Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
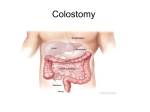
1/23/03 12:27 PM Page 19 THE OSTOMY FILES A LOOK AT THE PURPOSE AND OUTCOMES OF COLOSTOMY IRRIGATION F LI CA T NO T or nearly 75 years, colostomy irrigation has been an accepted management option that allows a colostomy patient to control bowel evacuation. Colostomy irrigation evolved as an answer to the nearly universally chronic peristomal skin problems caused by a lack of commercially available pouching systems, protective skin barriers, and skin care products.1 It was theorized that if the bowel could be evacuated once a day, no stool would seep onto the skin and, therefore, peristomal skin irritation would be minimized. Since that time, however, the procedure has gone in and out of acceptance by both patients and professionals — mostly due to fear of bowel perforation from irrigation catheters. This fear has been reversed by the introduction of soft catheter irrigation cones now available on most colostomy irrigation sets. For many years, nearly all colostomy patients were instructed on colostomy irrigation, but the outcomes were often less than satisfactory for the patient. Today, more realistic criteria have been developed to screen for those patients who have a better chance of success with it. Even though colostomy irrigation is not required to maintain bowel function, the procedure is a management option that may allow a patient to be free from fecal discharge for approximately 24 hours. The most important factors to evaluate in determining who is a candidate for colostomy irrigation are the patient’s clinical situation and lifestyle. For example, a patient with a sigmoid colostomy who has good manual dexterity and visual acuity, had regular bowel habits prior to surgery, is not undergoing chemotherapy, and is not DO taking medications that cause diarrhea may appear to be a perfect candidate. However, an assessment of the patient’s lifestyle reveals that he works “swingshift” hours and has an irregular work schedule. It would be nearly impossible for this patient to attempt colostomy irrigation at a regular time each day. Similarly, a physician writes orders for the home care nurse to teach a new patient how to irrigate. The initial home visit reveals that the patient lives in a setting without adequate bathroom facilities and running water. A patient’s inability to obtain control over bowel function in the manner prescribed by healthcare professionals can lead to feelings of frustration and failure, which decreases the overall quality of the patient’s life. A small prospective, crossover study in Singapore2 compared natural evacuation (ie, allowing the bowel to function on its own) to colostomy irrigation and found that colostomy irrigation after abdominoperineal resection was superior to natural evacuation in terms of cost and patient satisfaction. When patients irrigated, fewer peristomal skin problems, sleep disturbances, and sexual problems occurred. An overall decrease in management costs also was demonstrated due to a decrease in pouch usage. The study’s researchers recommended that colostomy irrigation be introduced to qualified patients soon after surgery. In an outcomes-oriented environment, clinicians should evaluate each patient on a case-by-case basis to determine if the patient can benefit from colostomy irrigation. Below are some criteria to consider during this assessment.3 Candidates should have: • a descending or sigmoid colostomy • a history of regular bowel habits prior to surgery • the desire to learn and perform the procedure • the ability (manual dexterity and visual acuity) to perform the procedure • a lifestyle that is compatible to irrigation (work schedule, bathroom facilities, adequate time, other family or personal issues). Patients with stomal prolapse or peristomal hernia should not be taught colostomy irrigation because performing the procedure could potentially exacerbate the DU P – Gwen B. Turnbull, RN, BS E 19-20, ostomyfiles February 2003 Vol. 49 Issue 2 19 19-20, ostomyfiles 1/23/03 12:27 PM Page 20 Accuzyme® Papain-Urea Debriding Ointment References DO NO T 1. Turnbull RW, Turnbull GB. The history and current status of paramedical support for the ostomy patient. Seminars in Colon and Rectal Surgery. 1991;2(2):131–140. 2. Peng Kheong Leong AF, Yunos ABM. Stoma management in a tropical country: colostomy irrigation versus natural evacuation. Ostomy/Wound Management. 1999;45(11):52–56. 3. Erwin-Toth P, Doughty DB. Principles and procedures of stomal management. In: Hampton BG, Bryant RA, eds. Ostomies and Continent Diversions: Nursing Management. St. Louis, Mo.: Mosby Year Book, 1992:29–103. 4. Venturini M, Bertelli G, Forno G, et al. Colostomy irrigation in the elderly. Effective recovery regardless of age. Dis Colon Rectum. 1990;33:1031–1033. The Ostomy Files is made possible through the support of ConvaTec, A Bristol-Myers Squibb Company, Princeton, NJ. Gwen B. Turnbull, RN, BS, author of The Ostomy Files, is a healthcare consultant specializing in public and private healthcare reimbursement as well as the development of professional and consumer educational and marketing tools. 20 OstomyWound Management LI CA T DESCRIPTION: Each gram of ACCUZYME enzymatic debriding ointment contains papain (8.3 x 105 USP units of activity based on lot H) and 100mg urea USP in a hydrophilic ointment base composed of purified water USP, emulsifying wax NF, glycerin USP, isopropyl palmitate NF, lactose NF, potassium phosphate monobasic NF, fragrance, methylparaben NF and propylparaben NF. CLINICAL PHARMACOLOGY: Papain, the proteolytic enzyme from the fruit of carica papaya, is a potent digestant of nonviable protein matter but is harmless to viable tissue. It is active over a pH range of 3 to 12. Papain is relatively ineffective when used alone as a debriding agent and requires the presence of activators to stimulate its digestive potency. In ACCUZYME, papain is combined with urea, a denaturant of proteins, to bring about two supplemental chemical actions: (1) to expose by solvent action the activators of papain, and (2) to denature the nonviable protein matter in lesions and thereby render it more susceptible to enzymatic digestion. Pharmacologic studies have shown that the combination of papain and urea result in twice as much digestive activity as papain alone. INDICATIONS AND USES: ACCUZYME is indicated for debridement of necrotic tissue and liquefication of slough in acute and chronic lesions such as pressure ulcers, varicose and diabetic ulcers, burns, postoperative wounds, pilonidal cyst wounds, carbuncles and miscellaneous traumatic or infected wounds. CONTRAINDICATIONS: ACCUZYME is contraindicated in patients who have shown sensitivity to papain or any other components of this preparation. PRECAUTIONS: See Dosage and Administration. Not to be used in eyes. ADVERSE REACTIONS: ACCUZYME is generally well-tolerated and nonirritating. A transient “burning” sensation may be experienced by a small percentage of patients upon applying ACCUZYME. Occasionally, the profuse exudate from enzymatic digestion may irritate the skin. In such cases, more frequent dressing changes will alleviate discomfort until exudate decreases. DOSAGE AND ADMINISTRATION: Cleanse the wound with ALLCLENZ® Wound Cleanser or saline. Avoid cleansing with hydrogen peroxide solution as it may inactivate the papain. Apply ACCUZYME directly to the wound, cover with appropriate dressing, and secure into place. Daily or twice daily applications are preferred. Irrigate the wound at each redressing to remove any accumulation of liquefied necrotic material. NOTE: Papain may also be inactivated by the salts of heavy metals such as lead, silver and mercury. Contact with medications containing these metals should be avoided. HOW SUPPLIED: 30g tube, 6g unit dose tube. Store in a cool place. Rx ONLY DU P prolapse or cause bowel perforation, leakage between irrigations, or poor control over elimination. Chemotherapy, pelvic or abdominal radiation treatments, a poor prognosis, and diarrhea-producing medication are also contraindications to colostomy irrigation. Age, on the other hand, should not be considered a contraindication, as colostomy irrigation has been shown to be effective regardless of the person’s age.2,4 Therefore, each individual should be carefully evaluated as a candidate. Once taught, the patient always has the choice to discontinue the procedure should it become incompatible with his or her lifestyle. However, the opportunity to learn the procedure exists for candidate patients throughout the duration of their treatment within the healthcare system (ie, home health care, outpatient clinic, doctor’s office, WOC nurse clinic). Colostomy irrigation is not the solution for all colostomy patients, but the decision to irrigate or not irrigate is ultimately the patient’s — not the healthcare professional’s. - OWM E NDC 0064-1000-01 (30g tube) NDC 0064-1000-07 (6g unit close tube) Distributed by: Healthpoint, Ltd. San Antonio, Texas 78215 1-800-441-8227 www.healthpoint.com Manufactured by: DPT Laboratories, Ltd. San Antonio, Texas 78215 REORDER NO. 0064-1000-01 (30g tube) 0064-1000-07 (6g unit dose tube) 127897-1002 Panafil® Healing, Debriding and Deodorizing Ointment NDC 0064-3410-30 (30g tube) NDC 0064-3410-07 (6g unit dose tube) Papain-Urea-Chlorophyllin Copper Complex Sodium DESCRIPTION: PANAFIL Ointment is an enzymatic healing-debriding ointment which contains standardized Papain, USP (not less than 521,700 USP units per gram of ointment), Urea, USP 10% and Chlorophyllin Copper Complex Sodium, USP 0.5% in a hydrophilic base composed of Purified Water, USP; Propylene Glycol, USP; White Petrolatum, USP; Stearyl Alcohol, NF; Polyoxyl 40 Stearate, NF; Sorbitan Monostearate, NF; Boric Acid, NF; Chlorobutanol (Anhydrous), NF as a preservative; Sodium Borate, NF. CLINICAL PHARMACOLOGY: Papain, the proteolytic enzyme derived from the fruit of carica papaya, is a potent digestant of nonviable protein matter, but is harmless to viable tissue. It has the unique advantage of being active over a wide pH range, 3 to 12. Despite its recognized value as a digestive agent, papain is relatively ineffective when used alone as a debriding agent, primarily because it requires the presence of activators to exert its digestive function. Urea is combined with papain to provide two supplementary chemical actions: (1) to expose by solvent action the activators of papain (sulfhydryl groups) which are always present, but not necessarily accessible, in the nonviable tissue or debris of lesions, and (2) to denature the nonviable protein matter in lesions and thereby render it more susceptible to enzymatic digestion. In pharmacologic studies involving digestion of beef powder, Miller1 showed that the combination of papain and urea produced twice as much digestion as papain alone. Chlorophyllin Copper Complex Sodium adds healing action to the cleansing action of the proteolytic papain-urea combination. The basic wound-healing properties of Chlorophyllin Copper Complex Sodium are promotion of healthy granulations, control of local inflammation and reduction of wound odors.2 Specifically, Chlorophyllin Copper Complex Sodium inhibits the hemagglutinating and inflammatory properties of protein degradation products in the wound, including the products of enzymatic digestion, thus providing an additional protective factor.1,3 The incorporation of Chlorophyllin Copper Complex Sodium in PANAFIL Ointment permits its continuous use for as long as desired to help produce and then maintain a clean wound base and to promote healing. INDICATIONS AND USES: PANAFIL Ointment is suggested for treatment of acute and chronic lesions such as varicose, diabetic and decubitus ulcers, burns, postoperative wounds, pilonidal cyst wounds, carbuncles and miscellaneous traumatic or infected wounds. PANAFIL Ointment is applied continuously throughout treatment of these conditions (1) for enzymatic debridement of necrotic tissue and liquefaction of fibrinous, purulent debris, (2) to keep the wound clean, and simultaneously (3) to promote normal healing. CONTRAINDICATIONS: None known. PRECAUTIONS: See Dosage and Administration. Not to be used in eyes. ADVERSE REACTIONS: PANAFIL Ointment is generally well-tolerated and nonirritating. A small percentage of patients may experience a transient “burning” sensation on application of the ointment. Occasionally, the profuse exudate resulting from enzymatic digestion may cause irritation. In such cases, more frequent changes of dressings until exudate diminishes will alleviate discomfort. DOSAGE AND ADMINISTRATION: Cleanse the wound with ALLCLENZ® Wound Cleanser or saline. Avoid cleansing with hydrogen peroxide solution as it may inactivate the papain. Apply PANAFIL directly to the wound, cover with appropriate dressing, and secure into place. Note: Papain may also be inactivated by the salts of heavy metals such as lead, silver and mercury. Contact with medications containing these metals should be avoided. When practicable, daily or twice daily changes of dressings are preferred. Longer intervals between redressings (two or three days) have proved satisfactory, and PANAFIL Ointment may be applied under pressure dressings. HOW SUPPLIED: 30g tube, 6g unit dose tube. Store at controlled room temperature (59°-86°F, 15°-30°C). Rx ONLY References 1. Miller, J.M.: The Interaction of Papain, Urea and Water-Soluble Chlorophyll in a Proteolytic Ointment for Infected Wounds, Surgery 43:939, 1958. 2. Smith, L.W.: The Present Status of Topical Chlorophyll Therapy, New York J. Med. 55:2041, 1955. 3. Barnard, R.D.: Elucidation of Chemically Defined Haptens for Competitive Inhibition of Aggressin Activity, Immunol. 8:78, 1954. Marketed by: Healthpoint, Ltd. San Antonio, Texas 78215 1-800-441-8227 www.healthpoint.com Manufactured by: DPT Laboratories, Ltd. San Antonio, Texas 78215 REORDER NO. 0064-3410-30 (30g tube) 0064-3410-07 (6g unit dose tube) 127898-1002