Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
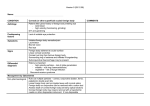
CLINICAL MANAGEMENT GUIDELINES Corneal abrasion Aetiology Loss of corneal epithelial tissue due to: sub-tarsal foreign body trauma (e.g. fingernail, twig, edge of paper, mascara brush) contact lens related trauma trichiasis (e.g. lash contact in entropion) Predisposing Contact lens wear factors Corneal dystrophy Epithelial Basement Membrane (EBM) dystrophy, in which epithelium is abnormal and easily traumatised Corneal exposure dry eye lagophthalmos facial palsy Diabetes Neurotrophic keratitis Symptoms Pain ranges from mild foreign body sensation to severe pain; may be disproportionate to objective findings absence of pain should alert to possibility of neurotrophic keratitis Blepharospasm Photophobia Lacrimation Redness History of trauma Signs Vary according to severity of trauma Lid oedema and erythema Conjunctival hyperaemia Corneal epithelial defect (stains with fluorescein) Corneal oedema beneath defect Visual loss (due to epithelial disruption and stromal oedema) Possible secondary anterior uveitis (anterior ciliary injection, cells, flare) Differential Infectious keratitis (all forms) diagnosis Recurrent corneal erosion Spontaneous epithelial breakdown in EBM Dystrophy (see Clinical Management Guideline on Recurrent Erosion Syndrome) Photokeratitis (see Clinical Management Guideline on Photokeratitis) Management by Optometrist Practitioners should recognise their limitations and where necessary seek further advice or refer the patient elsewhere Non Determine how the injury was caused. In particular rule out chemical injury pharmacological and penetrating trauma Evaluate abrasion using fluorescein size (use length of slit beam) and location depth edge quality oedema beneath abrasion confirm no corneal foreign body present If corneal foreign body present, see Clinical Management Guideline on Corneal Foreign Body Evaluate anterior chamber reaction Evert eyelids to confirm no foreign body present Corneal abrasion Version 10, Page 1 of 3 Date of search 07.12.14; Date of revision 26.03.15; Date of publication 28.05.15; Date for review 06.12.16 © College of Optometrists CLINICAL MANAGEMENT GUIDELINES Corneal abrasion If sub-tarsal foreign body present, see Clinical Management Guideline on SubTarsal Foreign Body Advise patient to return/seek further help if symptoms persist (potential for development of Recurrent Epithelial Erosion Syndrome (see CMG on Recurrent Epithelial Erosion Syndrome) Advise on suitable eye protection (GRADE*: Level of evidence=low, Strength of recommendation=strong) For large abrasions, consider therapeutic contact lens fitting (GRADE*: Level of evidence=low, Strength of recommendation=weak) Do not patch eye (GRADE*: Level of evidence=high, Strength of recommendation=strong) Pharmacological Topical anaesthetic (e.g. gutt. benoxinate 0.4%) if necessary to aid examination Systemic analgesia for first 24h (paracetamol, aspirin, or ibuprofen if no contraindications; dosage as for headache) (GRADE*: Level of evidence=low, Strength of recommendation=strong) Ocular lubricants for symptomatic relief (drops for use during the day, unmedicated ointment for use at bedtime) (GRADE*: Level of evidence=low, Strength of recommendation=strong) Also consider a topical NSAID for its analgesic and anti-inflammatory properties, e.g. gutt. diclofenac 0.1% up to four times daily for 1-3 days (GRADE*: Level of evidence=moderate, Strength of recommendation=strong) If there is a possibility of infection, prescribe a broad spectrum topical antibiotic e.g. chloramphenicol (NB risk of infection following mild trauma is low) (GRADE*: Level of evidence=low, Strength of recommendation=weak) For large abrasions or in associated iritis, consider cycloplegia to prevent pupil spasm, e.g. gutt. cyclopentolate 1% twice daily until healed) (GRADE*: Level of evidence=low, Strength of recommendation=weak) B3: management to resolution A2: if abrasion deep and/or contaminated with foreign material, or apparently infected, refer as emergency (same day) to Ophthalmologist Possible management by Ophthalmologist Assess for secondary infection Debridement if indicated Therapeutic contact lens fitting Plain X-ray or CT scan to exclude retained foreign body Evidence base *GRADE: Grading of Recommendations Assessment, Development and Evaluation (see http://gradeworkinggroup.org/toolbox/index.htm) Management Category Sources of evidence Calder LA, Balasubramanian S, Fergusson D. Topical nonsteroidal antiinflammatory drugs for corneal abrasions: meta-analysis of randomized trials. Acad Emerg Med. 2005;12(5):467-73 Meek R, Sullivan A, Favilla M, Larmour I, Guastalegname S. Is homatropine 5% effective in reducing pain associated with corneal abrasion when compared with placebo? A randomized controlled trial. Emerg Med Corneal abrasion Version 10, Page 2 of 3 Date of search 07.12.14; Date of revision 26.03.15; Date of publication 28.05.15; Date for review 06.12.16 © College of Optometrists CLINICAL MANAGEMENT GUIDELINES Corneal abrasion Australas. 2010;22(6):507-13 Turner A, Rabiu M. Patching for corneal abrasion. Cochrane Database of Systematic Reviews 2006, Issue 2. Art. No.: CD004764. DOI: 10.1002/14651858.CD004764.pub2 Wipperman JL, Dorsch JN. Evaluation and management of corneal abrasions. Am Fam Physician. 2013;87(2):114-20 LAY SUMMARY Abrasions of the cornea (the clear window of the eye) are common, being usually caused by a minor accidental injury, for example by a finger, mascara brush or contact lens, or by a speck of foreign matter under the upper eyelid. There are also medical conditions that make abrasions more likely, for example a condition, known as a dystrophy, in which the surface tissue of the cornea (the epithelium) is more delicate than usual; also when the cornea is exposed by failure of the normal blink reflex, or when its sensitivity to touch is reduced by damage to its nerves, as in diabetes or following shingles of the eye. Corneal abrasion can be very painful as the cornea is one of the most sensitive areas of the body. The clinician will assess the area involved and prescribe treatment accordingly. The damage to the surface can be seen more easily if fluorescein, an orange dye, is instilled into the eye. Antiinflammatory or antibiotic eye drops are often recommended, depending on the type and size of abrasion. Dilating eye drops, to relax the pupil, are sometimes given. There is little evidence supporting the use of these drugs. Corneal abrasions usually heal quickly and completely but if the injury is deeper, or contaminated by foreign material, or possibly infected, referral to an ophthalmologist is recommended. Corneal abrasion Version 10, Page 3 of 3 Date of search 07.12.14; Date of revision 26.03.15; Date of publication 28.05.15; Date for review 06.12.16 © College of Optometrists