Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
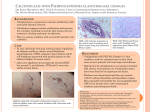
Danielle N. Butto DPM, AACFAS1 , Melissa Gulosh DPM, PGY-32 , Jeffrey Martone DPM, FACFAS2 1Fellow, Statement of Purpose Case review of a case of calciphylalxis with the first presenting lesion on the heel. The patient was evaluated initially and found to have no heel lesions. Six days after initial evaluation, the service was re-consulted for a pressure ulceration to heel which was found to be calciphylaxis. This study serves to review calciphylaxis and its characteristics. Literature Review It is estimated that calciphylaxis occurs in 1-4% of dialysis patients each year with a female preponderance of 3:1.1,2 It is more common in Caucasian females.3 Painful, violaceous mottled skin lesions that progress to plaque and/or nodules are the first dermatologic changes. The lesions progress to nonhealing ulcerations that ultimately develop eschar formation and gangrene.4 Calciphylaxis is seen in the lower extremities in 90% of cases.2 Sepsis from infected ulcers is a frequent cause of death. Peripheral pulses are often preserved and favor the diagnosis of calciphylaxis.1 Laboratory findings typically include increased parathyroid hormone levels, seen in 80% of patients, and elevated calcium and phosphorus concentrations2. Calcium-phosphorus product levels greater than 70 mg/dl favors the diagnosis of calciphylaxis.1 Elevated levels of alkaline phosphatase and low serum albumin are also frequently observed. Radiographic evaluation may demonstrate pipe-stem pattern of vascular calcification.3 Less concrete associations have been made between low protein C and S levels as well5. A high index of suspicion is critical for making the diagnosis of calciphylaxis especially in light of normal lab values. Risk factors include end stage renal disease, long term dialysis, female gender, obesity (BMI >30), presence of autoimmune disorder, and a hypercoagulable state. In addition, the administration of certain medications is associated with an increased risk of developing calciphylaxis. These medications include warfarin, systemic corticosteroids and high dose vitamin D6. Ankle and Foot Care Centers, Youngstown OH, 2 St Francis Hospital and Medical Center, Hartford CT Case Study Case Study Analysis and Discussion A 61y Hispanic female presented to ED, from a skilled nursing facility, with a temperature of 102.5⁰F with complaints of thigh redness and swelling, abdominal pain, nausea, and vomiting. Past medical history was significant for asthma, congestive heart failure, hypertension, gastroesophageal reflux disease, chronic renal failure (dialysis started Aug 2012), diabetes mellitus, rheumatoid arthritis (on chronic steroids), chronic leukocytosis, depression, anxiety, and a history of an embolic CVA (on Coumadin). Past surgical history was significant for I&D of posterior right thigh abscess and bilateral total knee replacements. She had no history of smoking, alcohol, or intravenous substance abuse. Her white count on admission was 31.1. Patient was admitted with the diagnoses with urinary tract infection, cholelithiasis, questionable BONE SCAN FINDINGS clostridium difficile, and bilateral lower extremity cellulitis. Antibiotics were initiated to include oral Vancomycin, intravenous Flagyl, and intravenous Ancef. Further lab work performed on the floor revealed an albumin of 2.0 (normal range 3.5-5.0), prealbumin 8.9 (normal range 17-42), fibrinogen 367 (normal range 204-431), phosphorus 1.9 mg/dl (normal range 2.5-4.5), alkaline phosphatase 313 U/L (normal range 38-126). Podiatry was consulted on hospital day 10. Physical examination revealed palpable dorsalis pedis and HISTOLOGIC FINDINGS posterior tibial pulses bilateral. A superficial ulcer was noted at the calcaneal-cuboid joint of the left foot with no purulence, no malodor, and no probing. Patient was also noted to have a right posterior leg superficial ulceration with no purulence, no malodor, and no probing. No erythema was noted to either lower extremity at this time. X-Ray imaging showed evidence of previous Charcot of the left foot without periosteal reaction and no evidence of osteomyelitis. Continued The hallmark signs of calciphylaxis must be kept in mind when assessing the patient. Affected patients will usually have intact peripheral pulses, bilateral necrosis, and frequent involvement of the lower extremity6 The clinical manifestations of calciphylaxis are similar to those of other vascular disorders therefore making diagnosis difficult. Disorders that share the characteristics of calciphylaxis include:Arteriosclerosis, DIC, Coumadin necrosis, connective tissue disorders, CREST and Scleroderma. Arteriosclerosis/cholesterol embolus is a disease process of the mediumlarge arteries rather than the small-medium. Necrosis is generally seen at the tips of the digits. Unlike vasculitis, there are very few inflammatory cells in and around the blood 7 .vessels unless the skin is secondarily infected Disseminated intravascular coagulation presents similar to a deep vein thrombosis with persistent bleeding from puncture sites. Scleroderma/CREST patients typically have Raynaud’s phenomenon along with swelling of the distal extremities and polyarthralgia. Hematology/Oncology was consulted with recommendations that stated the patient had a vitamin D deficiency secondary to malabsorption/diarrhea, as well as malnutrition. Treatment included vitamin D therapy. Serology for vasculitis was negative Six days after the initial podiatric evaluation, the patient had developed a left posterior heel ulceration with periwound erythema and a necrotic base. Reexamination of the extremities two days later revealed violaceous tissue with patches of necrosis to bilateral legs. Further laboratory work was ordered showing normal calcium (8.2), normal phosphorus (3.7) and normal parathyroid hormone (56.9). A biopsy was performed which revealed “Multifocal calcium deposition, including calcification of small and medium size vascular structures with ischemic change. Histologic findings consistent with calciphylaxis”. The patient was started on Sodium Thiosulfate 25g IV MWF. CT SCAN FINDINGS Analysis and Discussion Discussion and Conclusion Continued The gold standard for diagnosis of calciphylaxis is biopsy. There is no pathognomonic feature of calciphylaxis on histologic examination; however, the most consistent microscopic feature is acute and chronic panniculitis with a predominantly septal pattern. In addition, micro-calcifications in small to medium sized venules are appreciated8. A high index of suspicion is required when diagnosing and treating calciphylaxis. The early stages of the disease often mimic other disease processes. This particular case was complicated by the presenting lesions location of the heel. The patient was thought to have a decubitus ulceration. It was not until a review of the patient’s notes that it was noted she was lesion free on admission. In addition, the patient’s laboratory results were within normal limits. The patient’s co-morbidities along with the rapid progression of necrosis led to the decision to biopsy. Initiation of treatment in a timely fashion resulted in preservation of the patient’s limb, while preventing sepsis. . References 1. Figure 1: Initial evaluation of L heel and R lower extremity Figure 3: Histopathology of biopsy with calcifications in adipose Figure 2: L heel, L lower extremity and R lower extremity 6 days after initial evaluation Figure 4: L & R Lower Extremity after treatment w Sodium Thiosulfate Budisavljevic M, Cheek D, et al. Calciphylaxis in Chronic Renal Failure. Journal of the American Society of Nephrology. 1996;7 (7): 978-983. 2. Snyder R, Beylin M, et al. Calciphylaxis and Its Relation to End-Stage Renal Disease: A Literature Review and Case Presentation. Ostomy/Wound Management. 2000;46(10): 40-47 3. Tindni A, Gaurav K, et al. Non-healing painful ulcers in a patient with chronic kidney disease and role of sodium thiosulfate: a case report. Cases Journal. Sept 2008. 4. Weenig RH, Sewell LD, et al. Calciphylaxis: a natural history, risk factor analysis, and outcome. Journal of the American Academy of Dermatology. 2007;56: 569 5. Sanusi AA, Arogundade FA, et al. Calciphylaxis causing digital, gangrene in end stage renal disease: a case report and review. West Africa Journal of Medicine. 2013;32(1): 68-72 6. Santos P, Hartle JE, et al. Calciphylaxis. UpToDate. http://www.uptodate.com. Published 2012. Accessed January 25, 2013. 7. Cicone J, Petronis J, et al. Successful Treatment of Calciphylaxis With Intravenous Sodium Thiosulfate. American Journal of Kidney Diseases. 2004;43(6): 1104-1108 8. Essary L, Wick M. Cutaneous Calciphylaxis: An Underrecognized Clinicopathologic Entity. American Society of Clinical Pathologists. 2000;113: 280-287 9. Arteriosclerosis and Cholesterol Emboli. Merck Manuals. http://merckmanuals.com. Accessed September 22, 2013. 10. Goli AK, Goli SA, et al. Calciphylaxis: a rare association with alcoholic cirrhosis. Are deficiencies in protein C and S the cause? South Med J 2005; 98:736-9 11. Vasileios KC, et al. Calciphylaxis: A Pseudo-Vasculitis Syndrome. Seminars in Arthritis and Rheumatism. 2007;36(4):265-267