27(6): 1493-9. Djajadiningrat-Laanen S, S Galac, H Kooistra. Primary hyperaldosteronism: expanding the diagnostic net. J Feline Med Surg Sept 2011; 13(9): 641-50. Schulman, Rhonda L. Feline primary hyperaldosteronism. Vet Clin North Am Small Anim Pract. March 2010; 40(2): 353-9. Brown, S., C. Atkins, R. Bagley, et al. Guidelines for the Identification, Evaluation, and Management of Systemic Hypertension in Dogs and Cats. J Vet Intern Med 2007; 21: 542-558. Roderick, Andrew Ash, AM Harvey, S Tasker. Primary hyperaldosteronism in the cat: a series of 13 cases. J Feline Med Surg June 2005; 7(3): 173-82 CLINICAL ASSESSMENT 1 2 Idiopathic hypertension is common in cats. True or False? An appropriate initial workup for any cat presenting with hypertension includes all EXCEPT the following: a.Minimum database (CBC, Chemistry panel, T4, Urinalysis) b.Chest radiographs c.Abdominal ultrasound d.Aldosterone levels 3 Aldosterone levels 2 times above normal are consistent with primary hyperaldosteronism. True or False? 4 5 6 Adrenal hyperplasia is the most common cause of PHA in cats and medical management is the treatment of choice. True or False? What is the general guideline for maximum intravenous rate of potassium infusion? Proper indirect blood pressure technique includes all EXCEPT the following: a.Patient acclimation for 5-10 minutes prior to blood pressure measurement b.Pressure cuff 60% of the circumference of the limb or tail c.Artery positioned at the same level as the heart d.Discard first value and average 5-7 subsequent readings 7 Complete resolution of clinical signs can be expected with medical management for PHA in affected cats. True or False? 8 What is the mechanism of action of spironolactone and why is it used in the management of PHA? 9 Medical management of PHA includes all EXCEPT the following: a.Spironolactone b.Furosemide c.Amlodipine d.Potassium gluconate e. Magnesium 10 Hypomagnesemia may cause refractory hypokalemia. True or False? CLINICAL ASSESSMENT ANSWERS: 1. False. Idiopathic hypertension is rare in cats. Secondary hypertension is the most common cause of systemic hypertension and accounts for at least 80% of cases in both dogs and cats. 2. d) Aldosterone levels. Aldosterone levels should not necessarily be performed during the INITIAL screening workup of systemic hypertension. They are indicated if there is no apparent underlying disease, if the chemistry panel reveals hypokalemia or a cat is exhibiting signs of hypokalemic polymyopathy, if the abdominal ultrasound reveals adrenal abnormalities or if hypertension becomes refractory to treatment. 3. False. Aldosterone levels are expected to be 6 times (or more) above normal in cats affected by PHA. In addition, most affected cats will have systemic hypertension, hypokalemia, increased urinary excretion of potassium and an adrenal mass apparent on imaging. The diagnosis is sometimes imperfect and if aldosterone levels are not as dramatically elevated, a fludrocortisone suppression test could be considered as cats affected by PHA will fail to suppress or have <50% suppression of their UACR (urinary aldosterone: creatinine ratio). 4. False. Unilateral neoplasia (either adenoma or carcinoma) is the most common cause of PHA in cats and adrenalectomy is the treatment of choice. Resolution of hypertension and hypokalemia should be expected post-operatively with full resection. 5. When potassium chloride is given intravenously, the rate is more critical than the total amount administered. The rate should generally not exceed 0.5 mEq/kg/hr. If the infusion rate needs to be higher than this, a sampling line for aggressive serum potassium monitoring and close monitoring of cardiovascular status are required. 6. b) The pressure cuff should measure 40% of the circumference of the limb or tail to prevent erroneous blood pressure readings. 7. False. Most cats treated with medical management will have marked clinical improvement but they are unlikely to experience full resolution of hypokalemia and hypertension. The underlying mass and associated complications such as tumor hemorrhage or distant metastasis are obviously also not addressed with medical management. While surgery is the treatment of choice, medical management is a viable option for cats whose owners will not consider surgery, who have advanced or metastatic disease, bilateral adrenal hyperplasia, or who are poor anesthetic or surgical candidates. 8. Spironolactone is an aldosterone-antagonist which makes it useful for the management of PHA in cats. Aldosterone is competitively inhibited by spironolactone in the distal renal tubules with resultant increased excretion of sodium, chloride and water and decreased excretion of potassium, ammonium and phosphate. 9. b) Furosemide. Furosemide may induce fluid and electrolyte (particularly potassium) imbalances. Spironolactone is used in PHA primarily as an aldosterone antagonist and not specifically as a diuretic. 10. True. If you are unsuccessful at correcting hypokalemia with oral or intravenous potassium supplementation, measure serum magnesium as hypomagnesemia may be responsible. Milk of Magnesia® is a readily available source for oral magnesium supplementation.