Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
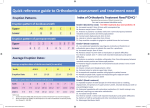
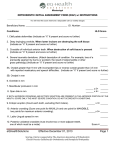
School of Dentistry ORTHODONTICS LECTURE 14 SELECTION OF ORTHODONTIC CASES Sources of difficulty Patient factors - Orthodontic considerations - - Co-operation, attendance, oral hygiene Skeletal factors Soft tissue factors Tooth malpositions - Four important relationships Four types of swallow Planning Treatment Decide on objectives Plan final tooth positions (Use models if necessary – Kesling set-up) Assess space requirements - MDA, Space analysis – measure displaced contact in each quadrant List stages of treatment. Define objectives for each stage GDPs are paid by results on the basis of start and finish models. PAR scoring is beginning to be introduced by the DPB and in the future it is possible that dentists will be paid for an “Improved” or “Greatly improved” outcome but not otherwise. It is therefore important that GDPs select cases carefully and treat only those that will give a results within a reasonable time using relatively simple appliances. If removable appliances are to be used a maximum of three is a good yardstick. The best measure of what to treat is the orthodontic experience of the individual. If a GDP is uncertain as to the best orthodontic treatment plan, the patient should be referred for advice to a Consultant Orthodontist. The alternative will be to refer to a Specialist Orthodontic Practitioner but this will result in treatment rather than advice. Read the development of the PAR Index. Richmond et al., 1992 EJO 14, 125-139. Before referral the GDP should tell the patient and parents: The reason for referral That the first hospital visit is for advice Treatment may or may not be offered. That there will be a waiting list for treatment 1 C:\lec\selection of orthocases Patients who are referred should: Be regular attenders at the practice of the referring dentist Have good OH - Plaque score below 10%. Be aware of the personal commitment needed Have a malocclusion severe enough to warrant treatment. (IOTN Grades 4.) Patients must appreciate that referral is for advice in the first instance, treatment may or may not be offered. Content of the referral letter: Outline of problem Past attendance record Level of patient/parental concern Previous orthodontic treatment Relevant medical and dental history (including caries) Confirmation that likely treatment has been discussed Signature of dentist Patients normally accepted for treatment: IOTN Grades 4 and 5 (Learn the IOTN system.) Facial clefts Adults requiring orthognathic treatment Interdisciplinary cases Transfers from other hospitals Suitable for GDP with undergraduate training only: Tooth behind bite Unilateral cross bite Class II(I) - extract upper fours only Class I - extract all fours + space maintainers Suitable for GDP with further training: Class I with anterior crowding Class II(I) Class II(I) - extract all fours headgear for molar correction lower lingual arch/fixed appliance buccal segment retraction with or without second molar extraction Specialist only: Severe skeletal anomaly: O/J > 6mm or < Edge to edge Traumatic overbite or Symmetrical anterior open bite Cases with mild or severe crowding Atypical extraction cases Missing teeth Surgery Adults 2 C:\lec\selection of orthocases All IMPORTANT GENERAL RULES IF REFERRAL IS CONTEMPLATED DO NOT: Extract teeth - primary or permanent Fit an appliance Refer early to beat the waiting list NEVER: Extract lower premolars in a Class II division 2 Extract upper premolars in a Class III before crossbite correction 3 C:\lec\selection of orthocases THE DENTAL HEALTH COMPONENT OF THE INDEXOF ORTHODONTIC TREATMENT NEED (IOTN) Grade 5 (very great) 5a Increased overjet greater than 9mm. 5h Extensive hypondontia with restorative implications (more than 1 tooth missing in any quadrant) requiring prerestorative orthodontics. 5i Impeded eruption of teeth (with the exception of third molars) due to crowding, displacement, the presence of supernumerary teeth, retained deciduous teeth and any pathological cause. 5m Reverse overjet greater than 3.5mm with reported masticatory and speech difficulties. 5p Defects of cleft lip and palate. 5s Submerged deciduous teeth. Grade 4 (great) 4a Increased overjet greater than 6mm, but less than or equal to 9mm. 4b Reverse overjet greater than 3.5mm with no maticatory or speech difficulties. 4c Anterior or posterior cross-bites with greater than 2mm discrepancy between retruded contact position and intercuspal position. 4d Severe displacements of teeth greater than 4mm. 4e Extreme lateral or anterior open bites greater than 4mm. 4f Increased and complete overbite with gingival or palatal trauma. 4h Less extensive hypodontia requiring prerestorative orthodontics or orthodontic space closure to obviate the need for a prosthesis. 4l Posterior lingual cross-bite with not functional occlusal contact in one or both buccal segments. 4m Reverse overjet greater than 1mm, but less than 3.5mm with recorded masticatory and speech difficulties. 4t Partially erupted teeth, tipped and impacted against adjacent teeth. Grade 3 (moderate) 3a Increased overjet greater than 3.5mm, but less than or equal to 6mm with incompetent lips. 3b Reverse overjet greater than 1mm, but less than or equal to 3.5mm. 3c Anterior or posterior cross-bites with greater than 1mm but less than or equal to 2mm discrepancy between retruded contact position and intercuspal position. 3d Displacement of teeth greater than 2mm, but less than or equal to 4mm. 3e Lateral or anterior open bite greater than 2mm, but less than or equal to 4mm. 3f Increased and complete overbite without gingival or palatal trauma. Grade 2 (little) 2a Increased overjet greater than 3.5mm, but less than or equal to 6mm with competent lips. 2b Reverse overjet greater than 0mm, but less than or equal to 1mm. 2c Anterior or posterior cross-bite with less than or equal to 1mm discrepancy between retruded contact position and intercuspal position. 2d Displacement of teeth greater than 1mm, but less than or equal to 2mm. 2e Anterior or posterior open bite greater than 1mm, but less than or equal to 2mm. 2f Increased overbite greater than or equal to 3.5mm without gingival contact. 2g Pre-normal or post-normal occlusion with no other anomalies. Includes up to half a unit discrepancy. Grade 1 (none) 1 Extremely minor malocclusions including displacements less than 1mm. 4 C:\lec\selection of orthocases