Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
9/6/14
Charles Dickens, The Pickwick Papers, 1837
Harly Greenberg, MD Medical Director North Shore-‐LIJ Sleep Disorders Center Division of Pulmonary, Critical Care and Sleep Medicine Professor of Medicine Hofstra North Shore-‐LIJ School of Medicine Case. 81 YOM with history of alcohol induced liver cirrhosis, congestive heart failure, dyslipidemia, hypertension and obesity presented to the sleep clinic for follow up after being discharged from the nursing home with bpap. In the past, treated for OSA, but treatment was recently discontinued by primary care physician after weight loss and patient’s report of decrease in snoring intensity. Few months later patient was hospitalized two times for hypercapnic respiratory failure, which was attributed to empiric diagnosis of COPD. Patient was discharged with bpap to the rehab, with empirically determined pressures, he did not undergo pressure titration. History. PMHx: Et-‐OH liver cirrhosis, HTN, HLD, CHF, obesity ( BMI:36kg/m2), chronic gastritis, CKD PSHx: hernia repair SocHx: non-‐specified street drugs, marijuana quit 40 years ago, alcohol overuse Allergies: NKDA Medications: aspirin, clopidogrel, furosemide, spironolactone, nadolol, lactulose, omeprazole, tamsulosin, advair 1
9/6/14
Labs/tests. On admission: November: 14
3
5
105
29
32
1.88
At discharge 132
142
4.5
107
29
29
1.64
ABG: 7.19/93/79/27/93% ABG: 7.31/67/51/29/85% January: 140
101
138
4.9
17
35
5.1
1.35
ABG: 7.14/104/67/29/91% 105
30
76
22
1.71
89
ABG: 7.41/52/82/31/98% CXR: Labs/tests. Observed
Predicted
% Reference
VC (liters)
1.6
2.7
61
FRC (Liters)
1.8
2.5
72
TLC
(liters)
3.7
4.6
74
Forced
expiration
Observed
Predicted
FEV1 (liters)
1.2
2.06
59
FVC (liters)
1.65
2.7
61
FEF25-75% (l/sec)
0.96
1.94
50
Diffusing capacity for
CO
(ml/min/mmHg)
13.6
23.4
58
Lung volumes and
compliance
FEV1/FVC %
75
2
9/6/14
What went wrong? What is the diagnosis? Why was it missed? What should be done now? Classifica6on of Overweight and Obesity Obesity Trends* Among U.S. Adults BRFSS, 2009 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person)
Behavioral Risk Factor Surveillance System, CDC No
NoData
Data
Data
No
<10%
<10%
10%–14%
10%–14%
10%–14%
15%–19% 20%–24%
20%–24%
15%–19%
25%–29%25%–29%
≥30%
≥30%
3
9/6/14
Obesity Hypoven6la6on Syndrome Score hypoventilation during sleep if EITHER of the below occur:
a. There is an increase in the arterial PCO2 (or surrogate) to a value >55
mmHg for ≥10 minutes.
b. There is ≥10 mmHg increase in arterial PCO2 (or surrogate) during sleep (in
comparison to an awake supine value) to a value exceeding 50 mmHg for
≥10 minutes.
Berry RB, Brooks R, Gamaldo CE, Harding SM, Lloyd RM, Marcus CL and Vaughn
BV for the American Academy of Sleep Medicine. The AASM Manual for the
Scoring of Sleep and Associated Events: Rules, Terminology and Technical
Specifications, Version 2.1. www.aasmnet.org, Darien, Illinois: American Academy
of Sleep Medicine, 2014.
Hypercapnia with OSA is unlikely to develop in pa6ents with BMI <30 kg/m2 RESPIRATORY CARE • OCTOBER 2010 VOL 55 NO 10 Prevalence of OHS Estimated prevalence of OHS in the general adult population 0.15% -‐0.3% As many as half a million individuals with OHS 10-‐20% of OSA 31% hospitalized adult patients with a BMI of >35 kg/m2 Because of cephalometric differences, OHS associated with OSA occurs at a lower BMI in Asians 4
9/6/14
Obesity Hypoven6la6on Syndrome Prevalence – Associa6ons with OSA 90% of OHS patients have OSA The prevalence of OHS in patients with an AHI greater than 60/hr is approximately 25% The prevalence of OHS in patients with OSA by BMI categories in the United States The prevalence of OHS in patients with OSA distributed by various AHI categories Clinical Presenta6on of OHS Middle-‐aged with a 2:1 male-‐to-‐female ratio Symptoms of OSA: hypersomnolence, loud habitual snoring, nocturnal choking episodes, and morning headaches. Dyspnea, lower extremity edema, and low oxygen saturation during wakefulness are common Elevated serum bicarbonate levels Restrictive defect seen on pulmonary function tests is common and is due to obesity. Pulmonary hypertension and cor pulmonale 5
9/6/14
Clinical features of 631 pa6ents with OHS Mokhlesi Chest 2007;132;1322-‐1336 Hypercapnia and elevated serum HCO3-‐ Elevated serum bicarbonate level due to the metabolic compensation for chronic respiratory acidosis Serum bicarbonate level is a reasonable test to screen for hypercapnia A serum bicarbonate >27 mEq/L sensitive (92%) although not specific (50%) for increased PaCO2, Pulse oximetry of less than 94% also suggests the need for an arterial blood gas measurement Arterial blood gas should be obtained to determine presence and severity of daytime hypercapnia in patients with obesity and OSA who have low waking SaO2 or elevated serum bicarbonate levels Hypercapnia and elevated serum HCO3 Sleep Breath 2007; 11:117–124 6
9/6/14
Hypercapnia and elevated serum HCO3 If hypercapnia is present, pulmonary function testing and chest imaging can be useful in excluding other causes of hypercapnia Overlap syndrome is the term used to describe the association of COPD and OSA Obstructive pattern on spirometry Thyroid function tests to exclude severe hypothyroidism and a CBC for secondary erythrocytosis. QOL and Comorbidi6es Moderate to severe dyspnea Peripheral edema, pulmonary hypertension, and cor pulmonale Pulmonary hypertension is more common (50% vs 15%, respectively) and more severe in patients with OHS than in those with OSA Lower quality of life measures Compared to patients with similar degrees of obesity, patients with OHS have: increased medical resource utilization more likely to be hospitalized more likely to require intensive care admission Greater cardiometabolic morbidity compared with OSAS or obesity alone. Increased prevalence of systemic hypertension, congestive heart failure, cor pulmonale, insulin resistance and angina Despite high contact with health care providers, there is a significant delay in the recognition of OHS and institution of definitive therapy Morbidity and Mortality of OHS Compared to patients with a similar degree of obesity but without hypoventilation, patients with OHS had higher rates of ICU admission (6% vs 40%, respectively) and a greater need for invasive mechanical ventilation 47 patients with OHS followed for 18 months after hospital discharge Mortality of patients with OHS was 23% compared to 9% in patients with a similar degree of obesity but without hypoventilation (hazard ratio: 4.0) Most deaths occurred in the first 3 months after hospital discharge Only 13% were discharged from the hospital with treatment for hypoventilation Am J Med 2004;116:1–7. 7
9/6/14
Obesity-‐associated hypoven6la6on in hospitalized pa6ents: prevalence, effects, and outcome. 23% mortality
Am J Med 2004;116:1–7. Pathophysiology of OHS EXCESSIVE LOAD ON THE RESPIRATORY SYSTEM 1. Mass loading from central obesity, ↑airway resistance Reduced respiratory system compliance compared to normal weight subjects Increased small airway resistance and overall respiratory system resistance ↑Work and energy cost of breathing-‐ 3 times normal in OHS 15% of oxygen consumption for work of breathing compared to 3% in nonobese individuals 3. Ferretti A, P, Cavalli A, Milic-‐Emili J, Tantucci C. Expiratory flow limitation and orthopnea in massively obese subjects.Chest 119: 1401–1408, 2001 2. Sharp JT, Henry JP, Sweany SK, Meadows WR, Pietras RJ. The total work of breathing in normal and obese men. J Clin Invest 43: 728–739, 1964. Pathophysiology of OHS 2. Increased upper airway resistance Lower lung volumes are associated with increased UA resistance Changes in UA resistance with increased BMI and reduced FRC 33% 49% 62% 30 kg/m2 35 kg/m2
40 kg/m2 Compared to BMI 20 8
9/6/14
Pathophysiology of OHS 3. Diaphragm dysfunction Mechanical overstretching due to increased abdominal mass ⇉length-‐tension disadvantage resulting in diaphragm fiber overstretching, worse supine Respiratory func6on in OHS Spirometry: low FVC and FEV1 and a normal FEV1/FVC ratio.-‐ restrictive pattern OHS Eucapnic obesity Comparison of lung volumes and awake blood gases in individuals with eucapnic morbid obesity (solid bars) and those with obesity hypoventilation syndrome (OHS; hatched bars). Data are composite values obtained from a number of studies reporting respiratory function in morbidly obese patients with and without hypoventilation Pathophysiology of OHS ABNORMALITIES OF CENTRAL RESPIRATORY DRIVE VENTILATORY RESPONSE TO CO2 Blunted ventilatory response to hypercapnia May improve with PAP therapy 9
9/6/14
Lep$n Product of the adipocyte-‐specific ob gene, leptin primarily regulates food intake and energy expenditure Leptin is also a ventilatory stimulant Leptin deficient ob/ob mouse – obese, attenuated hypercapnic ventilatory response, rapid shallow breathing pattern, reversed by leptin replacement However, in human OSA/OHS leptin is increased in relation to obesity Patients with OHS have a higher serum leptin levels than eucapnic subjects with OSA matched for percentage of body fat and AHI Serum leptin decreases after treatment with PAP
suggests that patients with OHS might be resistant to leptin
Effects of chronic hypoxia – may cause leptin resistance How could obstruc$ve sleep apnea lead to chronic day$me hypercapnia? Respiratory effects of obesity cannot be the only determinant of hypoventilation since hypercapnia develops in less than one third of morbidly obese individuals and in only 10-‐20% of obese OSA patients Obstructive apneas during sleep are a major contributing factor to the pathogenesis of daytime hypoventilation in OHS since resolution of awake hypercapnia occurs in most (not all) patients with OSA/OHS treated with PAP therapy or tracheostomy 10
9/6/14
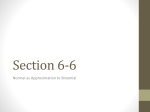
Nocturnal hypoven$la$on induced by sleep-‐
disordered breathing Sleep-‐disordered breathing can occur in the following three forms: Obstructive apneas Flow Effort Chest Abd Sum Obstructive hypopneas Flow Effort Chest Abd Sum Nocturnal hypoven$la$on induced by sleep-‐
disordered breathing Central apneas Flow Effort Chest Abd Sum 11
9/6/14
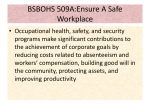
5 minutes Apnea Interapnea ventilation Pathophysiology apnea
Interapnea
breaths
Considerations of Obesity Hypoventilation Syndrome
Pathophysiology Fig. 3. Interapnea/hypopnea hyperventilation and carbon dioxide (CO2) excretion. In the first cycle, the interevent hyperpnea is
sufficient to excrete the carbon dioxide accumulated during hypopnea. In the second cycle, much more carbon dioxide is
accumulated during apnea than is excreted after the event. Multiple cycles of excessive carbon dioxide accumulation during
the apneic period lead to hypercapnia. (Adapted from reference 35 with permission.)
Upper Airway Obstruction
Patients with OHS display increased upper airway resistance
in both the sitting and supine position in comparison with
obese individuals with eucapnia.47 This may contribute to
the increased work of breathing found in OHS patients.48
Respiratory Mechanics
Simple obesity impairs respiratory mechanics leading to reduced lung volumes, decreased chest wall compliance, increased respiratory resistance, and increased work of breathing.49,50 These parameters are further impaired in OHS
patients (table 2). Spirometric values from patients with
OHS typically reveal a restrictive pattern with a reduction in
FEV1 and FVC but normal FEV1/FVC. Functional residual
capacity, total lung capacity, and expiratory reserve volume
oxygen consumption, carbon dioxide production, and work
of breathing.30,31,49 Obese individuals have a substantially
increased central respiratory drive compared with normalweight patients to compensate for the increased ventilatory
requirements.50 In contrast, patients with OHS have a
blunted central respiratory drive to both hypercapnia and
hypoxia. They do not hyperventilate to the same degree as
obese individuals with eucapnia when forced to rebreathe
carbon dioxide43,52,53 or breathe a hypoxic gas mixture.53
The blunting of central respiratory drive may result from
leptin resistance and sleep-disordered breathing.29,34
Pulmonary Hypertension
The incidence of pulmonary hypertension, as defined by a
mean pulmonary arterial pressure !20 mmHg, is higher in
12
9/6/14
Chronic hypercapnia In the majority of OSA patients hypercapnia does not occur. Compensation for acute hypercapnia that develops during an apnea is adequate to maintain overall eucapnia for the night. In OHS there is inadequate interapnea ventilation to compensate for CO2 that accumulates during an apnea, with an overall increase in CO2 load across the night. This leads to renal HCO3-‐ retention that further blunts the ventilatory response to CO2 Pathophysiology of OHS EDUCATION
Fig. 2. Mechanisms by which obesity and OSA result in chronic hypercapnia. HCO3! " serum bicarbonate; OSA " obstructive
sleep apnea.
Mokhlesi, B et al., Recent Advances in Obesity Hypoventilation Syndrome, Chest respiratory mechanics because of obesity, leptin resistance
leading to central hypoventilation, and impaired compensatory response to acute hypercapnia in OSA (fig. 2).3,21
obstructive events and renal bicarbonate retention, are required
to maintain carbon dioxide homeostasis.34 Chronic hypercapnia in OHS may occur if these compensatory responses are
impaired. In eucapnic subjects with OSA, periods of apIncreased Mechanical Load and Impaired
nea are separated by periods of hyperventilation such that
Respiratory Mechanics
the accumulated carbon dioxide load is eliminated.35
Obesity imposes a significant load on the respiratory system and
However, when apneas become three times longer than the breathcould result in hypoventilation secondary to fatigue and the
ing interval, carbon dioxide accumulates (fig. 3).35
relative weakness of the respiratory muscles.22–24 Several studies
Patients with OHS, in comparison with those with euthat compare patients with OHS with individuals who are eucapnia, have a reduced duration of ventilation between pericapnic and obese have noted a significantly higher BMI in the
ods of apnea.36 This is possibly related to a gradual adaptaOHS group.10,14,16,25 However, because less than a third of the
tion of chemoreceptors secondary to mild elevation of serum
morbidly obese individuals develop hypercapnia, other mechaHCO3! that can occur even during acute hypercapnia. In
nisms may result in hypoventilation.10,16,26
eucapnic individuals, arterial carbon dioxide tension is restored to normal during wakefulness and the excess HCO3! is
Leptin Resistance
excreted. However, a transition from acute to chronic hypercapLeptin is a protein produced specifically by the adipose tissue
nia
may
result t
ifherapy the small amount
retained HCO3! is not
Improve nocturnal ventilation with PAP to ofimprove that regulates appetite and energy expenditure.27–29 It
excreted by the kidneys, leading to a reduction of ventilatory
crosseschronic the blood-brain
barrier and exerts
its effect throughand daytime hypercapnia hypoxia carbon
dioxide responsiveness. In a computer model, when
28
binding to leptin receptors in various areas of the brain. In
both carbon dioxide response and the rate of renal HCO3!
patients,
CPAP a higher
is effective in ost patients with HS who ave obese
level of leptin
is m
found
causing
an
excretion
wasO
abnormally
low, h
a rise
in awake arterial carbon
increase in ventilation to compensate for the increased cardioxide tension
concomitant O
SA C
hest 2
007; 1
31:1678–1684
and HCO3! developed over multiple days.37
bon dioxide production associated with excess body
mass.27,30,31
Patients
OHS exhibit
an even
higher
se 57% of with
OSA/OHS pts: CPAP therapy resolved sleep-‐disordered Do Patients with OHS Possess Different Clinical
rum leptin level than eucapnic individuals matched for BMI,
breathing and nocturnal hypoxemia Features than Obese Patients with Eucapnia?
and their serum leptin level drops after positive airway pres32,33
Compared
with obese
patients
with eucapnia, patients with
sure (PAP)
therapy.
These observations
suggest leptin
43% of OSA/OHS: refractory hypoxemia during CPAP titration OHS demonstrate four main clinical features: more severe
resistance may contribute to the hypoventilation in OHS.
upper airway obstruction, impaired respiratory mechanics,
Improvement in daytime blunted central respiratory drive, and increased incidence
Impaired Compensation of Acute Hypercapnia in
blood Breathing
gas levels is achieved of pulmonary hypertension. Table 2 compares various reSleep-disordered
ported demographic and physiologic parameters between
Obstructive apneas, hypopneas, and long periods of hy as early s 1 result
month after the of patients with OHS and obese patients with eucappoventilation
during a
sleep
in transient
episodes
nia.5,10,11,14,16,25,26,38 – 46 The clinical features of OHS are
acute hypercapnia. Compensatory mechanisms, including
s
tart o
f P
AP t
herapy
hyperventilation during brief periods of arousal between the
summarized in figure 4.
Therapy of OHS However, up to 25% of patients Anesthesiology 2012; 117:188 –205
191
who are adherent to CPAP therapy do not become eucapnic Chau et al.
13
9/6/14
Bilevel Posi6ve Airway Pressure Therapy Bilevel or NPPV should be considered if during CPAP titration the oxygen saturation remains persistently below 90% after the resolution of apneas, hypopneas, and flow limitation with CPAP if the Paco2 does not normalize with CPAP Bilevel PAP is more effective than CPAP therapy in improving awake hypercapnia (decrease in Paco2, 7.8 vs 5.3 mm Hg) Proc Am Thorac Soc 2005; 2:A613 Bilevel PAP Pressure support Bilevel PAP How to titrate Bilevel PAP: EPAP should be increased until there is resolution of obstructive respiratory events (apneas). If the oxygen saturation remains persistently below 90% after the resolution of apneas, hypopneas, and flow limitation, inspiratory PAP (IPAP) should be added to the final EPAP to improve ventilation. IPAP was at least 8 to 10 cm H2O above EPAP (Pressure support of 8 to 10 cmH2O) in the studies that showed successful long-‐term resolution of hypercapnia and hypoxia with bilevel PAP therapy 14
9/6/14
Newer modali6es Average Volume-‐Assured Pressure Support Six weeks of therapy with AVAPS was more successful than bilevel PAP therapy in improving nocturnal and daytime ventilation (mean transcutaneous CO2 during sleep, 45.3 vs 52.4 mm Hg, respectively; mean daytime Paco , 42.5 vs 46.4 mm Hg, respectively). Changes in sleep quality and quality of life were similar between the two modes of ventilation Chest 2006; 130:815–821 Set the target tidal volume to 8 ml/kg of
ideal weight
Set respiratory rate 2-3 BPM below resting
respiratory rate
Adjust EPAP to eliminate obstructive
events; auto EPAP
2
15
9/6/14
Management of pa6ents with OHS with acute-‐on-‐chronic hypercapnic respiratory failure 16
9/6/14
Survival rates in OHS with and without long term NIV Am. J. Respir. Crit. Care Med. December 15, 2012 vol. 186 no. 12 1205-1207
Considerations of Obesity Hypoventilation Syndrome
Fig. 4. Clinical features of the patient with obesity hypoventilation syndrome.
weight reduction surgery, and pharmacologic respiratory
stimulants.
ventilatory defect is assumed to be due to a decrease in the
premature closure of dependent airways during expiration
and to an opening of microatelectasis. Lin only reported a
trend toward improved FEV1 with 4 weeks of CPAP.71
PAP Therapy: Short-term and Long-term Benefits
However, the course of treatment was much shorter than
The two main forms of PAP therapy currently being used
that examined by the other three studies (24 – 48 weeks).
are continuous positive airway pressure (CPAP) and biFive studies evaluated the effects of PAP on central respilevel PAP.
ratory drive, as measured by carbon dioxide sensitivity, calShort-term benefits of PAP include an improvement in
culated as the change in minute ventilation per unit change
gas exchange and sleep-disordered breathing (tables 3 and 4).
in end-tidal carbon dioxide (table 4).41,70,71,77,80 Three studThere were five studies that evaluated the effects of a short
ies demonstrated a significant increase in carbon dioxide sencourse (! 3 weeks) of PAP on PaCO2 and PaO2.63,70 –73 All
sitivity, whereas the other two studies reported a trend tofive studies reported a significant decrease in PaCO2 and four
ward an increase in carbon dioxide sensitivity.
studies reported a significant increase in PaO2. One possible
PAP may also reduce mortality in OHS. Two retrospecexplanation for the single study that showed a nonsignificant
tive studies have demonstrated a mortality rate of 13–19% in
change in PaO2 could be related to the short duration of
patients with OHS on PAP throughout a mean period of 4
70
therapy (five nights). There were four studies that studied
yr.76,79 Through indirect comparison, this mortality rate is
the benefits of short-term PAP on sleep-disordered breathlower than the 23% mortality rate reported in patients with
ing.70 –72,74 All four studies reported a significant improveuntreated OHS at 18 months of follow-up (fig. 5).5
CPAP therapy is eduring
ffective of stable patients with OHS, ment in
AHI
and oxygen
saturation
sleep. in the majority In summary, short-term (!3 weeks) PAP therapy imparticularly in include
the san
ubgroup of pinatients ho have sand
evere OSA breathing. In adLong-term
benefits of PAP
improvement
proveswgas
exchange
sleep-disordered
gas exchange, lung volumes, and central respiratory drive to
long-termw("4
PAP
therapy improves
Bilevel PAP therapy should be used dition,
in patients ho weeks)
do not respond to lung
carbon dioxide. Nine studies examined the relationship bevolumes
and
central
respiratory
drive to carbon dioxide and
CPAP atients with (table
OHS who experience acute-‐on-‐chronic tween long-term
PAPtherapy, ("4 weeks)pand
gas exchange
lowers mortality. Because of its noninvasiveness and effec75– 83
respiratory f
ailure, a
nd i
n p
atients w
ho h
ave O
HS w
ithout O
SA All but one study showed a significant improvement
3).
tiveness, PAP is considered the first-line therapy for OHS.
PaO2.
in PaCO2 and
AVAPS-‐ new modality There were four studies that investigated the effects of
Efficacy of Bilevel PAP versus CPAP
Treatment o
f O
HS w
ith P
AP i
mproves blood as levels, morning 71,76,77,84
Three
long-term PAP on FEV1 and FVC (table 5).
CPAP
failure,gdefined
by a residual
AHI "5 or a mean nocheadaches, excessive daytime sleepiness, dOyspnea, pulmonary of the four studies
found a significant
improvement
in pulturnal Sp
2 !90%, has been documented in some patients
hypertension, and studies
leg edid
dema. monary function.
Two of the positive
not report
with OHS. These nonresponders improved after treatment
81
a significant
change in BMI.lThis
of restrictive
bilevel PAP.
Decreased ong improvement
term mortality with with
NPPV Summary Improvements in symptoms and b
lood gas levels are directly related Chau et al.
194
to adherence with therapy Changes in serum bicarbonate level and pulse oximetry could be used as a less invasive measure of success of nocturnal ventilation 2012; 117:188 –205
Anesthesiology
17