Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
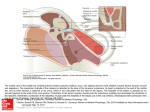
Simultaneous Management of Malleus Fixation during Stapedectomy for Otosclerosis David R Friedmann, MD, Ayaka J Iwata, MS, Anil K Lalwani, MD Department of Otolaryngology-Head and Neck Surgery, New York University School of Medicine, New York, NY. ABSTRACT DISCUSSION FIGURES Objectives / Hypothesis: Describe a rare entity of simultaneous malleus and stapes fixation, our approach to its work up and operative management. Study Design: Case Report. Methods: A 37 year old patient with presumed otosclerosis underwent left middle ear exploration for stapedectomy. Pre-operative imaging was normal. Intraoperatively, ligamental fixation of the malleus was noted in addition to stapes footplate fixation. A single stage malleostapedotomy was performed. Results: Postoperative audiogram revealed closure of the left air bone gap to within 10 dB and at 6 months, there is complete closure of the air bone gap. Conclusions: Preoperative imaging and a methodical intraoperative approach to middle ear exploration are critical to making an accurate diagnosis. Simultaneous anterior malleolar fixation stapes fixation can be addressed simultaneously by malleostapedectomy. INTRODUCTION • The finding of a simultaneously fixed malleus and stapes is extremely rare, and is reported to be present in 0.4 to 4% of otosclerosis cases (1-3). • Preoperatively, the presumed etiology of otosclerosis is isolated stapes fixation, but the definitive diagnosis is made during surgery. • Preoperative temporal bone CT scan may be particularly beneficial in cases with an unclear clinical history. • Simultaneous malleus and stapes fixation can be managed by a one-step malleostapedectomy or a two stage operation, but no systematic studies have been done to compare these two methods. Figure 1: Preoperative audiogram shows maximal conductive hearing loss on left and 35 dB air bone gap on right. Figure 3: Postoperative audiogram at six weeks demonstrates closure of the left air bone gap to within 10 dB, which has since closed completely on further follow up. Methods • Case report and review of the literature. RESULTS • We report the case of a 37 year old man who presented with a 10 year history of bilateral progressive hearing loss. • He also reported two episodes of vertigo accompanied by hearing loss, fullness, and tinnitus over the previous five years. • There was no family history of hearing loss. • Audiologic evaluation revealed bilateral conductive hearing loss with an air bone gap of 55dB on the left and 30dB on the right, with good cochlear reserve bilaterally (Figure 1). • CT of the temporal bone was obtained given the unclear clinical history. It did not reveal foci of otospongiosis, ossicular fixation, or other abnormality, and the radiology report was read as normal (Figure 2). • Upon further independent review intraoperatively, we found some suggestion of fixation in the area of the left malleus to the anterior epitympanum. • Patient underwent left middle ear exploration with planned stapedectomy for presumed otosclerosis. • Intraoperatively, fixation of both the malleus and stapes footplate was noted. • The malleus was immobile due to fixation at the anterior malleolar ligament to the anterosuperior epitympanum. • A single stage malleostapedotomy was performed with laser lysis of the bony fixation of malleus and a small fenestra stapedectomy using a 4.5mm Eclipse piston prosthesis. • There was excellent mobility of the malleus, incus, and the prosthesis within the stapedotomy. • The postoperative audiogram at six weeks revealed closure of the left air bone gap to within 10 dB (Figure 3). • On further follow-up at six months, complete air bone gap closure was achieved. A B C Figure 2: Preoperative computed tomography (CT) of the temporal bone demonstrates area of possible fixation of the malleus (A). Remainder of temporal bone CT was unremarkable (B, C). REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. Daniel R, Krieger L, Lippy W. The other ear: Findings and results in 1,800 bilateral stapedectomies. Otol Neurotol. 2001; 22:603-7. Vincent R, Sperling NM, Oates J, Jindal M. Surgical findings and long-term hearing results in 3,050 stapedotomies for primary otosclerosis: a prospective study with the otology-neurotology database. Otol Neurotol. 2006 Dec; 27(8 Suppl 2):S25-47. Lesinski SG. Causes of conductive hearing loss after stapedectomy or stapedotomy: a prospective study of 279 consecutive surgical revisions. Otol Neurotol. 2002 May; 23(3):281-8. Nandapalan V, Pollak A, Langner A, Fisch U. The anterior and superior malleal ligaments in otosclerosis: a histopathologic observation. Otol Neurotol. 2002 Nov;23(6):854-61. Oktay MF, Cureoglu S, Schachern PA, Gulbahce E, Paparella MM, Hayasi H. Histologic changes in the anterior mallear ligament and the head of the malleus in otosclerosis. Otolaryngol Head Neck Surg. 2006 Feb;134(2):232-5. Vincent R, Lopez A, Sperling NM. Malleus ankylosis: a clinical, audiometric, histologic, and surgical study of 123 cases. Am J Otol. 1999 Nov; 20(6):717-25. Huber A, Koike T, Wada H, Nandapalan V, Fisch U. Fixation of the anterior mallear ligament: diagnosis and consequences for hearing results in stapes surgery. Ann Otol Rhinol Laryngol. 2003 Apr; 112(4):348-55. Dalchow CV, Dünne AA, Sesterhenn A, Teymoortash A, Werner JA. Malleostapedotomy: the Marburg experience. Adv Otorhinolaryngol. Magliulo G, Celebrini A, Cuiuli G, Parrotto D, Re M. Malleostapedotomy in tympanosclerosis patients. J Laryngol Otol. 2007 Dec;121(12):1148-50. Epub 2007 May 25. • The likelihood of an ossicular chain abnormality is supported in the setting of a maximal conductive hearing loss and absent acoustic reflexes. • Pre-operative imaging in cases with an unclear clinical history may prevent an unnecessary middle ear exploration with all the inherent operative risks. • While in this particular case, pre-operative imaging did not help predict all of the intraoperative findings, having obtained this information assured us that other possible etiologies that might require a different surgical approach such as superior semicircular canal dehiscence (SSCD) were not present. • Independent review of the imaging raised suspicion for left malleus fixation which confirmed the intraoperative findings (Figure 2). • Specific palpation of each ossicle is critical to confirm mobility of the ossicular chain even if stapes fixation is observed. • A failure rate of 4 to 37.5% after primary stapes surgery due to malleus fixation has been reported by past studies (3, 6-8), but these include cases of simultaneous malleus-incus ankylosis with stapes fixation rather than ligamental fixation of the malleus. • Otosclerosis may be a predisposing factor to malleus fixation, related more to the duration of otosclerosis rather than its severity (4, 5). • While other groups advocate malleostapedotomy as the management of choice (8, 9) there are no systematic studies that compare the results of specific surgical techniques to address malleus fixation at the time of stapedectomy for otosclerosis. • Of great concern in such cases of ligamental fixation is the potential for re-fixation of the malleus, but we are encouraged by our success over the follow up period to date with complete closure of the air bone gap. CONCLUSION • Consideration for preoperative temporal bone CT should be given to cases with unclear clinical history to prepare for surgical exploration. • Palpation of each bone of the ossicular chain individually is essential to ensure that no other bones are fixed. • While only a single case, the audiometric follow up in this case supports the safety and efficacy of simultaneous malleostapedectomy as the primary management in cases of malleolar ligament fixation in otosclerosis.