Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
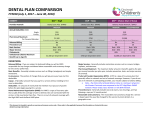
Blue Cross and Blue Shield of Texas ASO - Dental Summary of Benefits Prepared for Weatherford International Ltd. Account Number: 039865 Group Number: 40285 TYPE OF SERVICE NETWORK OUT-OF-NETWORK $25 per Individual / $50 per Family Yes $2,000 $50 per Individual / $100 per Family Yes $1,500 100% 100% 100% 100% 80% after plan ded. 80% after plan ded. 80% after plan ded. 80% after plan ded. 80% after plan ded. 80% after plan ded. 80% after plan ded. 80% after plan ded. 80% after plan ded. 80% after plan ded. 50% after plan ded. 50% after plan ded. 50% after plan ded. 50% after plan ded. 50% after plan ded. 50% after plan ded. GENERAL PROVISIONS Calendar Year Deductible Prior Deductible Credit Calendar Year Maximum per Participant (In-network and Out-of-network deductibles and maximums update each other) DIAGNOSTIC AND PREVENTIVE CARE BENEFITS (Deductible Waived) Oral Examinations (2 exams per Calendar Year) Prophylaxis (2 exams per Calendar Year) Fluoride Treatment (up to age 19; One per calendar year) Dental X-rays MISCELLANEOUS SERVICES (Deductible Waived) Sealants (No age limit – one every 3 years) Space Maintainers (No age limit) Labs and Tests Palliative Care Perio Maintenance RESTORATIVE SERVICES Routine Fillings (amalgams and resins) GENERAL SERVICES Intravenous sedation General Anesthesia Stainless Steel Crowns Denture Adjustments Denture Repairs Recement Bridge ENDODONTIC SERVICES Root Canals Direct pulp caps PERIODONTAL SERVICES Scaling and root planing Osseous surgery ORAL SURGERY SERVICES Simple/Surgical tooth extractions CROWNS, INLAYS/ONLAYS SERVICES Inlays, Onlays and Crowns (other than temporary crowns) IMPLANT SERVICES PROSTHODONTIC SERVICES Bridges Full and partial dentures ORTHODONTIC BENEFITS Orthodontic Diagnostic Procedures and Treatment (Child up to age 25 and Adult) Lifetime deductible applies Lifetime Maximum per Participant Yes 50% $25 Orthodontic ded. 50% $50 Orthodontic ded. $2000 This is a general Summary of your benefit design. Please refer to your benefit booklet for other details and for limitations and exclusions. The following eligibility provisions apply: Effective 9/1/2011dependents covered to age 26, regardless of marital, student or employment status. Retirees are not eligible for coverage. Open enrollment – employees and/or dependents not presently covered may enroll for dental 30 days prior to the anniversary date. A preexisting condition exclusion will apply to expenses involving the replacement of teeth that were missing prior to the effective date of the dental contract. This exclusion will not apply to: Any participant who becomes effective on the dental contract date. Any participant who has been continuously covered for 24 months under a group dental care contract with BCBSTX which included prosthetic benefits. DEN8-FRSTG-PPO-SOB REV. 05/26/09 * A Division of Health Care Service Corporation, a Mutual Legal Reserve Company, an Independent Licensee of the Blue Cross and Blue Shield Association Blue Cross and Blue Shield of Texas ASO - Dental Summary of Benefits Prepared for Weatherford International Ltd. Account Number: 039865 Group Number: 40285 When the course of treatment will be in excess of $200, a predetermination request should be submitted to BCBSTX in advance of treatment. Accums apply to calendar year deductible, 4th quarter carryover deductible from 2008, annual max and orthodontic lifetime max and deductible. Effective 01/01/2011 the plan will add dental implants as covered benefit Effective 9/1/2012 members who are enrolled in the medical and dental plan and are Pregnant or have Cardiovascular Disease or Diabetes, will be offered a third scaling and root planning service, routine cleaning and office visit, and periodontal maintenance cleaning per calendar year. These additional services will be paid at 100% and will apply to the calendar year maximum. Please note that our dental is a “freestanding” product and can be purchased separately from the health product, i.e., an employee can have only himself covered for health, but have dental for the family and vice versa. DEN8-FRSTG-PPO-SOB REV. 05/26/09 * A Division of Health Care Service Corporation, a Mutual Legal Reserve Company, an Independent Licensee of the Blue Cross and Blue Shield Association