Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
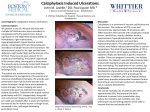
CALCIPHYLAXIS WITH PSEUDOXANTHOMA ELASTICUM-LIKE CHANGES DR. KARA HOVERSON, M.D. PGY-2, NATIONAL CAPITAL CONSORTIUM DERMATOLOGY RESIDENCY DR. WENDI WOHLTMANN, M.D DERMATOPATHOLOGIST, WILFORD HALL AMBULATORY SURGICAL CENTER B ACKGROUND • Calciphylaxis is a progressive vascular calcification with associated ischemic necrosis. • Calcification triggers intimal proliferation and narrows the arterioles resulting in necrotic skin lesions that are resistant to healing and prone to infections. • This is a serious condition with an overall mortality rate of 80-85%. C ASE • 74 year old female with past medical history significant for diabetes mellitus, obesity, atrial fibrillation, hyperlipidemia, COPD, congestive heart failure and B cell lymphoma presented with painful plaques on the bilateral thighs. No recent travel. • Labs were significant for persistently elevated BUN, but normal Cr and albumin. PTH and Ca were also within normal limits. H&E, 100x Calcium deposition in the wall of small to medium sized blood vessels along with thickened fibrous septae. H&E, 200x Thickened fibrous septa with "bramble bush" appearing elastic fibers (PXElike changes). D ISCUSSION • Calciphylaxis with PXE-like changes is a rare condition, with two reported cases to date. Both cases were in patients with end stage renal disease. • Risk factors for calciphylaxis in our patient included DM, obesity and warfarin use. Prothrombic states have been found to be important risk factor. • Warfarin was discontinued and she was treated with IV sodium thiosulfate and hyperbaric oxygen. She responded well initially but was hospitalized for CHF seven months later, with worsening of condition and subsequent death. Slightly indurated reticulated erythematous plaques on the bilateral thighs, some with central duskiness and ulcerations with clean moist bases. REFERENCES 1. Weenig RH, Sewell LD, Davis MD, McCarthy JT, Pittelkow MR. Calciphylaxis: Natural history, risk factor analysis and outcome. J Am Acad Dermatol. 2007 Apr;56(4):569-79. 2. Adrogué HJ, Frazier MR, Zeluff B, Suki WN. Systemic calciphylaxis revisited. Am J Nephrol. 1981;1(3-4):177-83. 3. Nikko AP, Buningan M, Cockerel CJ. Calciphylaxis with Histologic Changes of Pseudoxanthoma Elasticum. Am J Dermatopathol. 1996 Aug;18(4):396-9. 4. Lewis KG, Lester BW, Pan TD, Robinson-Bostom L. Nephrogenic fibrosing dermopathy and calciphylaxis with pseudoxanthoma elasticum-like changes. J Cutan Pathol. 2006 Oct;33(10):695-700.