Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
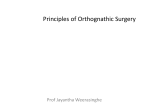
Journal of Dental Sciences (2014) 9, 272e276 Available online at www.sciencedirect.com journal homepage: www.e-jds.com ORIGINAL ARTICLE Influence of bone-cut position in intraoral vertical ramus osteotomy on skeletal stability after mandibular setback Chun-Ming Chen a, Steven Lai a, Kun-Rong Hsu b, Shiu-Shiung Lin c* a Department of Oral and Maxillofacial Surgery, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan b Department of Family Dentistry, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan c Orthodontic Department, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University, College of Medicine, Kaohsiung, Taiwan Received 23 June 2012; Final revision received 9 August 2012 Available online 27 July 2013 KEYWORDS bone-cut position; intraoral vertical ramus osteotomy; long-term stability; mandibular prognathism; sagittal split ramus osteotomy Abstract Background/purpose: Postoperative skeletal stability is associated with osteotomy design of orthognathic surgery. The purpose of this study was to investigate osteotomy siterelated factors of intraoral vertical ramus osteotomy (IVRO) related to skeletal relapse in a 2-year postoperative follow-up. Materials and methods: Twenty-seven patients with mandibular prognathism underwent surgical mandibular setback with IVRO. Cephalometric radiographs of the patients were collected after completing preoperative orthodontic treatment (T1), at the stage immediately after surgery (T2), and in the 2-year postoperative follow-up (T3). Pir was located at the posterior most and inferior most ramus point. Io was the inferior most osteotomy point of the mandible. Relapse was defined as forward movement of menton (Me) in the 2-year follow-up. Hierarchical modeling analyses were used to assess changes in the variables, including the amount of postoperative relapse (MeT32), the quantity of surgical setback (MeT21), the available setback horizontal distance (PireIo), and the available setback ratio (MeT21/PireIo). Results: The mean setback of Me was 12.6 mm, and the mean relapse was 0.9 mm (7.1% Z 0.9/ 12.6). In the 1-by-1 and 1-by-2 models, there were no significant differences between the relapse and other variables. However, we found a significant difference in the 1-by-3 model. The MeT21 and MeT21/PireIo were significant factors in postoperative relapse. * Corresponding author. Orthodontic Department, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University, College of Medicine, Number 123, Da-Pi Road, Niaosong District, Kaohsiung City 83301, Taiwan. E-mail address: [email protected] (S.-S. Lin). 1991-7902/$36 Copyright ª 2013, Association for Dental Sciences of the Republic of China. Published by Elsevier Taiwan LLC. All rights reserved. http://dx.doi.org/10.1016/j.jds.2013.06.002 Bone-cut position in IVRO 273 Conclusion: We found that multiple factors contributed to postoperative relapse of IVRO. Our study also confirmed the 2-year stability of IVRO in treating mandibular prognathism. Copyright ª 2013, Association for Dental Sciences of the Republic of China. Published by Elsevier Taiwan LLC. All rights reserved. Introduction In recent years, many operations were designed to address mandibular prognathism.1,2 Early evolution of orthognathic surgical procedures, such as subcondylar osteotomy, ramus osteotomy, and mandibular body osteotomy or step osteotomy, were routinely used to address mandibular prognathism. Subcondylar osteotomy and horizontal osteotomy of the ramus resulted in significant postoperative relapse due to the deficiency in bone-adjoining sphere. Disadvantages of mandibular body osteotomy are potential damage to the inferior alveolar nerve and forfeiture of bilateral bony segments in molar areas. In addition, divergences in the cross-distance between the bilateral second molars and second premolars are inordinate. Therefore, mandibular body osteotomy is now rarely used to handle mandibular prognathism. The blood supply to the mandible is one of the main problems during surgery. There has been concern regarding the safety of complex mandibular osteotomies because the inferior alveolar artery plays a predominant role. The work of Bell and Levy showed that blood flow through the mandibular periosteum tended to maintain a sufficient blood supply to the teeth in a mobile segment.3 This even held true in cases where the labial periosteum was degloved. This phenomenon is well evidenced by the rapidly increasing applications of orthognathic surgery. Over the years, many amendments have been applied to ameliorate postoperative stability, such as sagittal split ramus osteotomy (SSRO) and intraoral vertical ramus osteotomy (IVRO). The most crucial advantage of IVRO compared with SSRO is its much lower relative incidence of trauma to the inferior alveolar nerve.4,5 Hence, we prefer using IVRO to correct mandibular prognathism. Our department formulated a modified IVRO procedure.6 Therefore, the current research was to analyze the relationship between postoperative relapse and the osteotomy length achieved by the modified IVRO, as appraised by consecutive cephalograms in the 2-year follow-up. Materials and methods Twenty-seven patients with mandibular prognathism (22 females and 5 males) were treated with the modified IVRO procedure to correct their mandibular prognathism. Their mean age was 20.4 years (range: 17e27 years). All operations were carried out at the Department of Oral and Maxillofacial Surgery, Kaohsiung Medical University Hospital, from January 1991 to December 1998. The selection criteria for patients in this study satisfied the following standards: (1) all patients had skeletal Class III developmental malformations of mandibular prognathism with natural dentition; (2) patients with craniofacial anomalies were excluded from the analysis; (3) neither injuries nor acknowledged syndromes were etiologic factors; (4) none of the patients was in active development stage at the time of operation; (5) all patients accepted preoperative and postoperative orthodontic treatment; (6) all patients were surgically treated with modified IVRO technique by a single surgeon; and (7) an acrylic interocclusal splint and maxillomandibular fixation were used for 6 weeks postoperatively. Cephalograms were collected and appraised at the following three intervals: preoperatively after completion of presurgical orthodontic movement (T1), immediately postoperatively (T2), and at 2 years postoperatively (T3). The following items were examined: sella (S), nasion (N), the posterior most and inferior most ramus point (Pir), the inferior most osteotomy point (Io), and menton (Me). Because of the magnification differences between the left and right sides of the mandible, intermediate outlines of bilateral projected images of mandibular contour were traced and identified. In our IVRO method, the lower portion of proximal segment was excised. The Io landmark on T2 cephalometric tracing was located and transferred onto T1 cephalogram by superimposing it between T1 and T2 cephalometric tracings. The Pir landmark was identified on T1 cephalogram as the intersection between the lower half portion of ramus contour and the longest projected line perpendicular from the vertical reference line described below. For analysis, an xey coordinate axis was fabricated. The frame of reference was established with its source at nasion, and x axis was aligned at an angle of 7 upward to the source line (NeS) as the horizontal axis (Fig. 1). The vertical reference line (i.e., y axis) was aligned perpendicular to this line through sella. Cephalometric tracings of the preoperative stage (T1), changes immediately after surgery (T21), and at the 2-year postoperative stage (T32) were superimposed to assess differences. Changes in positions of the landmarks were compared with reference lines. Relapse was specified as an advancing movement of Me during the 2-year follow-up period. All alterations of each measurement were examined by a paired t test. The PireIo (the available setback horizontal distance at T1) was measured between Pir and Io along the y axis. The available setback ratio was defined as MeT21/PireIo. Hierarchical modeling analyses were used to survey differences in variables (MeT32, MeT21, PireIo, and MeT21/PireIo) and investigate factors responsible for postoperative stability. Hierarchical modeling was composed of seven models at three levels (1-by-1, 1-by-2, and 1-by-3). Differences at a level of P 0.05 were considered significant. 274 C.-M. Chen et al Table 1 (n Z 27). Summary of variable changes in patients Variable (mm) MeT21 (horizontal) MeT32 (horizontal) MeT21 (vertical) MeT32 (vertical) PireIo MeT21/PireIo Figure 1 Landmarks, references lines, and linear measurements applied in this study. The x axis was constructed by drawing a line through nasion 7 upward from the SeN line. The y axis was constructed by drawing a line through sella (S) perpendicular to the x axis. Me (menton) Z the inferior most point on the mandibular symphysis; Io Z the inferior most osteotomy point along the mandibular border; Pir Z the posterior most and inferior most point of the ramus. The error of the method in this study was assessed by replicating standardized tracings of all cephalograms several months after the first tracing. This was to assess the intraexaminer error. The error study determined the extent to which a single rater obtained the same result using the same instrument to measure the objects. Therefore, the intraexaminer error was studied in terms of landmark identification on cephalograms during tracing. Whenever the disparity between two values of any point or angle was >0.5 mm or >1 , respectively, the point or angle was noted and measured again. Other registrations were compared with the third one. The outlier was not included in the data. In addition, the mean value was determined by the two approximate values. Therefore, our outcomes and variables were considered to be reliable. Results The changes in Me at three stages (T1, T2, and T3) are shown in Table 1. The mean changes in Me were 12.6 mm backward and 0.8 mm downward. In the 2-year follow-up, the relapse rate of Me was 0.9 mm on average, and this amount represented 7.1% of the total range of the mean setback. In the Mean 12.6 0.9 0.8 0.6 14.7 0.9 Standard deviation 3.30 2.99 1.73 1.64 3.81 0.29 vertical direction, Me was 0.6 mm higher in 2 years postoperatively. The horizontal distance of PireIo was 14.7 mm. The available setback ratio (MeT21/PireIo) was 0.9. Results of hierarchical modeling analyses are demonstrated in Table 2. The P values of individual 1-by-1 models were 0.4315 (MeT21), 0.6984 (PireIo), and 0.77 (MeT21/ PireIo). The P values of 1-by-2 models were still not significant (Table 2). In the 1-by-3 model, however, P values of MeT21 and MeT21/PireIo revealed significant differences. Because of the high correlation in three independent variables, we subsequently checked the collinearity with Jump 7 software (SAS Institute, Cary, NC, USA). Collinearity is a statistical phenomenon in which an independent variable is a linear combination of other independent variables. However, we found that the largest condition index (42.88) was >30. We then used the centered scores to avoid collinearity, which would tend to involve the interaction. Finally, the largest condition index (7.06) was <10 and the outcomes were the same in the 1-by-3 model. This confirmed that MeT21 and MeT21/PireIo were significant factors responsible for postoperative stability. Discussion A research into the impact of surgery on the vascular supply has greatly benefited osteotomy designs of the mandibular Table 2 MeT32 in the hierarchical model test. Variable (model level) 95% Confidence level P Model 1: MeT21 Model 2: PireIo Model 3: MeT21/PireIo Model 4 MeT21 PireIo Model 5 PireIo MeT21/PireIo Model 6 MeT21 MeT21/PireIo Model 7 MeT21 PireIo MeT21/PireIo ( 0.23, 0.51) ( 0.26, 0.38) ( 4.92, 3.68) 0.4315 0.6984 0.77 ( 0.26, 0.53) ( 0.32, 0.37) 0.4929 0.8856 ( 0.34, 0.44) ( 5.47, 4.98) 0.7896 0.9234 ( 0.19, 0.71) ( 7.50, 2.90) 0.2518 0.3706 (0.13, 2.16) ( 1.70, 0.03) ( 27.39, 0.93) 0.0286 * 0.0578 0.0371 * *P < 0.05. Bone-cut position in IVRO ramus. Surgeons traditionally believed that the inferior alveolar artery played a key role in nourishing the mandible. However, Bell and Schendel showed that blood supply from the surrounding soft tissues was sufficient.7 The blood supply tended to be maintained when the inferior alveolar artery was obstructed. In 1957, Trauner and Obwegeser8 initially described the procedure of SSRO, and it was successively adjusted by Bell and Schendel,7 Dal Pont,9 and Epker.10 Furthermore, Moose identified the intraoral median approach to a subcondylar osteotomy in 1964,11 and in 1968, Winstanley described the intraoral lateral approach to a subcondylar osteotomy.12 Later on, Hall and McKenna further elaborated the method of IVRO.13 It is widely admitted that a certain level of skeletal alteration invariably occurs after treating mandibular prognathism. Numerous studies reported an acceptable postsurgical stability of both SSRO and IVRO techniques.4,14e16 Nevertheless, the postoperative skeletal stability is a matter of debate even among the most seasoned surgeons. The issue of major concern in orthognathic surgery is the long-term skeletal stability. In previous studies, it was found that the mean amount of surgical setback was approximately 4.87e8.4 mm for SSRO,14,15,17e19 and approximately 5.3e8.4 mm for IVRO.14,15,20 According to our research,21 the average amount of Me setback was 12.7 mm, which is greater than those in the previous reports. Compared with the amount of setback, the range of relapse potency was from 7.1% (0.6/8.4 mm) to 51.4% (2.87/5.58 mm) for SRRO, and 11.7% (0.7/6.3 mm) to 24.5% (2.06/8.4 mm) for IVRO. Our current report demonstrated a relapse potency of 11.8% (1.5/12/7). In addition, our patients who underwent surgical mandibular setback greater than 10 mm showed no obvious relapse. This indicated that the modified IVRO surveyed in this study presented good skeletal stability even when treating patients with severe prognathism of the mandible. The postoperative stability of both IVRO and SSRO has been extensively evaluated. However, the causes of relapse remain unclear. The most frequently proposed cause of relapse is the amount of mandibular setback. Conclusions about the correlation between the amount of mandibular setback and the tendency to relapse are still controversial. Phillips et al,14 Kobayashi et al,18 and Schatz and Tsimas19 found that the amount of surgical setback was correlated with relapse. By contrast, no relationship between the amount of surgical movement and the degree of relapse was found by Sorokolit and Nanda22 and Mobarak et al.23 Our findings indicated that the changes in Me (T32) between the immediate postsurgical stage and the 2-year postoperative stage revealed no significant difference. Anatomical differences of individual patients and the preference of surgeon to carry out the procedure are two factors that affected the length of the osteotomy. Tornes investigated the osteotomy length and the postoperative stability of 80 patients treated with vertical subcondylar ramus (VSCR) osteotomy.24 He concluded that the osteotomy length appeared to be a minor factor in postoperative stability. However, the osteotomy length of IVRO is greater than that of VSCR osteotomy and can go beyond the gonial point on the lower border of the mandible. Despite previous findings, in 1-by-1 hierarchical modeling analyses, PireIo and MeT21/PireIo did not 275 significantly differ in terms of the relationship between the osteotomy length of IVRO and postoperative skeletal relapse. In the 1-by-2 model, there was still no significant difference regarding the postoperative skeletal relapse. However, it might have been significant if there had been more combined variables that contributed to the relationship between the osteotomy length and postoperative stability. Finally, there was a significant difference in the combined variables (MeT21, PireIo, and MeT21/PireIo), which correlated with the postoperative stability. The MeT21 and MeT21/PireIo were significant factors responsible for postoperative stability. Therefore, we found that the combination of osteotomy design and its available setback capacity could be primary factors affecting its postoperative stability. Research methods and surgical approaches can greatly vary among surgeons even in the same hospital. This is a major problem for surgeons when they try to select the best techniques to minimize postoperative skeletal changes. Interosseous semirigid or rigid fixation is commonly used with SSRO technique. However, fixation between distal and proximal segments was found to be difficult, and hence it cannot be mandatory for IVRO technique. Instead of interosseous fixation, an acrylic interocclusal splint and maxillomandibular fixation were used in this study to immobilize the jawbones for 6 weeks after surgery. The bilateral temporomandibular joint gradually and physiologically adapts. None of our patients reported any complications of temporomandibular disorders after surgery. The postoperative relationship of the jawbones of our patients was stable, and the relapse rate was less than 10%. Furthermore, reports regarding postoperative permanent complications of our patients were rare. It is important for surgeons to evaluate postoperative complications to refine the surgical technique. A thorough investigation of temporary and permanent postoperative complications will be conducted in the future. In conclusion, our study demonstrated 2-year stable surgical outcomes by applying a modified IVRO to correct mandibular prognathism. The postoperative stability of IVRO was found to be affected by multiple variables rather than merely a single factor. The results showed that three combined factors of MeT21, PireIo, and the ratio (MeT21/ PireIo) presented a statistically significant influence on postoperative stability. Conflicts of interest The authors have no conflicts of interest relevant to this article. References 1. Bell WH, Hall HD, White RP, Proffit WR. Mandibular excess. In: Surgical Correction of Dentofacial Deformities. Philadelphia, PA: WB Saunders, 1980:844e1013. 2. Steinhäuser EW. Historical development of orthognathic surgery. J Craniomaxillofac Surg 1996;24:195e204. 3. Bell WH, Levy BM. Revascularization and bone healing after anterior mandibular osteotomy. J Oral Surg 1970;28:196e203. 276 4. Ghali GE, Sikes Jr JW. Intraoral vertical ramus osteotomy as the preferred treatment for mandibular prognathism. J Oral Maxillofac Surg 2000;58:313e5. 5. Al-Bishri A, Barghash Z, Rosenquist J, Sunzel B. Neurosensory disturbance after sagittal split and intraoral vertical ramus osteotomy: as reported in questionnaires and patients’ records. Int J Oral Maxillofac Surg 2005;34:247e51. 6. Lai SS, Tseng YC, Huang IY, Yang YH, Shen YS, Chen CM. Skeletal changes after modified intraoral vertical ramus osteotomy for correction of mandibular prognathism. J Plast Reconstr Aesthet Surg 2007;60:139e45. 7. Bell WH, Schendel SA. Biologic basis for modification of the sagittal ramus split operation. J Oral Surg 1977;35:362e9. 8. Trauner R, Obwegeser H. The surgical correction of mandibular prognathism and retrognathia with consideration of genioplasty. I. Surgical procedures to correct mandibular prognathism and reshaping of the chin. Oral Surg oral Med Oral Pathol 1957;10:677e89. 9. Dal Pont G. Retromolar osteotomy for the correction of prognathism. J Oral Surg Anesth Hosp Dent Serv 1961;19:42e7. 10. Epker BN. Modifications in the sagittal osteotomy of the mandible. J Oral Surg 1977;35:157e9. 11. Moose SM. Surgical correction of mandibular prognathism by intraoral subcondylar osteotomy. J Oral Surg Anesth Hosp Dent Serv 1964;22:197e202. 12. Winstanley RP. Subcondylar osteotomy of the mandible and the intraoral approach. Br J Oral Surg 1968;6:134e6. 13. Hall HD, McKenna SJ. Further refinement and evaluation of intraoral vertical ramus osteotomy. J Oral Maxillofac Surg 1987;45:684e8. 14. Phillips C, Zaytourn Jr HS, Thomas PM, Terry BC. Skeletal alterations following TOVRO or BSSO procedures. Int J Adult Orthodon Orthognath Surg 1986;1:203e13. C.-M. Chen et al 15. Proffit WR, Phillips C, Dann 4th C, Turvey TA. Stability after surgical-orthodontic correction of skeletal class III malocclusion. I. Mandibular setback. Int J Adult Orthodon Orthognath Surg 1991;6:7e18. 16. Wolford LM. The sagittal split ramus osteotomy as the preferred treatment for mandibular prognathism. J Oral Maxillofac Surg 2000;58:310e2. 17. Franco JE, Van Sickels JE, Thrash WJ. Factors contributing to relapse in rigidly fixed mandibular setbacks. J Oral Maxillofac Surg 1989;47:451e6. 18. Kobayashi T, Watanabe I, Ueda K, Nakajima T. Stability of the mandible after sagittal ramus osteotomy for correction of prognathism. J Oral Maxillofac Surg 1986;44:693e7. 19. Schatz JP, Tsimas P. Cephalometric evaluation of surgicalorthodontic treatment of skeletal class III malocclusion. Int J Adult Orthodon Orthognath Surg 1995;10:173e80. 20. Greebe RB, Tuinzing DB. Overcorrection and relapse after the intraoral vertical ramus osteotomy. A one-year postoperative review of thirty-five patients. Oral Surg Oral Med Oral Pathol 1982;54:382e4. 21. Chen CM, Lee HE, Yang CF, et al. Intraoral vertical ramus osteotomy for correction of mandibular prognathism: longterm stability. Ann Plast Surg 2008;61:52e5. 22. Sorokolit CA, Nanda RS. Assessment of the stability of mandibular setback procedures with rigid fixation. J Oral Maxillofac Surg 1990;48:817e22. 23. Mobarak KA, Krogstad O, Espeland L, Lyberg T. Long-term stability of mandibular setback surgery: a follow-up of 80 bilateral sagittal split osteotomy patients. Int J Adult Orthodon Orthognath Surg 2000;15:83e95. 24. Tornes K. Osteotomy length and postoperative stability in vertical subcondylar ramus osteotomy. Acta Odontol Scand 1989;47:81e8.