Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
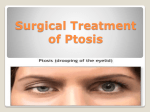
HEALTH CARE PROFESSIONALS DELIVERING EYE CARE ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ Rarely ptosis in the newborn can result from a third cranial nerve palsy or damage to the sympathetic nerves going into the orbit. A third nerve palsy may occur with birth trauma and generally presents with a complete ptosis as well as an eye that is turned down and out. The pupil is also dilated. Damage of the sympathetic nerve leads to Horner’s Syndrome (ptosis, anhidrosis, miosis, iris heterochromatia and apparent enophthalmos). Another neurogenic type of ptosis is referred to as “Jaw-wink ptosis” (or synkinetic ptosis). In this situation, when the child sucks on a bottle, thumb or chews food, the droopy lid f licks open. [Figure 2a and 2b] Essentially a ○ Neurogenic Ptosis ○ ○ The commonest cause of ptosis in the child is due to a localized dystrophy of the muscle tissue. [Figure 1] Histopathologic studies of the levator muscle have demonstrated fibrous tissue where striated muscle would be expected. The more fibrous tissue present, the poorer the levator function. The process may be unilateral or bilateral. The lid may have good function or poor function depending upon how much fibrous tissue is in the muscle. ○ Myogenic Ptosis ○ ○ ○ Aponeurotic disinsertion can occasionally occur in the child as a result of trauma from forceps or trauma through the birth canal. The lid is low but generally has excellent levator function as well as a defined lid crease. ○ ○ ○ ○ ○ ○ ○ ○ ○ Aponeurotic Ptosis ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ Figure 1 – Ptosis blocking visual axis. ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ Congenital ptosis, may be divided into Aponeurotic, Myogenic, Neurogenic, Neuromyogenic and/or Mechanical causes [Table 1]. The commonest cause of ptosis in the adult is a result of a weakening or dehiscence of the levator aponeurosis, which connects the levator muscle to the tarsal plate of the lid. Congenital ptosis on the other hand is most commonly due to a developmental problem within the muscle itself (i.e. myogenic). ○ What Causes Congenital Ptosis? ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ Ptosis (pronounced “toe-sis”) refers to a drooping of the upper eyelid. The lid may droop only slightly or it may droop enough to partially or completely cover the pupil, restricting or obscuring vision. [Figure 1] Ptosis may be inherited, may affect one or both eyelids, can be present at birth or occur later in life. Ptosis which is present at birth is called Congenital Ptosis. If the ptosis develops with age it is referred to as Acquired Ptosis. Although both congenital and acquired ptosis may significantly affect cosmesis and interfere with visual function, congenital ptosis is of particular importance as it may lead to serious problems with visual system development and maturation, proper ocular alignment as well as psychosocial development. ○ ○ ○ ○ Professor of Ophthalmology University of Ottawa Ottawa, ON, Canada ○ M.D., F.R.C.S.(C), F.A.C.S. ○ by David R. Jordan ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ Ptosis In Children ○ Issue 4 ○ Volume 6 ○ ○ ○ ○ ○ ○ ○ In A QUARTERLY REPORT FOR 1 · 3rd nerve palsy · Horner’s syndrome · Jaw-wink ptosis Neuromyogenic · myasthenia Mechanical · lid tumors Pseudo-ptosis · · · · ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ Figure 2a – Ptosis of childs left upper lid. ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ¯ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ¯ ○ ○ ○ ○ Figure 2b – Child opens her mouth or chews and ptotic eyelid flicks open. ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ microphthalmic eye, anophthalmos, phthisis bulbi hypotropia contralateral lid retraction contralateral proptosis ○ Age at time of onset should be elicited from the patient and/or the parents; old photographs may be valuable for this purpose. Di fferentiating congenital (present at bir th) from acquired is extremely important since management of the two disorders can be quite different. A neonatal medical history should include information on prematurity, trauma at ○ ○ Neurogenic ○ What Features Are Important During History Taking? ○ ○ ○ ○ ○ ○ ○ ○ ○ · localized dystrophy (most common) · other muscle diseases (myotonic dystrophy) ○ Myogenic ○ ○ · disinsertion of aponeurosis ○ ○ Aponeurotic ○ A distinction must also be made between “pseudo-ptosis” and “tr ue ptosis” i n determining the pathogenesis of abnormal eyelid position in patients with suspected congenital ptosis. Pseudo-ptosis, “an apparent drooping of the upper eyelid secondary to abnormalities involving the globe or ocular adnexa” results from ipsilateral enophthalmos (microphthalmic eye), contralateral exopthalmos, hypotropia (vertical strabismus), and contralateral eye retraction. ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ Congenital Ptosis: Classification ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ Pseudo-ptosis ○ ○ ○ ○ ○ ○ Large upper lid lesions such as capillary hemangiomas or neurofibromas may act as a weight on the lid, causing it to droop. ○ ○ Mechanical Ptosis ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ TABLE 1 ○ ○ birth, other congenital anomalies and, significant systemic illness. The clinician should inquire about any prior associated ocular abnormalities such as amblyopia, strabismus and the jaw-winking phenomenon when eating, chewing, etc. A family history of congenital ptosis is also important in making the diagnosis. ○ Myasthenia Gravis is a rare condition in children that is a result of a problem at the ner ve-muscle junc tion. The neurotransm itter (acet ylcholi ne) wh ich is released from the ner ve terminal and stimulates the muscle to contract is being blocked from activating the muscle. The key to this diagnosis is fatigue with time. That is, the lid(s) appear at a normal height in the morning but droops as the day goes on. Treatment is nonsurgical and requires medication to increase the level of acetylcholine at the neuromuscular junction. ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ Neuro-myogenic Ptosis ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ branch of the fifth cranial nerve going to the pter ygoid muscles (used during swal lowi ng, suck ing, etc.) has been misdirected during embryologic development and travels to the lid where it innervates the levator muscle. When these sucking or chewing muscles are activated the lid “f licks” open and gives the appearance of a “winking” eyelid. 2 ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ Figure 3a – Ptosis of patients right upper lid pre-operative. ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ¯ ○ ○ Children with ptosis will have a droop of one or both lids and may appear sleepy looking. They will often tilt their heads back into a chin-up position to see, or raise their eyebrows in an effort to raise their lids above the visual axis. When the lid droop is bilateral and severe, the developing infant may bump into things as a result of the droopy lids causing a visual restriction. This may also lead to a delay in development of the child. ○ ○ ○ ○ ○ ○ ○ ○ What Are The Signs And Symptoms Of Congenital Ptosis? ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ The most common surgical procedure for congenital ptosis involves an advancement of the levator aponeurosis and/or levator muscle. [Figure 3a and 3b] ○ ○ ○ How Is Congenital Ptosis Treated? The treatment of congenital ptosis is surgical in the majority (98%) of patients. Indication for surgery include visual axis occlusion by the ptotic lid, an abnormal head position, developmental delay and an unsatisfactory facial appearance. Surgery is generally performed during the pre-school years (age 3-5) although earlier intervention may be required if visual impairment (causing amblyopia) is significant. When deciding upon surgery, the surgeon must consider many factors including the extent of the patient’s ptosis, the maximum upper lid excision and the pathogenesis of the disorder. For surgical cases it is the levator function that determines what type of surgery is to be carried out. ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ Each child with ptosis requires a thorough ophthalmic exam. A visual acuity check, ocular motility assessment and refraction The levator muscle function (downgaze to upgaze) is important to determine during the exam as it will determine what type of surgery is required. ○ ○ Examination Of The Child With Ptosis: (looking for astigmatism) are important. Children should also be examined for iris heterochromia (congenital Horner’s syndrome), Jaw-winking, dilated pupil (3rd nerve) as well as looking at the lid anatomy for signs of capillary hemangioma, neurofibroma or other congenital anomalies for example the blepharophimosis syndrome (epicanthus inversus, telecanthus and phimosis). ○ ○ In addition, a number of children with ptosis also have astigmatism on the same side. If the astigmatism is not corrected, the blurred image created can also lead to amblyopia. ○ ○ ○ Ptosis can also hide a “misalignment or crossing of the eyes” which can also cause amblyopia. If the misalignment is not treated early in childhood (<6 years) the child’s vision will be permanently reduced as a result. Figure 3b – Post operative photo, equal lid heights. ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ A child’s visual system develops and matures throughout the first 6 years of life. In the first few months of life the visual system is particularly fragile. If the eyelid covers part of the visual axis, the child’s visual development can be turned off resulting in poor vision and a condition known as “amblyopia”. If the amblyopia is not corrected early, the poor vision becomes permanent and the vision will remain poor. If the amblyopia is recognized early (i.e. less than 6 years) it may be corrected with eye patching and in some cases glasses. The earlier the amblyopia is picked up, the easier it is to correct. Similarly, the longer it is left the harder it becomes to correct. Beyond 6 years the visual system is locked in and amblyopia can not be corrected (by glasses, laser, etc.). ○ ○ ○ ○ What Problems Can Occur As A Result Of Childhood Ptosis? ○ ○ ○ ○ ○ Figure 4b – Post frontalis sling surgery. ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ Bleeding and infection are possible but extremely rare. Under or over correction of the lid height can occasionally occur. If the lid height anomaly is obvious, a suture adjustment may be required in the first to two weeks. A temporary inability to fully close the eye after ptosis surgery is common and generally resolves in most over a few weeks. The eyelids do not remain “stuck open”. During this time period when the lids are not fully closing it is important to use lubricating drops and ointment to keep the cornea moist. ○ What Are The Risks Of Ptosis Surgery? ○ ○ Summary ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ Ptosis in children can be successfully treated with surgery to improve visual function as well as improve cosmetic appearance. The drooping lid can affect visual development in an infant and if the lid is blocking part of the visual axis, an ophthalmic assessment is extremely important to avoid the development of amblyopia. ○ The commonest type of ptosis in the child is due to a “muscle development problem”, the muscle simply has more fibrous and fatty tissue than normal. As a result it is weak. It does not improve with time. The only type of ptosis that might improve with time is a ptosis secondary to birth canal trauma or forceps. In these cases the lid may be bruised or swollen. ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ Figure 4a – Severe bilateral ptosis. ○ In those children with very poor levator muscle function (less than 3 mm), there is no point in advancing or resecting the levator, the lid will remain low. In these children the lid must be raised by attaching a suture, silicone rod or facial strip (autogenous or banked fascia) from the eyelid to the frontalis muscle at the level of the eyebrows. This procedure is termed a “frontalis sling”. This procedure works very well when the ptosis is bilateral. [Figure 4a and 4b] When a poor function unilateral ptosis is present a difficult question arises: should one carry out a unilateral frontalis sling, leaving one lid to be raised by the normal levator muscle while the other ptotic lid is being raised by a much different mechanism, the frontalis muscle? Or, should one carry out a bilateral frontalis sling? The best surgical approach to use in patients with severe unilater al congenital ptosis remai ns controversial. Some surgeons advocate unilateral frontalis sling procedures to avoid surger y on the anatom ically nor mal contralateral upper lid. However, patients undergoing unilateral frontalis suspension may prefer to see with the normal nonptotic eye; these patients may fail to use the frontalis muscle that opens the ptotic eye, thus negating the desired effect of surgery. Additionally, unilateral frontalis sling surgery may produce lagophthalmos and lid lag on the operated side, with cosmetically unacceptable palpebral fissure asymmetry on downgaze. Consequently, many surgeons, prefer an alternative approach: bilateral frontalis suspension with weakening of the normal levator muscle by partial excision (basically converting the normal eyelid to a poor function ptotic eyelid). This procedure usually achieves satisfactory eyelid elevation and palpebral fissure symmetry in primary position and downgaze. Bilateral frontalis suspension may also be the procedure of choice in patients with severe congenital ptosis and the jaw-winking phenomenon. In these patients, partial levator excision on the ptotic winking side, levator excision on the nor mal side, and bilateral frontalis suspension are combined to alleviate abnor mal upper lid movement with masseter and pterygoid contraction. If you have any questions regarding the topics of this newsletter, or requests for future topics of “InSight”, please contact Dr. David R. Jordan by telephone (613) 563-3800, fax (613) 563-1576 or e-mail at [email protected] · Check our Web Site for previous issues of InSight – www.drjordan.on.ca