Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
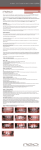
TECHNO BYTES Comparison of measurements made on digital and plaster models Margherita Santoro, DDS, MA,a Scott Galkin, DMD,b Monica Teredesai, DMD,c Olivier F. Nicolay, DDS, MS,d and Thomas J. Cangialosi, DDSe New York, NY Measuring plaster models by hand is the traditional method of assessing malocclusion. Recent technologic advances now allow the models to be digitized, measured with software tools, stored electronically, and retrieved with a computer. OrthoCAD (Cadent, Fairview, NJ) performs this service. The purpose of this study was to evaluate the reliability of the OrthoCAD system. Two independent examiners measured tooth size, overbite, and overjet on both digital and plaster models. The results were compared, and interexaminer reliability was assessed. The study sample consisted of 76 randomly selected pretreatment patients. The results showed a statistically significant difference between the 2 groups for tooth size and overbite, with the digital measurements smaller than the manual measurements. However, the magnitude of these differences ranged from 0.16 mm to 0.49 mm and can be considered clinically not relevant. No difference was found between the 2 groups in the measurement of overjet. Interexaminer reliability was consistent for both the plaster and the digital models. (Am J Orthod Dentofacial Orthop 2003;124:101-5) C omputer technology is expanding to include more areas in various scientific fields, and orthodontics is no exception. Orthodontists use computers for record keeping, practice management, patient education, communication with colleagues, restorations fabrication, and many other tasks. Computers have become a necessity rather than an option. The introduction of digital models offers the orthodontist an alternative to the plaster study models routinely used. Plaster study models are a standard component of orthodontic records, and they are fundamental to diagnosis and treatment planning, case presentations, evaluation of treatment progress and results, and record keeping. Tooth size, crowding or spacing, overjet, overbite, and Bolton analysis are typically measured by hand on plaster models. Several other methods of measuring have been proposed over the years.1-7 Schirmer and Wiltshire1 and Champagne2 compared measurement From the Division of Orthodontics, Columbia University, School of Dental and Oral Surgery, New York, NY. a Assistant professor of clinical orthodontics. b Former postgraduate resident, now in private practice, NJ. c Former postgraduate resident, now in private practice, Conn. d Associate professor of clinical orthodontics. e Professor and chairman. None of the authors has a financial interest in OrthoCAD or digital model companies. Reprint requests to: Margherita Santoro, DDS, MA, Division of Orthodontics, Columbia University, School of Dental and Oral Surgery, 635W 168th Street, P&S Box 20, New York, NY 10032; e-mail, [email protected]. Submitted, April 2002; revised and accepted, August 2002. Copyright © 2003 by the American Association of Orthodontists. 0889-5406/2003/$30.00 ⫹ 0 doi:10.1016/S0889-5406(03)00152-5 made manually on casts with those made on digitized casts obtained from a photocopier. They concluded that, although photocopies are easy to handle, manually measuring teeth with a calibrated gauge produces the most “accurate, reliable, and reproducible” measurements. The photocopier method, furthermore, still requires a traditional plaster model, and only provides a 2-dimensional image of a 3-dimensional object. Bhatia and Harrison3 studied the performance of the “travelling microscope,” an apparatus modified to measure dental casts, and concluded that the method was more precise than some alternatives. Martensson and Ryden4 investigated a holographic system for measuring dental casts. The method was shown to be more precise than previous methods, and the authors believed that it would also save storage space. However, although microscope and holographic systems had some advantages, they did not prove to be practical in clinical practice, and they never became popular. OrthoCAD (Cadent, Fairview, NJ) is a patented computer model system that creates digital images of dental casts (Fig 1). To obtain the digital images, the orthodontist sends alginate impressions and a wax bite to the OrthoCAD laboratory. The impressions are scanned, converted into digital images that are stored on the company’s server, and made available for downloading by the account holder. OrthoCAD provides software the orthodontist can use to make routine measurements, such as tooth size, overjet, overbite, and Bolton analysis, on the digital images. 101 102 Santoro et al American Journal of Orthodontics and Dentofacial Orthopedics July 2003 The study sample to compare plaster and digital models was selected randomly from the patient records at the Columbia University Orthodontic Clinic. Two sets of alginate impressions were made, plaster models were poured the same day, and 1 set was shipped immediately to OrthoCAD via overnight courier. The following selection criteria were used: ● ● ● ● Fig 1. Gallery 3-dimensional model images in OrthoCAD. ● ● ● OrthoCAD offers many advantages, including elimination of model breakage and storage problems, instant retrieval of models, ease of communication with patients and colleagues, and model access from many locations. It enables the orthodontist to e-mail images if desired and is a convenient presentation tool. Disadvantages include lack of tactile input for the orthodontist and time needed to learn how to use the system. As with any new method, accuracy must be assessed by comparison with the existing gold standard, in this case, measurements made manually on plaster casts. The purpose of this study was to compare the accuracy of measurements made by the OrthoCAD system on digital models with measurements made by hand on traditional plaster models. Because 2 separate alginate impressions were needed, 1 for plaster models and 1 for OrthoCAD, we also compared 2 consecutive alginate impressions made during the patient’s first visit, to determine whether any major bias could be detected. MATERIAL AND METHODS The sample to compare plaster models from consecutive alginate impressions consisted of 20 randomly selected subjects, each with all permanent teeth from first molar to first molar erupted, no missing teeth from first molar to first molar, and no existing orthodontic appliances. Two consecutive alginate impressions were taken on each subject and poured immediately in plaster. The bite was recorded using a wax wafer. A single examiner () measured tooth width, overbite, and overjet on both casts. The results were then statistically evaluated. Plaster and digital models made from alginate impressions taken consecutively at the same visit No appliances pretreatment Permanent dentition erupted from first molar to first molar No missing teeth from first molar to first molar Stable centric occlusion with at least 3 occlusal contacts No voids or blebs in the plaster or digital models No fractures on the teeth on the plaster models An initial sample of 100 patients was randomly selected. After the above criteria were applied, the sample size was reduced to 76 patients. Two examiners, working independently, recorded tooth size, overbite, and overjet on the plaster and digital models The sizes of the mandibular and maxillary teeth from first molar to first molar were measured, and the maximum mesiodistal width was recorded for each tooth. Overbite was measured as the amount of vertical overlap of the mandibular incisor in millimeters. This maximum overbite involving a maxillary central incisor was recorded. Overjet was measured in millimeters from the labial surface of the mandibular incisor to the labial surface of the maxillary incisor. In case of different labial inclination of the maxillary incisors, the maximum overjet was recorded. Tooth size was measured on the plaster model with an orthodontic-style Boley gauge (Orthopli, Philadelphia, Pa), to the nearest 0.1 mm. Overjet and overbite were measured with a graduated, calibrated periodontal probe, to the nearest 0.5 mm. Tooth size was measured on the digital models with the analysis tools provided by OrthoCAD, to the nearest 0.1 mm (Fig 2). The posterior teeth were measured from the occlusal view and the anterior teeth from the facial view. However, in case of rotated or malpositioned anterior teeth, the images were rotated on-screen, and the measurements were made from the occlusal view to provide better visibility. For ease and accuracy of measurements, the images were enlarged on-screen 2 or 3 times using the built-in magnifying tool. Overjet and overbite were also measured using the analysis tools. Two windows appear during this process (Fig 3). The right window has a cross-section plane Santoro et al 103 American Journal of Orthodontics and Dentofacial Orthopedics Volume 124, Number 1 Table. Repeated-measures analysis of variance between plaster and digital models P values and mean differences Variable Fig 2. Tooth size measurement tools (mesiodistal diameters) in OrthoCAD. Mand R first molar Mand R second premolar Mand R first premolar Mand R canine Mand R lateral incisor Mand R central incisor Mand L central incisor Mand L lateral incisor Mand L canine Mand L first premolar Mand L second premolar Mand L first molar Max L first molar Max L second premolar Max L first premolar Max L canine Max L later incisor Max L central incisor Max R central incisor Max R lateral incisor Max R canine Max R first premolar Max R second premolar Max R first molar Overbite Overjet P Mean difference ⬍.0001* .0003* ⬍.0001* ⬍.0001* ⬍.0001* ⬍.0001* ⬍.0001* ⬍.0001* ⬍.0001* ⬍.0001* ⬍.0001* ⬍.0001* .0012* ⬍.0001* ⬍.0001* ⬍.0001* ⬍.0001* .0009* .0002* ⬍.0001* ⬍.0001* ⬍.0001* .0001* .028* .0124* .9771 ⫺0.3053 ⫺0.2138 ⫺0.3066 ⫺0.2888 ⫺0.3592 ⫺0.2605 ⫺0.2816 ⫺0.3842 ⫺0.2447 ⫺0.3250 ⫺0.2862 ⫺0.3605 ⫺0.1632 ⫺0.2375 ⫺0.2836 ⫺0.2375 ⫺0.2763 ⫺0.2395 ⫺0.2605 ⫺0.3164 ⫺0.2224 ⫺0.2816 ⫺0.2191 ⫺0.2151 ⫺0.4901 ⫺0.00987 Mand, mandibular; Max, maxillary; R, right; L, left. *Significant at P ⬍ .05. RESULTS Fig 3. Right, selection of section plane for overbite and overjet measurements. Models can be rotated, which facilitates cross-sectioning at point of maximum overjet. Left, resulting cross-section. Overjet and overbite measurements. tool, which can be dragged to the location at which the overjet or overbite is to be measured. The maximum overjet and overbite were determined by selecting the most accurate cross-sectioning plane on the image in the right window, while actual measurements were made in the left window, where the resulting crosssection is shown. Once again, the images were enlarged to facilitate ease and accuracy of measurement. OrthoCAD measures overjet and overbite to the nearest 0.1 mm, and these measurements were rounded to the nearest 0.5 mm. Student t tests based on equality of variances revealed no significant difference between any of the measurements made on the plaster models made from consecutive alginate impressions (P values ranged between .83 and 1.00). The 2 sets of measurements made by the 2 independent examiners on the plaster and digital models were found to be significantly correlated, both for the plaster and digital models, via Pearson correlation coefficient (P ⬍ .0001), indicating good interexaminer reliability for both methods. This finding allowed the whole set of measurements to be treated as the product of the work of a single examiner. A repeated-measures analysis of variance (ANOVA) was then performed (Table). There was a statistically significant difference (significance set at P ⬍ .05) between tooth width measurements made by the 2 methods, with all the digital model measurement smaller than the corresponding plaster model measurements. The greatest mean difference 104 Santoro et al was found for the mandibular left lateral incisor (0.38 mm). ANOVA showed a statistically significant difference in overbite measurement between the plaster and digital models (P ⫽ .0124). All digital measurements were smaller than the manual measurements, with the mean difference being 0.49 mm. ANOVA showed no statistically significant difference between the overjet measurements by the 2 methods (P ⫽ .98). The mean difference was 0.098 mm. DISCUSSION The plaster and digital model groups showed differences in measurements of tooth width for each of the teeth measured. The mean differences were statistically significant but fell within a small range (0.16-0.38 mm). The digital measurements were smaller than the manual measurements. This finding cannot be attributed to differences between alginate impressions. The comparison between the measurements made on plaster casts from the 2 consecutive sets of alginate impressions showed no significant difference. Alginate shrinkage during transportation to OrthoCAD location and different pouring times therefore remained the most likely explanations for the differences. Another possible cause of different tooth size measurement is the intrinsic difference between the 2 methods. OrthoCAD provides a 3-dimensional visual pointing to interproximal contacts on an enlarged image (Fig 2) and digital tools to measure diameters and distances along selected planes. Depending on the orthodontist’s training, abilities, and preferences, measuring on a computer screen can be more or less accurate than the traditional gauge-on-cast method. There was also a statistically significant difference in overbite measurements between the 2 groups, with the digital measurements smaller than the manual ones. The difference could be attributed to the digital tooth sizes being consistently smaller than the plaster measurements. A smaller overbite, in pure terms of millimeters, must therefore be expected if the teeth are smaller. However, overbite expressed in terms of percentage will not be affected by measurements in millimeters. The magnitude of the difference (0.49 mm on average), even if slightly larger than the difference detected in tooth measurements, does not appear to be clinically significant. In fact, earlier studies have shown that the measurement error itself in the repeated single operator clinical measurements of plaster casts averages 0.2 mm.8 Other factors could have introduced some inconsistency in overbite measurements, eg, an incorrect probe angulation during the traditional model manipulation or rounding the digital measurements to American Journal of Orthodontics and Dentofacial Orthopedics July 2003 the nearest 0.5 mm. Even a different vertical plane used to measure overbite in the 2 methods could have contributed, because the plane is randomly selected in the traditional manual measurements. On the other hand, if the factors mentioned above were actually responsible for measurement inconsistency, we should expect the same discrepancy to apply to the evaluation of overjet. However, no significant difference in overjet was found in this study between the 2 groups. The finding suggests that the difference in overbite measurement could be simply and safely attributed to the smaller tooth sizes in the digital models. As stressed before, as long as the smaller tooth size is generalized and uniform, it is not a threat to the diagnostic capability of the digital method, because it does not affect proportional measurements (such as Bolton analysis and overbite expressed as a percentage). CONCLUSIONS 1. Tooth width and overbite measurements made on plaster and digital models showed statistically significant differences; the magnitude of the differences does not appear to be clinically relevant. 2. No significant difference was found in the measurement of overjet between the 2 samples. 3. Digital models seem to be a clinically acceptable alternative to stone casts for the routine measurements used in orthodontic practice. Further studies are needed to test the accuracy of OrthoCAD in calculating Bolton ratio. The time needed to measure digital models should also be evaluated and compared with the time needed to measure plaster models. There is a definite learning curve involved with the use of OrthoCAD. Familiarity with the system, as with any new method, can substantially improve measurement accuracy and reduce the time needed to complete the measurements. REFERENCES 1. Schirmer UR, Wiltshire WA. Manual and computer-aided space analysis: a comparative study. Am J Orthod Dentofacial Orthop 1997;112:676-80. 2. Champagne M. Reliability of measurements from photocopies of study models. J Clin Orthod 1992;10:648-50. 3. Bhatia SN, Harrison VE. Operational performance of the travelling microscope in the measurement of dental casts. Br J Orthod 1987;14:147-53. 4. Martensson B, Ryden H. The holodent system, a new technique for measurement and storage of dental casts. Am J Orthod Dentofacial Orthop 1992;102:113-9. 5. Halazonetis DJ. Acquisition of 3-dimensional shapes from images. Am J Orthod Dentofacial Orthop 2001;119:556-60. 6. Ramsay DS, Soma M, Sarason IG. Enhancing patient adherence: the role of technology and its application to orthodontics. In: American Journal of Orthodontics and Dentofacial Orthopedics Volume 124, Number 1 McNamara JA Jr, Trotman CA, editors. Creating the compliant patient. Craniofacial growth series, volume 33. Ann Arbor: Center for Human Growth and Development; University of Michigan; 1997. p. 141-65. 7. Mok K, Cooke M. Space analysis: a comparison between sonic Santoro et al 105 digitization (DigiGraphTM Workstation) and the digital caliper. Eur J Orthod 1998;20:653-61. 8. Santoro M, Ayoub ME, Pardi V, Cangialosi TJ. Mesiodistal crown dimensions and tooth size discrepancy of the permanent dentition of Dominican Americans. Angle Orthod 2000;70:303-7.