Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
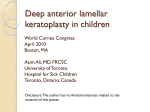
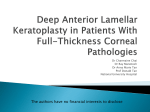
TECHNIQUE Deep anterior lamellar keratoplasty in post-laser in situ keratomileusis keratectasia Alberto Villarrubia, MD, Juan J. Pérez-Santonja, MD, PhD, Elisa Palacı́n, MD, Paz Rodrı́guez-Ausı́n P, MD, Antonio Hidalgo, MD We describe a technique using deep anterior lamellar keratoplasty (DALK) in 5 eyes that developed keratectasia after LASIK. The technique is based on surgical manipulation that allows visualization of the lamellar dissection depth using a posterior approach to reach the predescemetic space. The mirror effect, indentation effect, and folding effect were used to determine proximity to Descemet’s membrane. The same diameter donor and recipient buttons were used to correct myopia. The donor button without Descemet’s membrane was placed using 10-0 nylon sutures. No intraoperative or postoperative complications occurred. The mean best spectacle-corrected visual acuity changed from 0.16 diopter (D) G 0.05 (SD) (range 0.10 to 0.25 D) before DALK to 0.68 G 0.19 D (range 0.5 to 1.0 D) after DALK. Deep anterior lamellar keratoplasty may be a better alternative than penetrating keratoplasty for any pathology with healthy endothelium. J Cataract Refract Surg 2007; 33:773–778 Q 2007 ASCRS and ESCRS Ectatic corneal disorder (ECD) is commonly used to refer to any condition that leads to progressive corneal thinning and an increase in corneal curvature, with multiple sequelae that lead to loss of best spectaclecorrected visual acuity (BSCVA).1 Corneal disorders such as keratoconus, pellucid marginal degeneration, keratoglobus, and corneal ectasia after laser in situ keratomileusis (LASIK) fit this definition of ECD. Representing a major health burden, ECDs are the second most common indication for penetrating keratoplasty (PKP) in the United States.1 Subtractive corneal procedures such as excimer laser surgery induce weakening of the cornea postoperatively that can lead to corneal ectasia (keratectasia).1,2 A reduction in the tensile strength of the cornea is considered a major risk factor for the development of keratectasia. Iatrogenic keratectasia can occur months or years after LASIK and leads to irregular astigmatism and visual distortion.1 Currently, the definitive treatment for iatrogenic keratectasia is PKP. However, there are only a few reports of successful PKP in the treatment of iatrogenic keractectasia.2–7 One significant disadvantage of PKP is the potential for graft rejection, which can lead to significant loss of BSCVA. An alternate approach to the treatment of post-LASIK keratectasia is deep anterior lamellar keratoplasty (DALK), a partial-thickness graft that preserves the host endothelium and Descemet’s membrane (DM). Deep anterior lamellar keratoplasty has been reported for the treatment of keratoconus,8 but to our knowledge, there are no reports of DALK for the treatment of post-LASIK keratectasia. We report our technique and outcomes using DALK in 5 eyes that developed keratectasia after LASIK. Accepted for publication December 15, 2006. SURGICAL TECHNIQUE Surgery was performed by 2 of us (A.V., patients 1, 2, and 3; J.J.P.-S., patient 4). The criterion for surgical intervention with DALK was reduced BSCVA with spectacles or contact lenses. Deep anterior lamellar keratoplasty was performed using the Melles et al.9 technique. Briefly, the technique is based on surgical manipulation that allows visualization of lamellar dissection depth using a posterior approach to reach the predescemetic space.10 After air is delivered into the anterior chamber, the mirror effect, indentation effect, From the Instituto de Oftalmologı́a La Arruzafa (Villarrubia, Palacı́n, Hidalgo), Córdoba, VISSUM, Instituto Oftalmológico de Alicante (Pérez-Santonja), Alicante, and the Hospital General Universitario Gregorio Marañón (Rodrı́guez-Ausı́n P), Madrid, Spain. No author has a financial or proprietary interest in any material or method mentioned. Corresponding author: Alberto Villarrubia Cuadrado, MD, Instituto de Oftalmologı́a La Arruzafa, Avenida/Arruzafa, n 9, 14012, Córdoba. Spain. E-mail: [email protected]. Q 2007 ASCRS and ESCRS Published by Elsevier Inc. 0886-3350/07/$dsee front matter doi:10.1016/j.jcrs.2006.12.035 773 774 TECHNIQUE: DALK IN POST-LASIK KERATECTASIA Table 1. Patient data before and after deep anterior lamellar keratoplasty. Pre-LASIK Pt/Eye Sex Age (Y) Eye Spherical Equivalent (D) 1/A 2/B 3/C 4/D 5/E M M M F F 32 28 40 31 31 OD OS OS (ectasia both eyes) OD OS 8.00 6.00 5.00 12.75 14.25 Central Pachymetry (mm) Topographic Pattern BSCVA 523 Unknown Unknown 531 554 Unknown Unknown Unknown FFK FFK 0.6 1.0 0.8 0.6 0.6 BSCVA Z best spectacle-corrected visual acuity; DALK Z deep anterior lamellar keratoplasty; FFK Z forme fruste keratoconus and folding effect are used to determine the proximity of the knife to DM.10 At the predescemetic space, spatulas (2110, DORC International BV) were used to dissect this space up to the limbus, followed by delivery of an ophthalmic viscosurgical device (OVD). On maintenance of this pseudo anterior chamber, trephination was performed until the OVD emerged. Finally, scissors were used to remove residual stroma from the recipient bed and the donor button without DM was placed using 10-0 nylon sutures.9 Postoperatively, the patients were initially instructed to instill topical fluorometholone 4 times a day, with a tapered schedule over 4 months. Sutures were removed 4 months after surgery if needed. Results Four patients (5 eyes) had DALK between 2002 and 2005 for the treatment of post-LASIK keratectasia. The mean age of the 3 men and 1 woman at the time of DALK was 32.4 years between G 4.51 (SD) (range 28 to 40 years). Three eyes of 3 patients (1, 2, and 3) and both eyes of 1 patient (4) had DALK (Table 1). Before LASIK, patient 1 had a spherical refractive error; patients 2 and 3 denied the existence of astigmatism. The pre-LASIK corneal topography of eyes A, B, and C were not available as LASIK had been performed at another institution. Patient 4 had forme fruste keratoconus (FFK) in both eyes before LASIK (Table 1). Eye E was retreated for a residual refractive error 6 months after primary LASIK. Patients 1 and 2 developed unilateral keratectasia after LASIK; patients 3 and 4 developed bilateral keratectasia (Table 1). Patient 3 had DALK in the left eye due to reduced BSCVA; the right eye has retained excellent BSCVA and has not had DALK. The mean time from LASIK to the clinical diagnosis of keratectasia was 19.2 G 17.60 months (range 6 months to 4 years) and from the diagnosis to the performance of DALK, 3.3 G 1.3 years (range 2.0 to 5.5 years). The time to DALK differed because keratectasia progressed at different rates, which reduced the BSCVA at different time points. As all eyes presented with an axial length longer than 24.0 mm, the same diameter was used for the donor button and the recipient bed to correct some myopia. The mean manifest refractive spherical equivalent (MRSE) was 9.20 G 4.11 D (range 5.00 to 14.25 D) before LASIK, 12.85 G 6.22 D (range 7.00 to 21 D) before DALK, and 7.1 G 5.67 D (range 1.50 to 13.50 D) after DALK. The mean BSCVA was 0.72 G 0.20 (range 0.6 to 1.0) before LASIK, 0.16 G 0.05 (range 0.1 to 0.25) before DALK, and 0.68 G 0.19 (range 0.5 to 1.0) after DALK. Eyes C and E experienced a 1-line loss of BSCVA after DALK (Table 1); however, only 6 months of follow-up were available for eye C (Table 1). No intraoperative or postoperative complications occurred. Case Reports Eye A The corneal topography before DALK showed curvature changes consistent with ectasia (Figure 1, A); after DALK, it showed a more regular astigmatism pattern, with significantly reduced steepening (Figure 1, B). Slitlamp examination of the cornea 12 months after DALK showed folds in DM inferiorly, sparing the pupil (Figure 1, C). Histology of the recipient cornea showed integrity of Bowman’s lamina, a thick flap, and the absence of DM and endothelium (Figure 1, D). Eye E The keratometric corneal topography before LASIK showed a pattern consistent with FFK (Figure 2, A). Keratometric corneal topography after LASIK and before DALK showed a pattern consistent with inferior ectasiadsteep curvature changes inferiorly (Figure 2, B). The keratometric corneal topography after DALK showed a reduction in corneal curvature changes (Figure 2, C). Twelve months after DALK, the interface was not visible (Figure 2, D). J CATARACT REFRACT SURG - VOL 33, MAY 2007 775 TECHNIQUE: DALK IN POST-LASIK KERATECTASIA Pre-DALK Time from LASIK to Ectasia Diagnosis (Mo) Time from Ectasia Diagnosis to DALK (Y) 6 24 48 9 9 3 3 5.5 3 2 Post-DALK BSCVA Refractive Error (D) Size Recipient Donor (mm) Examination (Mo) BSCVA 0.15 0.25 0.1 0.15 0.15 6.0 6.0 130 5.0 4.0 65 7.5 3.5 130 18.0 20.0 2.0 10 8.5–8.5 8.0–8.0 8.5–8.5 8.0–8.0 8.0–8.0 12 12 6 24 18 0.6 1.0 0.7 0.6 0.5 Refractive Error (D) 4.5 4.0 0.5 11.5 11.0 3.0 170 4.0 175 2.0 130 2.0 40 5.0 180 Figure 1. Eye A (first patient). A: Orbscan corneal topography before DALK showing central and inferior ectasia. B: Orbscan corneal topography after DALK. C: The cornea 12 months after DALK showing folds in the intrapupillary part of DM. D: Histology of the recipient cornea showing integrity of Bowman’s lamina, thick flap, and absence of DM and endothelium. DISCUSSION Keratectasia after LASIK is a progressive condition that eventually leads to loss of BSCVA and reduction in visual quality.1 The first case of post-LASIK keratectasia was described in 1998.2 However, accurate estimates of the number of eyes that develop ectasia after LASIK are not available due to the lack of reliable data (Cornea Clinical Committee, ‘‘Corneal J CATARACT REFRACT SURG - VOL 33, MAY 2007 776 TECHNIQUE: DALK IN POST-LASIK KERATECTASIA Figure 2. Eye E (fourth patient). A: Corneal topography before LASIK showing a pattern similar to that of FFK. B: Corneal topography before DALK showing a pattern consistent with inferior ectasia. C: Corneal topography after DALK. D: Twelve months after DALK, the interface is not visible. Ectasia After LASIK,’’ presented at the ASCRS Symposium on Cataract, IOL and Refractive Surgery, San Francisco, California, USA, April 2003). The onset of ectasia after LASIK varies between 3 months and 5 years.11,12 In our series of 4 patients, the earliest diagnosis of ectasia was 6 months after primary LASIK and the latest was 4 years. Keratectasia has been reported to occur more frequently after retreatments,13 as seen in the left eye of patient 4 in our study. The disruption of corneal integrity by a combination of the flap cut and excess tissue removal leaving less than 250 mm of residual stromal bed depth is considered a significant precipitating factor for the development of ectasia.13 The lack of consistency in flap thickness and stromal dehydration can lead to variable residual stromal bed depth postoperatively. Collagen fibers in corneal stroma are organized from limbus to limbus perpendicularly. The tensile strength of the organized stromal tissue is reduced by the creation of the flap during LASIK. Coupled with tissue removal, this could trigger corneal irregularity due to intraocular pressure (IOP). A significant risk factor for the development of keratectasia is preoperative FFK. Histologic studies of explanted ectatic corneas that had LASIK show structural alterations in Bowman’s lamina that are highly indicative of keratoconus.2–6 From these studies, it is clear that LASIK was performed in a cornea with preexisting FFK. However, there are other reports in which Bowman’s lamina had no structural changes consistent with keratoconus,4–7 similar to the case that we present (Figure 1, D). It is likely that in this case, keratectasia developed due to a thicker flap than intended and/or a predisposing factor that is currently unknown. We are not able to determine whether eyes A, B, and C presented with FFK prior to LASIK because these patients were referred from elsewhere and pre-LASIK corneal topography was J CATARACT REFRACT SURG - VOL 33, MAY 2007 TECHNIQUE: DALK IN POST-LASIK KERATECTASIA not available. Corneal topography of eyes D and E (both eyes of the same patient) do show FFK before LASIK (Figure 2, A). A wide range of therapies are available for keratectasia, from rigid gas-permeable (RGP) contact lenses to surgical intervention such as PKP.14 Therapy is usually initiated based on the severity of the condition. We recommend an initial trial with ocular hypotensive agents (eg, timolol) as complete reversal of keratectasia has been described with this treatment.15 If this trial is not successful, we opt for optical correction with spectacles or RGP contact lenses. If optical correction does not yield optimal visual acuity, surgical treatment is warranted. The recent introduction of corneal collagen crosslinking may be a less invasive, temporary therapy for the progression of keratoconus.16 Intrastromal corneal ring segments (Intacs, Addition Technology; Ferrara, Visiontech Medical Optics) represent a surgical alternative. Intacs can correct myopic regression after LASIK as well as keratectasia after LASIK.17–21 Our experience is that Intacs are a successful treatment for central ectasia rather than inferior ectasia. In cases of inferior keratectasia, greater success has been achieved by implanting 1 inferior Intacs segment instead of 2.22 If ectasia is central, 2 Intacs segments are required.22 If Intacs are not successful, corneal transplantation (penetrating or lamellar) is the next logical option. Successful results have been reported with PKP.2–7 However, to our knowledge, there are no reports of DALK for the treatment of post-LASIK ectasia. There are reports of DALK for the treatment of keratoconus.8 The advantages of DALK over PKP for any corneal pathology with healthy endothelium have been described.23 Advantages of DALK over PKP include faster functional outcomes because sutures can be removed sooner than in PKP; there is no risk for endothelial rejection, and the survival of the transplant is longer since endothelial density declines slowly over a period of years after PKP. The main disadvantage is that DALK is a technically demanding and time-consuming procedure. Additionally, poor quality of vision may be likely due to the light scatter between the 2 interfaces. Although we agree that poor quality of vision is a possibility, in our opinion, the benefit of faster visual rehabilitation and easier postoperative management are reasons to select DALK over PKP. This is especially true in patients with keratoconus and with post-LASIK ectasia, who are generally young and socially active. The BSCVA after DALK is similar to that obtained after PKP for the treatment of keratoconus.8 If exposure of DM has been performed 777 without intraoperative complications, the BSCVA outcomes should be similar for DALK and PKP, which is what we found in this series of 5 eyes. REFERENCES 1. Binder PS, Lindstrom RL, Stulting RD, et al. Keratoconus and corneal ectasia after LASIK. J Refract Surg 2005; 21:749–752 2. Seiler T, Quurke AW. Iatrogenic keratectasia after LASIK in a case of forme fruste keratoconus. J Cataract Refract Surg 1998; 24:1007–1009 3. Amoils SP, Deist MB, Gous P, Amoils PM. Iatrogenic keratectasia after laser in situ keratomileusis for less than 4.0 to 7.0 diopters of myopia. J Cataract Refract Surg 2000; 26:967–977 4. Argento C, Cosentino MJ, Tytiun A, et al. Corneal ectasia after laser in situ keratomileusis. J Cataract Refract Surg 2001; 27:1440–1448 5. Rao SN, Epstein RJ. Early onset ectasia following laser in situ keratomileusis: case report and literature review. J Refract Surg 2002; 18:177–184 6. Spadea L, Palmieri G, Mosca L, et al. Iatrogenic keratectasia following laser in situ keratomileusis. J Refract Surg 2002; 18:475–480 7. Rumelt S, Cohen I, Skandarani P, et al. Ultrastructure of the lamellar corneal wound after laser in situ keratomileusis in human eye. J Cataract Refract Surg 2001; 27: 1323–1327 8. Watson SL, Ramsay A, Dart JKG, et al. Comparison of deep lamellar keratoplasty and penetrating keratoplasty in patients with keratoconus. Ophthalmology 2004; 111:1676–1682 9. Melles GRJ, Lander F, Rietveld FJR, et al. A new surgical technique for deep stromal, anterior lamellar keratoplasty. Br J Ophthalmol 1999; 83:327–333 10. Melles GRJ, Rietveld FJR, Beekhuis WH, Binder PS. A technique to visualize corneal incision and lamellar dissection depth during surgery. Cornea 1999; 18:80–86 11. Barraquer RI, de Toledo MC, Torres E. Distrofias y Degeneraciones Corneales; Atlas y Texto. Barcelona, Spain, Espaxs Publicaciones Médicas, 2004 12. Randleman JB, Russell B, Ward MA, et al. Risk factors and prognosis for corneal ectasia after LASIK. Ophthalmology 2003; 110:267–275 13. Binder PS. Ectasia after laser in situ keratomileusis. J Cataract Refract Surg 2003; 29:2419–2429 14. Colin J, Velou S. Current surgical options for keratoconus. J Cataract Refract Surg 2003; 29:379–386 15. Hiatt JA, Boxer Wachler BS, Grant C. Reversal of laser in situ keratomileusis-induced ectasia with intraocular pressure reduction. J Cataract Refract Surg 2005; 31:1652–1655 16. Caporossi A, Baiocchi S, Mazzotta C, et al. Parasurgical therapy for keratoconus by riboflavin-ultraviolet type A rays induced cross-linking of corneal collagen; preliminary refractive results in an Italian study. J Cataract Refract Surg 2006; 32:837–845 17. Güell JL, Velasco F, Sánchez SI, et al. Intracorneal ring segments after laser in situ keratomileusis. J Refract Surg 2004; 20:349–355 18. Barbara A, Shehadeh-Masha’our R, Garzozi HJ. Intacs after laser in situ keratomileusis and photorefractive keratectomy. J Cataract Refract Surg 2004; 30:1892–1895 J CATARACT REFRACT SURG - VOL 33, MAY 2007 778 TECHNIQUE: DALK IN POST-LASIK KERATECTASIA 19. Pokroy R, Levinger S, Hirsh A. Single INTACS segment for postlaser in situ keratomileusis keratectasia. J Cataract Refract Surg 2004; 30:1685–1695 20. Siganos CS, Kymionis GD, Astyrakakis N, Pallikaris IG. Management of corneal ectasia after laser in situ keratomileusis with INTACS. J Refract Surg 2002; 18:43–46 21. Alió JL, Salem TF, Artola A, Osman AA. Intracorneal rings to correct corneal ectasia after laser in situ keratomileusis. J Cataract Refract Surg 2002; 28:1568–1574 22. Alió JL, Artola A, Hassanein A, et al. One or 2 Intacs segments for the correction of keratoconus. J Cataract Refract Surg 2005; 31:943–953 23. Benson WH, Goosey CB, Prager TC, Goosey JP. Visual improvement as a function of time after lamellar keratoplasty for keratoconus. Am J Ophthalmol 1993; 116:207–211 J CATARACT REFRACT SURG - VOL 33, MAY 2007 First author: Alberto Villarrubia, MD