Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
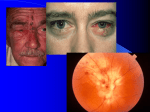
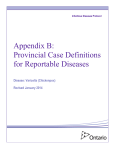
Viral Vasculopathy Maria Acena Nagel Overview I. Background II. VZV vasculopathy Clinical, morphological, and immunological features III. Cerebrovascular adventitial fibroblast studies Varicella zoster Latency cranial nerve ganglia dorsal root ganglia autonomic ganglia Varicella Latency VZV reactivation from neurons Peripheral spread to skin Central spread to cerebral arteries Productive virus infection in cerebral arteries multinucleated giant cells herpesvirions Cowdry A inclusions VZV DNA VZV antigen Gilden et al., Neurology, 1996 How common is VZV vasculopathy? VZV persists in >95% of the world population VZV Virgin et al., Cell, 2009 VZV reactivation 1 in 3 individuals will develop zoster; 2/3 will continue to shed VZV in saliva up to 12 years after zoster 30% increased risk of stroke after zoster 4.5x higher if ophthalmic-distribution zoster an unknown number will develop stroke from VZV infection of arteries without rash Kang et al., Stroke, 2009 Lin et al., Neurology, 2010 Nagel et al., J Inect Dis, 2011 VZV is present in cerebral arteries of an assymptomatic diabetic subject without zoster Nagel et al., Arch Neurol, 2012 Clinical features Stroke is most often ischemic, sometimes hemorrhagic Large and small vessels are involved Time from rash to neurological s/s ~ 4 months Time from neurological s/s to diagnosis ~ 4 months Only 2/3 of patients have rash Only 2/3 of patients have increased cells in CSF Clinical diagnosis is confirmed by detection of VZV DNA or anti-VZV IgG antibody in CSF Nagel et al., Neurology, 2007; 2008 VZV travels transaxonally to infect cerebral arteries Trigeminal Ganglia VZV Morphological/immunological features of VZV vasculopathy Cerebral artery morphology lumen intima IEL media adventitia nerve fibers normal early VZV vasculopathy chronic 1 chronic 2 Nagel et al., Neurology, 2011 normal VZV vasculopathy early chronic 1 chronic 2 Nagel et al., Neurology, 2011 Leukocytes in early case of VZV vasculopathy correlates with the thickened intima CD45 Immune response in arteries from subjects with VZV vasculopathy VZV VASCULOPATHY ADVENTITIA EARLY VZV CD45 CD3, 4, 8 CD68 CD15 MEDIA INTIMA ADVENTITIA ASSOCIATED WITH THICKENED INTIMA CD45 CD3, 4, 8 CD68 CD3, 4, 8 CD68 CD20 CHRONIC CD45 CD3, 4, 8 CD68 VZV CD45 CD3, 4, 8 CD68 VZV-infected arteries from subjects with VZV vasculopathy Thickened neointima, composed of SMA+ and SMA+/myosin+ cells not endothelial cells Internal elastic lamina is duplicated/disrupted VZV is present in adventitia in early case and media and intima in later cases supporting transmural spread of virus The media is more severely disrupted in later cases Inflammatory cells are associated with thickened intima Pathogenesis of VZV vasculopathy Trigeminal Ganglia VZV myofibroblast accumulation disruption of media Primary human cerebrovascular adventitial fibroblast studies Human cerebrovascular adventitial fibroblasts Establish quiescence Infect with VZV qPCR and ICC for migratory, proliferative, & invasive trasncripts/proteins Migration/invasion assay on transwell chambers RNA/protein analysis Functional analysis VZV infection of human cerebrovascular adventitial fibroblasts (6 dpi) fold difference (VZV/mock-infected) Fold difference (VZV/mock-infected) 1000 chemokine/cytokines adhesion proliferation/migration invasion 100 10 1 0.1 n=3 IL8 protein is elevated in VZV-infected human cerebrovascular adventitial fibroblasts IL8 concentration (pg/mL) 250 mock-infected VZV-infected ELISA 200 150 100 50 0 VZV IL8 DAPI VZV-infected cells bystander cells mock-infected cells Conditioned media from VZV-infected cerebrovascular adventitial fibroblasts attract neutrophils Neutrophil migration (%) 35 IL8 (20 ng/mL) VZV mock VZV+Acyclovir VZV+PAA 30 25 20 15 10 5 0 0 20 40 60 Time (minutes) 80 100 VZV-infected artery from a patient with early VZV vasculopathy has cells expressing IL8 in adventitia 100x 600x 100x Tonsil (+) Atherosclerosis (-) Normal (-) Abundant neutrophils are in adventitia of a VZV-infected artery from a patient with early VZV vasculopathy VZV-infected cerebrovascular adventitial fibroblasts Feasible model for studying early VZV vasculopathy IL8 is characteristic of early VZV vasculopathy Neutrophils are abundant in early VZV vasculopathy Ongoing/future studies How common is VZV vasculopathy? VZV infection in stroke patients (CDC) Screening of cerebral arteries for VZV What are other methods for diagnosis? Saliva testing for VZV PET imaging with labeled antiviral How does VZV persist and evade immune clearance? Immunosenescence Infection of immunoprivileged media Modulation of innate immune response How does thickened intima form? Source of thickened intima, mitogenic factors Extracellular ATP/purinergic signalling Consider VZV vasculopathy in your stroke differential since it is treatable with antivirals! Alexander Choe Igor Traktinskiy ACKNOWLEDGMENTS Nagel Lab Igor Traktinskiy Alexander Choe Eugene Azarkh, PhD April Rempel UCH-CVPR Laboratories Kurt Stenmark, MD Maria Frid, PhD VZV Labs Don Gilden, MD Randy Cohrs, PhD Ravi Mahalingam, PhD NIH NINDS K08 067070 NIA RO1 AG006127 NIA PO1 AG032958 Neuropathologists Bette Kleinschmidt-DeMasters, MD - UCH Tessa Hedley-Whyte, MD - Harvard Eve VanEgmond, MD - Henry Ford Hospital