Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
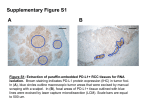
Targeted immunotherapy: unleashing the immune system against cancer Suzanne L. Topalian, MD Johns Hopkins University School of Medicine Sidney Kimmel Comprehensive Cancer Center 2013 MMS Annual Education Program: Navigating the Currents of Change Disclosure Information Suzanne L. Topalian, MD I have the following financial relationships to disclose: – Consultant for: Bristol-Myers Squibb (uncompensated), Jounce Therapeutics, Sanofi, and Amplimmune (spouse) – Research grant support from Bristol-Myers Squibb – Royalties through institution: Amplimmune (spouse), Bristol-Myers Squibb (spouse) “Cancer is a genetic disease” rationale for personalized medicine limitation: rapid resistance Cancer is an immunological disorder immunotherapy is a common denominator that can activate immune responses against mutant proteins the adaptable immune system can keep pace with tumor evolution The adaptive immune system: an “ideal” anti-cancer agent Diversity T cells - 1018 Antibodies - 1022 Specificity Can distinguish minute chemical alterations Tumor cell T cell Memory After effective antigen priming, immunity can last for decades Immune tolerance: Multiple barriers to tumor elimination Regulatory immune cells T reg cells MDSCs T-cell inhibitory receptors CTLA-4, PD-1, LAG-3, etc. Immunosuppressive cytokines IL-6, IL-10, TGF-ß, VEGF Solution: adoptive transfer of T cells optimized/engineered ex vivo Solution: systemic blockade of suppressive cytokines or inhibitory receptors/ligands (“immune checkpoints”) Advances in Immunotherapy 2011 Anti-CTLA-4 (ipilimumab) was approved for treating metastatic melanoma based on improved overall survival in a randomized study. However, the grade 3-4 drug-related toxicity rate approximated the clinical benefit rate Adapted from Hodi et al, NEJM 2010 Ipilimumab Control Antigen presenting or tumor cell PD-L1 is expressed by many human tumors and may play a pivotal role in local cancer immunosuppression T cell The PD-1/PD-L1 pathway: New strategies for immune checkpoint blockade Pardoll 2012 Role of PD-1 in suppressing antitumor immunity Activation (cytokines, lysis, prolif., migration) APC T cell B7.1 MHC-Ag CD28 TCR Signal 1 (-) (-) (-) PD-1 PD-L1 Inhibition Tumor (anergy, exhaustion, death) Tumor Role of PD-1 in suppressing antitumor immunity Activation (cytokines, lysis, prolif., migration) APC T cell B7.1 MHC-Ag CD28 TCR Signal 1 (-) (-) (-) AntiPD-1 PD-1 PD-L1 Inhibition Tumor (anergy, exhaustion, death) Tumor CTLA-4 vs. PD-1: Distinct immune checkpoints B7.1/2 APC CD28 signal 1 CTLA-4 to surface APC Costim. ligand Costim. receptor signal 1 Traffic to periphery signal 1 CTLA-4 Naïve/resting T cell APC + Experienced T cell Tissue PD-L1 T cell priming Topalian et al., Curr Opin Immunol 2012 signal 1 PD-1 Nivolumab (anti-PD-1) (BMS-936558, MDX-1106, ONO-4538) Fully human IgG4 anti-human PD-1 blocking mAb High affinity for PD-1 (KD ~ 3 nM), blocks binding to both known ligands: PD-L1 (B7-H1, broadly inducible) and PD-L2 (B7-DC, selective for APCs) Favorable safety profile and preliminary evidence of clinical activity in patients with treatment-refractory solid tumors in a first-in-human study (Brahmer et al., J Clin Oncol 2010) Two early phase clinical trials of anti-PD-1 (nivolumab) in patients with advanced solid tumors (Brahmer et al., JCO 2010; Topalian et al., NEJM 2012) 1st Treatment Cycle Day 1 Dose 0.3-10 mg/kg Day 57 Scans 43 Day 85 Scans 2 years or until CR/PR or PD Follow Up or Additional Treatment Cycle(s) 1st Treatment Cycle Days 1, 15, 29 Dose 0.1-10 mg/kg Follow Up or Additional Treatment Cycle(s) Day 57 Scans 2 years or until CR or PD Eligible patients: treatment-refractory metastatic lung cancer, melanoma, kidney, colon, or prostate cancer CRC Durable anti-PD-1 responses OFF THERAPY: immune memory CR Stop Rx Latest eval.: CR (Lipson et al., CCR 2013) 0 1 yr RCC Stop Rx Best resp.(PR) 0 1 yr 1 yr 3 yr CR 2 yr Stop Best Rx resp.(PR) MEL 0 2 yr 2 yr 4 yr Latest eval.: CR 3 yr 4 yr 5 yr New LN met Resume Rx PR Latest eval. PR 3 yr 4 yr 5 yr Clinical activity of anti-PD-1 (nivolumab) ORR (CR/PR) SD 24 wk No. pts (%) No. pts (%) Tumor Type Dose (mg/kg) No. pts NSCLC 1-10 122 20 (16) 11 (9) MEL 0.1-10 106 33 (31) 6 (6) RCC 1 or 10 34 10 (29) 9 (27) 294 patients started therapy between 2008-2012 and had ≥6 mo. follow-up. No ORs in CRC (n=19) or CRPC (n=17) 28/54 responses lasted ≥1 yr in patients with ≥1 yr follow-up Toxicity: grade 3-4 drug-related AEs15%, mortality 1%. Topalian et al., ESMO 2012 Change in Target Lesions from Baseline (%) Anti-PD-1 response kinetics and durable tumor control off therapy 100 Melanoma 1 mg/kg 90 80 70 60 50 40 30 20 10 First occurrence of new lesion Maximum duration of therapy On study Off study 0 -10 -20 -30 -40 -50 -60 -70 -80 -90 -100 0 10 20 30 40 50 60 70 80 90 100 Weeks Since Treatment Initiation 110 120 130 140 Partial response of locally advanced primary melanoma to anti-PD-1 Pre Tumor Lymphs 2 mo. 35-year-old patient had disease progression after surgery and IL-2. Response to anti-PD-1 ongoing at 23 months. Partial regression of metastatic kidney cancer in response to anti-PD-1 Pretreatment 6 months 57-year-old patient developed progressive disease after receiving sunitinib, temsirolimus, sorafenib, and pazopanib Currently in cycle 12 anti-PD-1 therapy (~23 months) with ongoing PR Response of a “non-immunogenic” tumor to anti-PD-1: Squamous cell lung cancer Pre-Rx 2 months 12 months History: 61-year-old patient with stage IV NSCLC refractory to multiple surgeries, RT, 2 multidrug chemotherapy regimens, and epigenetic therapy (5-AZA and entinostat). Recently completed 2 yrs anti-PD-1 therapy. Drug-related AEs of special interest in ≥ 3% of 304 patients receiving anti-PD-1 AEOSI (“irAE”) All grades (n, %) Grade 3-4 (n, %) Any 138 (45) 18 (6) Rash 41 (14) 0 Diarrhea 36 (12) 3 (1) Pruritis 31 (10) 1 (0.3) ALT 13 (4) 2 (1) AST 11 (4) 2 (1) TSH 11 (4) 1 (0.3) Pneumonitis* 10 (3) 3 (1) Vitiligo 9 (3) 0 Infusion reaction 8 (3) 0 *There were 3 (1%) deaths in patients with pneumonitis (2 NSCLC, 1 CRC). AEOSIs in ≤1% of pts included colitis, hepatitis, hypophysitis, nephritis and thyroiditis. Analysis as of July 2012. Topalian et al, ESMO 2012 Partial response of metastatic mucosal melanoma to anti-PD-1, associated with nephritis Pre-Rx 8 months Prior therapies included multiple surgeries, RT and temozolomide. Nephritis developed after 8 months of antiPD-1 therapy, associated with administration of radiographic contrast dye. Nephritis associated with anti-PD-1 therapy: serologic and cellular immune components H&E, 400 X CD3 tubule glomerulus plasma cell intraepithelial T cell B7.1 PD-1 ? antiapoptotic signal in tumor cells PD-L1 PD-L2 Anti-PD-1 Anti-PD-L1 ? antiapoptotic signal in tumor cells (-) signal B7.1 PD-1 PD-L1 PD-L2 (-) signal If PD-1 pathway blockade acts locally in the tumor immune microenvironment………. Then it follows that the tumor site may hold the key to optimizing anti-PD-1/PD-L1 therapy: Biomarkers to select patients most likely to respond to therapy Early indicators of treatment outcomes Identification of resistance pathways and development of synergistic combinatorial therapies Melanoma Preliminary molecular marker studies: Correlation of PD-L1 expression in pretreatment tumor biopsies with clinical response to anti-PD-1 Proportion of patients 18/18 1 * 0.8 0.6 18/31 Kidney PD-L1(+) CR/PR PD-L1(-) NR 13/31 0.4 p=0.002 Lung 0.2 0/18 0 PD-L1(+) PD-L1(-) 49 patients include 20 with melanoma,13 NSCLC, 7 colon, 6 kidney, and 3 prostate cancer. * Normal renal glomerulus Correlation of PD-L1 expression with tumor type in 49 patients treated with anti-PD-1 18 No. patients 16 14 12 10 PD-L1(+) 8 PD-L1(-) 6 4 2 0 0 MEL Responders/total: 8/20 NSCLC 3/13 RCC 2/6 CRC 0/7 CRPC 0/3 Patients were “PD-L1+” if ≥5% of tumor cells in any tumor biopsy expressed cell surface PD-L1, using mAb 5H1 (L. Chen) and manual staining technique. 2 Mechanisms for PD-L1 up-regulation in tumors Innate Resistance MHC-pep TCR TUMOR T Cell Constitutive tumor signaling induces PD-L1 on tumor cells Oncogenic Pathway PD-L1 PD-1 Adaptive Resistance TUMOR T Cell PD-L1 expression reflects immune reaction TUMOR T Cell Stats IFN-g Focal PD-L1 expression in melanoma: geographic co-localization with TILs creates a “shield” against immune attack Tumor Lymphs PD-L1 expression in melanoma correlates with the presence of TILs and increased overall survival in patients with metastatic disease % of cases 80 60 TILs PD-L1(+) PD-L1(-) No TILs p<0.0001 40 20 % survival 100 p=0.032 0 PD-L1(+), n=57 PD-L1(-), n=93 Duration follow-up (mo) TILs are necessary but not sufficient for PD-L1 expression (Taube et al., Science Transl Med 2012) PD-L1 PD-L1 expression on tumor cells and TAMs in oropharyngeal SCCHN: association with CD8+ TILs, IFN-g and HPV+ tumors tumor p=0.002 CD68 # patients CD3 p=0.003 15 10 5 0 PD-L1+ PD-L1- HPV+ (n=20) HPV(n=7) Lyford-Pike, Pai , et al., Cancer Res 2013 PD-L1 tumor PD-L1 expression on tumor cells and TAMs in Merkel cell Ca: association with CD8+ TILs, MCV, and overall survival CD68 CD8 PD-L1+ 10 0 0 MCV+ (n=34) PD-L1p=0.01 MCV(n=8) Survival probability stroma # Tumors 20 Duration of follow-up (years) Lipson, Taube, et al., Cancer Immunol Res 2013 PD-1 pathway in virus-associated cancers: at the crossroads of cancer immunology and microbial immunology Principles of PD-1/PD-L1 mechanism-of-action first demonstrated in preclinical models of infectious disease PD-1 pathway restrains host immune responses against chronic infection Virus-associated cancers account for a large proportion of cancer deaths worldwide PD-1 blockade now in the clinic for virus-associated hepatocellular cancer, in planning for HIV Potential PD-1 pathway interactions in chronic HIV infection Increased PD-L1 expression on APCs in HIV infection PD-L1/2 PD-1 ?? CD4 T cell HIV+ APC CD4 T cell HIV+ ?? PD-1 and other coinhibitory molecules are expressed on HIV specific CD8 T cells (-) (-) (-) PD-1+ CD4 T cells might be an important latent viral reservoir CD8 T cell Dissecting mechanisms and resistance pathways: Immune infiltrates at the boundary of PD-L1+ melanoma cells PD-L1 H&E H&E IFN-g mRNA is overexpressed in PD-L1(+) vs. PD-L1(-) melanomas (Taube et al., Science Transl Med 2012) Gene expression profiling reveals inflammatory signature in PD-L1(+) tumors Gene expression profile of TILs from PD-L1(+) vs. (-) melanomas reveals functional groups of differentially expressed genes and potential bypass pathways -log10 p value PRF1 3.1x IL-10 3.3x CCL5 2.6x PD-1 7.3x TLR3 4.6x CXCL1 8.3x CD8a 2.4x LAG-3 10.7x Th1 IFN-g 11.3x IL-22R -4.4x IL-21 4.1x PD-L1 4.4x log2 fold change multiplex qRT-PCR, CD45 normalization CD8 T Checkpoint Association of lymphocyte activation gene-3 (LAG-3)+ lymphocytes with PD-L1+ melanoma cells H&E PD-L1 LAG-3 IHC tumor lymphs ISH Young, Taube et al., AACR 2013 abstr. #465 Meeker, Taube, Advanced Cell Diagnostics Synergistic anti-tumor effects of dual checkpoint blockade: anti-PD-1 and anti-LAG-3 in a murine tumor model AntiLAG-3 (0/10 TF) 2000 1500 1000 Anti-LAG-3 +Anti-PD-1 (8/10 TF) 500 50 40 30 20 0 10 Anti-PD-1 (4/10 TF) 0 Tumor Volume (mm3) Control Ab (0/10 TF) Days Post-Treatment Initiation (Shown: MC38 colon cancer) Drake, Vignali, Korman, Pardoll et al., Cancer Res 2012 Therapeutic implications for PD-1 pathway blockade in adaptive resistance model Anti-PD-1 monotherapy Strong endogenous anti-tumor immune response PD-L1 up-regulation in tumor Weak endogenous anti-tumor immune response No PD-L1 up-regulation in tumor RESPONSE 1 Inducer of anti-tumor immunity (vaccine, TKIs, “immunogenic” chemo, RT) Endogenous anti-tumor immune response PD-L1 expression in tumor 2 Anti-PD-1 RESPONSE PD-1 pathway blocking agents in clinical testing www.clinicaltrials.gov Target Molecule PD-L1 (B7-H1) Company PD-1 Amplimmune/GSK AMP-224 (PD-L2/Fc fusion protein) N/A Bristol-Myers Squibb Nivolumab/BMS-936558/ MDX-1106/ Ono-4538 (fully human IgG4 mAb) BMS-936559/MDX1105 (fully human IgG4 mAb) CureTech Pidilizumab/CT-011 (humanized IgG1 mAb) N/A Genentech N/A MPDL3280A (Fc-modified IgG1 mAb) MedImmune N/A Medi4736 (mAb) Merck Lambrolizumab/MK-3475 (humanized IgG4 mAb) N/A CTLA-4 Demonstration that B7.1/2 are CTLA-4 ligands Demonstration of potent immune regulatory role of CTLA-4 in KO mice Cloning of CTLA-4 gene 1985 Treatment of murine tumors with anti-CTLA-4 1990 Cloning of PD-1 gene PD-1 1995 First demonstration of clinical activity of anti-CTLA-4 in melanoma Anti-CTLA-4 confers survival benefit in melanoma Anti-CTLA-4 into patients 2000 Demonstration of organ-specific autoimmunity in PD-1 KO mice 2005 PD-L1 expression in murine tumors confers immune resistance & high PD-L1 expression in human tumors PD-L1/PD-L2 Identified as PD-1 ligands FDA approval for anti-CTLA-4 in melanoma 2010 2015 First demonstration of clinical activity of anti-PD-1 Anti-PD-1 into patients Predicted FDA approval of anti-PD-1 Anti-PD-1 & anti-PD-L1 Induce durable tumor responses in melanoma, kidney & lung cancer Pardoll , Nature Immunol 2012 How can the path to clinical approval be accelerated? Regulatory challenges for targeted immunotherapies: Defining appropriate endpoints for clinical efficacy Understanding unique side-effects and developing effective monitoring and management guidelines Identifying biomarkers predicting response, which may be dynamic and tissue-specific ACKNOWLEDGEMENTS Thanks to collaborating clinical trial centers. Sponsored by BMS, NIH, Barney Foundation, and Melanoma Research Alliance Sponsored by BMS, NIH, Barney Fdn., and Melanoma Research Alliance