Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
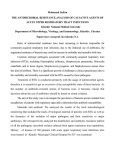
Schaad_OM Pharma_A4_2011 02/11/2012 11:18 Page 111 Respiratory Tract Infections The Management of Recurrent Respiratory Tract Infections in Children Urs B Schaad1 and Nicola Principi2 1. Professor Emeritus in Paediatrics and Paediatric Infectious Diseases, University of Basel, Basel, Switzerland; 2. Chair of Paediatrics, Universita degli Studi di Milano, Fondazione IRCCS Ospedale Maggiore Policinico, Mangiagalli e Regina Elena, Milan, Italy Abstract Respiratory tract infections (RTIs) constitute a major healthcare burden in children throughout the world. They tend to be recurrent, often causing multiple episodes of illness within a single year. Immature immune system, the presence of genetic and environmental factors and exposure to pathogens make young children highly susceptible to RTIs. These infections are still treated with antibiotics but the rise in resistant bacterial strains has prompted investigation of novel preventative strategies. One such approach to prevent recurrent RTIs (RRTIs) is the immunostimulant OM-85 that is an extract of eight pathogenic bacteria which has proven safe and effective as prophylaxis of recurrent respiratory infections in children at risk. Increased awareness and use of preventative approaches, including OM-85, are likely to help avoid the complications and co-morbidities of RTIs; and have the potential to significantly reduce the burden of disease and bacterial resistance. Keywords Recurrent respiratory tract infections, bacterial infection, virus, lung damage, immune response, immunostimulant, OM-85 Disclosure: Urs B Schaad serves as Consultant in Paediatrics for OM Pharma SA, Geneva, Switzerland. Urs B Schaad and Nicola Principi are Members of the Scientific Advisory Board for OM-85. Received: 12 September 2012 Accepted: 1 October 2012 Citation: European Infectious Disease, 2012;6(2):111–5 Correspondence: Urs B Schaad, University Children’s Hospital Basel UKBB, PO Box, CH-4031 Basel, Switzerland. E: [email protected] Support: The publication of this article was funded by OM Pharma SA. Burden of Respiratory Tract Infections in Children Paediatric respiratory tract infections (RTIs) are associated with significant morbidity and mortality worldwide.1 In industrialised countries, approximately half of the medical consultations concerning children involve RTIs.2 Moreover, these are often recurrent infections, occurring numerous times a year. The epidemiology data of RTIs are variable depending on the specific year and setting studied. In general, mortality rates in children within developed countries are relatively low.3 In contrast, RTIs in developing countries are not only more prevalent but also more severe, resulting in over 2 million deaths per year.4,5 A recent report from the United Nations International Children's Emergency Fund (UNICEF) concluded that over 2 million child deaths could be prevented in the 75 countries with the highest mortality burden if the entire population of children aged less than five years in each of these countries received the same coverage already available to the wealthiest 20 % of people in those countries.6 From other studies, it was estimated that approximately 6 % of children under the age of six years present with recurrent RTI.7 In developed countries, up to 25 % of children less than one year and 18 % of those aged 1–4 years experience recurrent RTIs.8 The vast majority (80–90 %) of RTIs are caused by viruses including rhinovirus, respiratory syncytial virus (RSV) and influenza. RSV is a common cause of both upper and lower RTIs. The same has been demonstrated for rhinovirus. However, whereas RSV is more common in younger children, rhinovirus strains A and B have been found as a © TOUCH MEDICAL MEDIA 2012 cause of RTIs in both younger and older children.9 Recent studies have highlighted the burden of influenza in young children.10,11 While recurrent RTIs often begin as viral infections, bacterial infection is observed in 60 % of patients with symptoms of an upper RTI lasting at least 10 days.12,13 Bacteria commonly involved in recurrent RTIs include Haemophilus influenzae, Streptococcus pneumoniae, Moraxella catarrhalis, Klebsiella pneumoniae and Streptococcus pyogenes.8,14,15 Bacterial infections of the lung have also been found to play a role in preschool children with recurrent wheeze.16 In particular, Mycoplasma pneumoniae, H. influenzae, S. pneumoniae and M. catarrhalis were the most commonly isolated species in these individuals. The burden of RTIs extends beyond their incidence and epidemiology data. The diagnosis of recurrent RTIs can be particularly challenging for paediatricians. While many infections involving the upper respiratory tract are easily managed, others are indicative of a more serious underlying pathology such as bronchiectasis or immune dysfunction.7 Further, differential diagnosis requires the appropriate use of diagnostic tools by physicians. Additional burdens include subsequent morbidity and complications in the child, resultant overuse and misuse of antibiotics, and all associated healthcare as well as indirect societal costs. These will be discussed in greater detail below. The Child Immune System The high incidence of respiratory infections in children relative to older adolescent and adult populations can be partially explained by the apparent limitations of their young immune systems. In fact, defects in immune responses are known to correlate with multiple 111 Schaad_OM Pharma_A4_2011 02/11/2012 11:18 Page 112 Respiratory Tract Infections Table 1: Summary of Environmental and Genetic Risk Factors for the Development of Recurrent Respiratory Tract Infections Environmental risk factors Day care attendance Early socialisation Large family size and overcrowding School-aged siblings Reduced breastfeeding Passive smoking, excessive exposure to pollutants, contact with infectious agents and the absence of breastfeeding have all been reported to increase the risk of infection.7,29 Indeed, breast milk contains important nutrients that help enhance the child’s immune response.30 Furthermore, attendance at crowded day care centres or preschools as well as interactions with siblings and other family members may add to the likelihood of RTIs.25 Missed or lack of vaccinations and malnutrition are other risk factors for RTIs that are especially prevalent in developing countries.31 Exposure to pollutants (indoor and outdoor) Home dampness and pets Genetic Risk Factors Parental smoking and smoking during pregnancy Certain children have a familial predisposition for recurrent and severe respiratory infections.32 This is often linked to the anatomical, physiological and/or immunological features of the individual.33 RTIs have been attributed to anatomic or functional alterations of the upper and/or lower airways as well as reduced immunity in the child. A family history of atopic diseases, low bodyweight and male gender have also been reported to contribute to a higher risk of RTIs.7 Malnutrition and missed vaccination Intense training and physical stress Genetic risk factors Positive family history of atopic diseases Prematurity and low bodyweight infants Anatomic or functional alterations of the airways Allergy/atopy Male gender Source: Jesenak et al., 2011.7 RTIs.17,18 It is, however, rare for a child with recurrent RTIs to present with a true immunodeficiency, rather there is likely an immaturity in their immune system due to their young age leading to increased infections;19 humoral and phagocytic immunity do not reach their optimal protective state until the fifth or sixth year of life.20,21 As such, it is important for paediatricians to be able to differentiate between deficiency and immaturity. For the most part, the child has normal immune functions – albeit young and immature – and therefore any symptoms or complications from RTIs will be transient and of limited duration. On the other hand, if a child presents with excessive amounts of infections (e.g. eight or more occurrences of otitis media in 12 months, two or more serious sinus infections within 12 months or several community-acquired pneumonia), there is likely to be an underlying primary immunodeficiency that requires attention.22,23 Careful history-taking and examination along with prompt immunologic testing are needed to make an accurate diagnosis and treat these patients appropriately. Although most affected children do not have immunodeficiencies, some may exhibit lower levels of haematological or immunological parameters such as deficiencies in specific immunoglobulin (Ig) isotypes or, much more rarely, decreased phagocytosis.7 Other aspects of the immune system that are immature in newborn and young children include T cells, cytotoxic activity, neutrophil production and function, and complement levels.24 It is also important to note the possibility that the observed immune defects are the consequences rather than the cause of recurrent RTIs. In particular, viral infections are known to influence immune responses.7 As such, repeated infections and viral penetration could result in ever deeper virus-induced immune dysfunction, which would in turn favour further respiratory infections, leading to a vicious cycle of recurrent RTIs.25,26 Patient Profile and Risk Factors Environmental Risk Factors A number of environmental factors have a well-established effect of increasing the susceptibility of a child to recurrent lung infections.27, 28 112 Table 1 lists the key environmental and genetic risk factors associated with the development of recurrent RTIs. Strategies to prevent recurrent RTIs must take into consideration all these patient characteristics and factors that potentially increase the risk for disease. Research has suggested that patients with the greatest risk of recurrent RTIs benefit the most from therapeutic intervention and prevention.17 Definition RTIs include all viral and bacterial infections of the upper or lower airways. These could be relatively benign and easily controlled or potentially more serious diseases such as pneumonia or bronchitis that can cause permanent lung damage. Recurrent RTIs can be defined as at least three RTI episodes per year or fall/winter season for at least two years.17,32 However, in terms of more specific definitions of individual types of infections (e.g. otitis media, infectious rhinitis, etc.), there is no clear consensus on a definition of ‘recurrent’, although standard references exist.7 For otitis media, three episodes within six months or four within 12 months is considered recurrent. In contrast, recurrent infectious rhinitis is frequently defined as greater than five episodes per year. Finally, recurrent pharyngitis or tonsillitis is more than three episodes within 12 months.8,34,35 For the most part, however, definitions tend to be arbitrary and may not necessarily help physicians determine the optimal therapeutic option for individual patients. Morbidity and Complications Direct complications from recurrent RTIs include bacterial manifestations such as acute otitis media, sinusitis and bronchitis.32 Infections of the ear, nose and throat constitute the most common pathologies in children aged six months to six years.34,36 Other important consequences include mastoiditis, pneumonia and sepsis. Paediatricians therefore need to diagnose and monitor patients carefully to limit these potentially life-threatening events and manage them appropriately. In some severe cases, the RTI may be fatal for the child. This risk is especially prevalent in developing countries where child mortality rates are generally higher.32 In the long-term, recurrent RTIs can cause damage to the lungs and lead to further respiratory problems as well as increased risk of disease in the future.37 Moreover, RTIs can at times lead to exacerbations of cough and wheeze in children.38 An association between recurrent RTIs in early life and asthma has been EUROPEAN INFECTIOUS DISEASE Schaad_OM Pharma_A4_2011 02/11/2012 11:19 Page 113 The Management of Recurrent Respiratory Tract Infections in Children reported39 and for some children, repeated respiratory infections are the first manifestations of asthma.7 These strategies look to prevent the development of recurrent RTIs in children by reducing the risks of infection. Socioeconomic Burden Parent Education Recurrent RTIs are responsible for much socioeconomic burden in the world, causing absenteeism from school for the child and from work for the parent(s).8,40,41 Healthcare and medical costs as well as learning delays from missed school days also add to the socioeconomic burden of recurrent RTIs.31 A key aspect of initiatives to prevent recurrent infections in children is the education of their parents. They need to know what factors increase a child’s risk of recurrent RTIs and work to minimise them. For example, the absence of breastfeeding is a risk factor for infection, suggesting a protective role of mothers’ milk in the infant. Breast milk is rich in nucleotides that have immunomodulatory activity thus enhancing a child’s immune defence. Similarly, nucleotide supplementations to infant formulas augment natural killer cell activity and humoral response.30 By increasing their knowledge of the disease and risk factors, parents can better care for their children and potentially reduce the frequency of RTIs. A study of 600 Australian families showed a mean 2.2 respiratory episodes per person per year, the frequency and severity being higher in young children (<2 years).42 The mean episode duration was 6.3 days; 28.7 % of these events required a visit to the physician and there was a 23 % rate of absenteeism. Another study with healthy children aged 12–71 months during a winter season in Australia demonstrated an average of 0.53 respiratory infectious episodes per child per month.43 The mean duration per episode was 10.4 days and for every 100 episodes there were 46.7 general practitioner visits, 19.7 courses of antibacterial therapies prescribed and 2.2 hospital admissions, all increasing the cost and burden of disease. The average cost of a community-managed acute respiratory episode was found to be AU$241 and approximately 70 % of this cost was the carer’s time away from their normal activities in order to care for the child. Non-prescription medications and general practice visits made up only a small proportion of the costs at 5.4 and 5.0 %, respectively.44 Other risk factors must also be limited; a child’s exposure to air pollution, passive smoke and overcrowded day care centres should be reduced as much as possible, and parents can play a major role in avoiding such adverse environments.7 Parents must also remember that children with recurrent infections are still ‘normal’ with regard to their immune response and so any major interferences to their developing immune system, such as surgery (e.g. adenoidectomy and tonsillectomy) or prophylactic antibiotic treatment, may actually be harmful and counter-productive.7 Immunisation Antibiotic Overuse and Misuse Antibacterial resistance in the bacteria that commonly cause or complicate RTIs is a major healthcare concern.45 If it is not adequately addressed, children will continue to encounter stronger, more resistant pathogens in the future. Overuse and misuse of antibiotics are the main factors that perpetuate this issue of resistance. Overuse refers to using antibiotic treatment when it is not necessary or indicated (i.e. for viral infections and non-infectious diseases). Conversely, antibiotic misuse occurs when the therapy is used incorrectly, either the wrong antibiotic is chosen or the dosage and/or duration are not appropriate. The use of antibiotics is common for the treatment of infections including RTIs. However, as these are often viral infections, antibacterials will likely not be effective in these situations.46,47 When a bacterial infection has been properly diagnosed as the cause of disease, antibiotics are the favoured treatment option. However, even with such infections, multiple courses of antibacterial therapies do not cure nor do they prevent subsequent recurrences. Importantly, application of these therapies contributes to the development of antibiotic-resistant strains of bacteria.48–50 Other drivers of resistance include the type of antibiotic used and the high rate of clonal spread. Considering the prevalence and effects of antibiotic resistance, it becomes important for paediatricians to take care when prescribing and ensure appropriate and responsible use of antibiotics.51 Improved diagnostic techniques that can provide more rapid and reliable identification of causal pathogens in RTI would allow antibiotics to be avoided whenever possible thereby limiting the number of unnecessary courses administered prior to a definitive diagnosis. Many vaccines are currently available to prevent various childhood diseases. As such, effective vaccination programmes for children to protect against viruses and bacteria known to cause RTIs will be the ultimate goal. At present, there are vaccines against influenza, measles, S. pneumoniae, B. pertussis and H. influenzae type b, which are relevant to the prevention of the infections due to these infectious agents. However, the availability of these vaccines is low in some areas of the world therefore limiting the effect of this strategy. Large-scale take-up of vaccination within any population is vital to establish herd immunity and limit exposure of vulnerable children to pathogens. Parents therefore need to understand the importance of immunisations for their children. While these vaccines should be administered wherever available, their role in preventing some recurrent viral infections is limited. In fact, only influenza vaccination can have a direct impact in this setting. As RTIs are mainly due to viruses the roles of bacterial vaccines (pertussis, pneumococcus and H. influenzae b) are limited in avoiding initial episodes even if they can play a relevant role in reducing bacterial complications. Immunostimulation As a result of the strong association between recurrent RTIs and inadequacies of the immune system, bacterial immunostimulants have been developed to non-specifically boost the body’s own defences against any invasive pathogens.31 Bacterial immunostimulants were first introduced in the 1980s and there are now several licensed formulas that are marketed around the world for the prevention and treatment of bacterial infections of the upper and lower respiratory tract. These include BioStim®, Luivac®, IRS 19®, Ribomunyl® and Broncho-Vaxom® (Broncho-Munal®, Ommunal®, Paxoral® and Vaxoral®).40 Preventive Measures As a result of the risks and negative impact antibiotic use can have in society, other forms of infection management have been explored. EUROPEAN INFECTIOUS DISEASE Some immunostimulant preparations are bacterial lysates while others contain cellular structures such as ribosomes. The constituents of each 113 Schaad_OM Pharma_A4_2011 05/11/2012 12:15 Page 114 Respiratory Tract Infections Figure 1: Proportion of Children with Recurrent Respiratory Tract Infections Following OM-85 or Placebo Percentage of patients in each group with ≥3 respiratory tract infections per six months 70 % 58.20 % 60 % 50 % p<0.001 40 % 32 % bacteria strains coming from eight bacteria species (Haemophilus influenzae, Streptococcus pneumonia, Streptococcus viridans, Streptococcus pyogenes, Klebsiella pneumoniae ssp. pneumonia, Klebsiella pneumoniae ssp. ozaenae, Staphylococcus aureus, Moraxella catarrhalis) often associated with respiratory infections. Taken orally, it is capable of inducing non-specific innate and adaptive immune responses in an individual. Following intestinal absorption, OM-85 stimulates immune cells in the intestinal mucosa. As a result, OM-85 can raise the overall body defences against infections by shaping the dendritic cell activation into a ‘pre-alert’ phenotype.53 30 % Efficacy 20 % 10 % 0% OM-85 Placebo Source: Schaad, 2010.17 Figure 2: Relationship Between Efficacy of OM-85 and Number of Respiratory Tract Infections in the 12 Months Prior to Treatment Favours OM-85 4.5 4.0 Mean differences & 2 SEM 3.5 The efficacy of OM-85 in children was supported in a recent meta-analysis of eight randomised controlled trials.17 Mean age and number of RTIs were comparable between the OM-85 (n=435) and placebo (n=416) groups at admission. Following treatment, there was a significant decrease in the percentage of children with recurrent RTIs (defined as at least three RTIs in six months) in the OM-85 treatment group relative to the placebo group (32 versus 58.2 %, p<0.001) (see Figure 1). There is also an association between OM-85 efficacy and the number of RTIs in the year prior to treatment indicating that patients with the highest frequency of RTIs benefit the most from treatment (see Figure 2). OM-85 was also shown to significantly reduce the duration of acute RTI, the number of infections, the use of antibiotics and conventional drugs, and the time on treatment compared with placebo.54 3.0 2.5 2.0 Ref 2 Ref 6 1.5 Ref 5 Ref 4 1.0 0.5 0.0 -0.5 -1.0 Ref 3 2 4 6 8 10 12 Ref 1 Number of recurrent RTIs during previous 12 months Favours placebo RTIs = Respiratory tract infections; SEM = Standard error of the mean. References 1: Schaad et al., 1986,58 2: Jara-Pérez et al., 2000,59 3: Schaad et al., 2002.60 4: Zagar et al., 1988,61 5: Del-Rio-Navarro et al., 2003.62 6: Gutiérrez-Tarango et al., 2001.63 Mean differences are shown with error bars representing the standard error of the mean. Source: Schaad, 2010.17 formulation were chosen according to their highly immunogenic properties. In RTI immunostimulants enhance the immune system, eliciting immune responses both in the respiratory tract and systemically, thereby inducing better protection against infections. This reduces both the frequency and severity of RTIs which in turn decreases the need for antibiotics and any subsequent resistance.31 Bacterial immunostimulants have shown positive safety data in trials while decreasing the number of RTIs as well as the use of antibiotics and other concomitant medications. Other immunostimulants in the form of herbal extracts and synthetic compounds also exist – such as pidotimod – that may be effective in decreasing the number of recurrent RTIs.52 However, compared with bacterial extracts, there is substantially less data available for these treatment options and further research is required. OM-85 in the Prevention of Recurrent Respiratory Tract Infection in Children OM-85 (Broncho-Vaxom®, Broncho-Munal®, Ommunal®, Paxoral® and Vaxoral®) is a standardised immunoactive lyophilised extract of 21 114 Another recent study looked at the effect of OM-85 on wheezing attacks associated with acute RTIs in children over the course of 12 months.55 Wheezing attacks are also a large healthcare concern, responsible for many hospital admissions in young children. OM-85 significantly reduced the number of wheezing attacks (37.9 % cumulative reduction, p<0.001) and the number of RTIs (31.4 % cumulative reduction, p<0.001) relative to placebo in the children studied (n=75). OM-85 was also shown to improve Ig levels and reduce infections in children with recurrent RTIs and hypogammaglobulinemia.56 This therapy significantly increased IgG and IgA levels post-treatment versus pre-treatment as well as versus placebo, with many reaching normal serum levels for their age. Safety The safety profile of OM-85 has been evaluated during more than 30 years of post-marketing experience. Adverse events are mostly non-serious and transitory. The most common side effects are headache and nausea, and OM-85 has shown a similar safety profile as placebo. Furthermore, no signs of autoimmunity have been observed in any subjects. A recent study on the effect of OM-85 prophylaxis on autoimmunity in IgA-deficient children found no significant difference between receivers and non-receivers of OM-85 in terms of clinical or laboratory markers for autoimmunity during four years of follow-up.57 Parent education and practical prophylaxis are important in managing recurrent RTIs in children. Parents need to be aware of the options available and how best to use them to benefit their offspring. At present, for preventive treatment, OM-85 is indicated for children as follows: one capsule/sachet (3.5 mg) or 10 drops (11 mg/ml) per day on an empty stomach for 10 consecutive days per month for three consecutive months, ideally before the beginning of the autumn. EUROPEAN INFECTIOUS DISEASE Schaad_OM Pharma_A4_2011 02/11/2012 11:19 Page 115 The Management of Recurrent Respiratory Tract Infections in Children Improved understanding by parents will ensure optimal compliance and improved clinical outcomes. essential alternative for the management of this disease and help reduce the risk of developing respiratory infections. At present, many practitioners still fail to employ prevention strategies in children with recurrent RTIs. Conclusions Paediatric recurrent RTIs represent a huge global health burden, resulting in much morbidity and mortality in children. Moreover, they contribute greatly to socioeconomic costs in the form of absenteeism from work of parents as well as visits to the general practitioner. Antibacterial treatments are often prescribed in this population; however, they have limited efficacy and, more importantly, increase the level of antibiotic resistance around the world. Preventive measures are therefore an 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. Williams BG, Gouws E, Boschi-Pinto C, et al., Estimates of world-wide distribution of child deaths from acute respiratory infections, Lancet Infect Dis, 2002;2:25–32. Kvaerner KJ, Nafstad P, Jaakkola JJ, Upper respiratory morbidity in preschool children: a cross-sectional study, Arch Otolaryngol Head Neck Surg, 2000;126:1201–6. Jokinen C, Heiskanen L, Juvonen H, et al., Incidence of community-acquired pneumonia in the population of four municipalities in eastern Finland, Am J Epidemiol, 1993;137:977–88. Rudan I, Boschi-Pinto C, Biloglav Z, et al., Epidemiology and etiology of childhood pneumonia, Bull World Health Organ, 2008;86:408–16. Wardlaw T, Salama P, Johansson EW, Mason E, Pneumonia: the leading killer of children, Lancet, 2006;368:1048–50. UNICEF, Pneumonia and diarrhoea: Tackling the deadliest diseases for the world's poorest children, 2012. Available at: www.unicef.org/media/files/UNICEF_P_D_complete_0604.pdf (accessed 2 July 2012). Jesenak M, Ciljakova M, Rennerova Z, et al., Recurrent Respiratory Infections in Children – Definition, Diagnostic Approach, Treatment and Prevention, MartÃn-Loeches I (eds.), Bronchitis (2011), InTech, Available at: www.intechopen.com/books/bronchitis/recurrentrespiratory-infections-in-children-definition-diagnosticapproach-treatment-and-prevention (accessed 23 May 2012). Bellanti JA, Recurrent respiratory tract infections in paediatric patients, Drugs, 1997;54 Suppl 1:1–4. Esposito S, Daleno C, Tagliabue C, et al., Impact of rhinoviruses on pediatric community-acquired pneumonia, Eur J Clin Microbiol Infect Dis, 2012;31:1637–45. Thompson WW, Shay DK, Weintraub E, et al., Influenzaassociated hospitalizations in the United States, JAMA, 2004;292:1333–40. Poehling KA, Edwards KM, Weinberg GA, et al., The underrecognized burden of influenza in young children, N Engl J Med, 2006;355:31–40. Kowalska M, Kowalska H, Zawadzka-Glos L, et al., Dysfunction of peripheral blood granulocyte oxidative metabolism in children with recurrent upper respiratory tract infections, Int J Pediatr Otorhinolaryngol, 2003;67:365–71. Salami A, Dellepiane M, Crippa B, et al., Sulphurous water inhalations in the prophylaxis of recurrent upper respiratory tract infections, Int J Pediatr Otorhinolaryngol, 2008;72:1717–22. Brook I, Shah K, Bacteriology of adenoids and tonsils in children with recurrent adenotonsillitis, Ann Otol Rhinol Laryngol, 2001;110:844–8. Gehanno P, Panajotopoulos A, Barry B, et al., Microbiology of otitis media in the Paris, France, area from 1987 to 1997, Pediatr Infect Dis J, 2001;20:570–3. Schwerk N, Brinkmann F, Soudah B, et al., Wheeze in preschool age is associated with pulmonary bacterial infection and resolves after antibiotic therapy, PLoS One, 2011;6:e27913. Schaad UB, OM-85 BV, an immunostimulant in pediatric recurrent respiratory tract infections: a systematic review, World J Pediatr, 2010;6:5–12. David JR, Rosen FS, Deficiencies in immunoglobulins and cellmediated immunity (CD-Rom). Chapter IX, Scientific American Medicine, New York, US, SAM-CD, 2000. Wheeler JG, Evaluating the child with recurrent infections, Am Fam Physician, 1996;54:2276–82,85–6. Wheeler JG, Steiner D, Evaluation of humoral responsiveness in children, Pediatr Infect Dis J, 1992;11:304–10. Yang KD, Hill HR, Neutrophil function disorders: pathophysiology, prevention, and therapy, J Pediatr, 1991;119:343–54. Champi C, Primary immunodeficiency disorders in children: EUROPEAN INFECTIOUS DISEASE 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. Currently there are several immunostimulants approved for use in treating recurrent RTIs and future trends will look to using and developing these more, making them available to a greater number of nations – particularly within developing countries that see higher child mortality rates from these diseases. OM-85 is currently the most studied immunostimulant and has the longest post-marketing experience with regards to efficacy and safety. n prompt diagnosis can lead to lifesaving treatment, J Pediatr Health Care, 2002;16:16–21. Slatter MA, Gennery AR, Clinical immunology review series: an approach to the patient with recurrent infections in childhood, Clin Exp Immunol, 2008;152:389–96. Evans N, Immature immune system and risk of infection in newborn infants, 2010. Available at: www.helium.com/items/ 1847365-immature-immune-system-and-risk-of-infection-innewborn-infants (accessed 9 October 2012). de Martino M, Balloti S, The child with recurrent respiratory infections: normal or not?, Pediatr Allergy Immunol, 2007;18(Suppl 18):13–8. Li Volti G, Malaponte G, Bevelacqua V, et al., Persistent high plasma levels of interleukins 18 and 4 in children with recurrent infections of the upper respiratory tract, Transplant Proc, 2003;35:2911–5. Don M, Fasoli L, Gregorutti V, et al., Recurrent respiratory infections and phagocytosis in childhood, Pediatr Int, 2007;49:40–7. Bloomberg GR, The influence of environment, as represented by diet and air pollution, upon incidence and prevalence of wheezing illnesses in young children, Curr Opin Allergy Clin Immunol, 2011;11:144–9. Uhari M, Mäntysaari K, Niemelä M, A meta-analytic review of the risk factors for acute otitis media, Clin Infect Dis, 1996;22:1079–83. Pickering LK, Granoff DM, Erickson JR, et al., Modulation of the immune system by human milk and infant formula containing nucleotides, Pediatrics, 1998;101:242–9. Bousquet J, Fiocchi A, Prevention of recurrent respiratory tract infections in children using a ribosomal immunotherapeutic agent: a clinical review, Paediatr Drugs, 2006;8:235–43. Schaad UB, Prevention of paediatric respiratory tract infections: emphasis on the role of OM-85, Eur Respir Rev, 2005;14:74–7. Klein JO, Nonimmune strategies for prevention of otitis media, Pediatr Infect Dis J, 2000;19:S89–92. Graham NM, The epidemiology of acute respiratory infections in children and adults: a global perspective, Epidemiol Rev, 1990;12:149–78. Teele DW, Klein JO, Rosner B, Epidemiology of otitis media during the first seven years of life in children in greater Boston: a prospective, cohort study, J Infect Dis, 1989;160:83–94. Brook I, Gober AE, Dynamics of nasopharyngitis in children, Otolaryngol Head Neck Surg, 2000;122:696–700. Wilson R, Bacteria, antibiotics and COPD, Eur Respir J, 2001;17:995–1007. Bacharier LB, Guilbert TW, Diagnosis and management of early asthma in preschool-aged children, J Allergy Clin Immunol, 2012;130(2):287–96 Shaheen SO, Barker DJ, Shiell AW, et al., The relationship between pneumonia in early childhood and impaired lung function in late adult life, Am J Respir Crit Care Med, 1994;149:616–9. McCutcheon H, Fitzgerald M, The public health problem of acute respiratory illness in childcare, J Clin Nurs, 2001;10:305–10. Banz K, Thomas AM, Olivieri D, Economic evaluation of ribosomal immunotherapy in patients with chronic ear, nose and throat and respiratory tract infections: results for Italy, BioDrugs, 1998;10:385–96. Leder K, Sinclair MI, Mitakakis TZ, et al., A community-based study of respiratory episodes in Melbourne, Aust N Z J Public Health, 2003;27:399–404. Lambert SB, O'Grady KF, Gabriel SH, Nolan TM, Respiratory illness during winter: a cohort study of urban children from temperate Australia, J Paediatr Child Health, 2005;41:125–9. 44. Lambert S, O'Grady KA, Gabriel S, et al., The cost of seasonal respiratory illnesses in Australian children: the dominance of patient and family costs and implications for vaccine use, Commun Dis Intell, 2004;28:510–6. 45. Felmingham D, Feldman C, Hryniewicz W, et al., Surveillance of resistance in bacteria causing community-acquired respiratory tract infections, Clin Microbiol Infect, 2002;8 Suppl 2:12–42. 46. International Consensus Report on the diagnosis and management of rhinitis. International Rhinitis Management Working Group, Allergy, 1994;49:1–34. 47. Hoberman A, Marchant CD, Kaplan SL, Feldman S, Treatment of acute otitis media consensus recommendations, Clin Pediatr (Phila), 2002;41:373–90. 48. Peterson LR, Squeezing the antibiotic balloon: the impact of antimicrobial classes on emerging resistance, Clin Microbiol Infect, 2005;11 Suppl 5:4–16. 49. Gillis LM, White HD, Whitehurst A, Sullivan DC, Vancomycintolerance among clinical isolates of Streptococcus pneumoniae in Mississippi during 1999-2001, Am J Med Sci, 2005;330:65–8. 50. Akins RL, Haase KK, Gram-positive resistance: pathogens, implications, and treatment options: insights from the Society of Infectious Diseases Pharmacists, Pharmacotherapy, 2005;25:1001–10. 51. Jacobs RF, Judicious use of antibiotics for common pediatric respiratory infections, Pediatr Infect Dis J, 2000;19:938–43. 52. Riboldi P, Gerosa M, Meroni PL, Pidotimod: a reappraisal, Int J Immunopathol Pharmacol, 2009;22:255–62. 53. Bosisio D, Salogni L, Nowak N, et al., OM-85 shapes dendritic cell activation into a ‘pre-alert’ phenotype, Eur Respir J, 2011;38(Suppl 55):701s. 54. Gutierrez-Tarango MD, Berber A, [In Process Citation], Clin Drug Investig, 1997;13:76–84. 55. Razi CH, Harmanci K, Abaci A, et al., The immunostimulant OM-85 BV prevents wheezing attacks in preschool children, J Allergy Clin Immunol, 2010;126:763–9. 56. Quezada A, Maggi L, Pérez MA, Rodríguez J, Effect of bacterial antigen lysate on IgG and IgA levels in children with recurrent infections and hypogammaglobulinemia, J Investig Allergol Clin Immunol, 1999;9:178–82. 57. Karaca NE, Gulez N, Aksu G, et al., Does OM-85 BV prophylaxis trigger autoimmunity in IgA deficient children?, Int Immunopharmacol, 2011;11:1747–51. 58. Schaad UB, Farine JC, Fux T, [Prospective placebo-controlled double-blind study using a bacterial lysate in infections of the respiratory tract and ENT region in children], Helv Paediatr Acta, 1986;41:7–17. 59. Jara-Pérez JV, Berber A, Primary prevention of acute respiratory tract infections in children using a bacterial immunostimulant: a double-masked, placebo-controlled clinical trial, Clin Ther, 2000;22:748–59. 60. Schaad UB, Mutterlein R, Goffin H, BV-Child Study Group, Immunostimulation with OM-85 in children with recurrent infections of the upper respiratory tract: a double-blind, placebo-controlled multicenter study, Chest, 2002;122:2042–9. 61. Zagar S, Löfler-Badzek D, Broncho-Vaxom in children with rhinosinusitis: a double-blind clinical trial, ORL J Otorhinolaryngol Relat Spec, 1988;50:397–404. 62. Del-Rio-Navarro BE, Luis Sienra-Monge JJ, Berber A, et al., Use of OM-85 BV in children suffering from recurrent respiratory tract infections and subnormal IgG subclass levels, Allergol Immunopathol (Madr), 2003;31:7–13. 63. Gutiérrez-Tarango MD, Berber A, Safety and efficacy of two courses of OM-85 BV in the prevention of respiratory tract infections in children during 12 months, Chest, 2001;119:1742–8. 115