Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
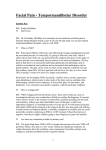
® XXI • NO5 1• •DECEMBER JUNE 2013 2014 VOLVOL XXII • NO Initial Findings fromVol. XXI, Issue 1 the OPPERA Study: VOL XI NO• Medicine 1 JUNE • 2013 Editorial Board Implications for Translational Pain P Editor-in-Chief ain researchers and clini- Jane C. Ballantyne, MD, FRCA cians have over the Anesthesiology, Pain Medicine USA last several decades advanced our Advisory Board knowledge and abilities to as- sessMichael J. Cousins, MD, DSC the underlying neural mechanisms June 2013 Psychosocial Aspects of Chronic Pelvic Pain many common chronic pain conditions, is a mosaic of measurable clinical signs and symptoms that can be viewed as Pain is unwanted, is unfortunately common, and remains essential for survival (i.e., a set of intermediate phenotypes evading danger) and facilitatingthat medical diagnoses. This complex amalgamation of andAustralia putative etiological pathways that aresensation, temporally influenced environemotions, andby thoughts manifests itself as pain behavior. Pain is a motimental events such as history of injury, 1 mediate temporomandibular disorder infections, life-relevant stressors, (TMD) and other persistent or chronic and a variety of chemical exposures.11 pain conditions. What has emerged is Environmental events or exposures in a model that recognizes that TMD, like turn influence the expression patterns Pain Medicine, Palliative Medicine vating factor for physician consultations and for emergency department visits and is a variety of signaling pathways that What Are the Phenotypic, Genetic, and Environmental Variables that Define or Characterize the Signs and Symptoms of TMD? manifest as quantitative and quali- Case-control studies have identified tative intermediate phenotypes that de- several intermediate phenotypes that fine the TMD patient at a specific point differentiate TMD cases from non- in time. With the progression of time, TMD cases.3 Recent findings from the the types and degree of exposure to en- Orofacial Pain: Prospective Evalua- vironmental exposures accumulate, re- tion and Risk Assessment (OPPERA) sulting in the signs and symptoms that case-control study of chronic TMD Center for Pain Research and Innovation, University of North Carolina at Chapel Hill, Chapel Hill, N. Car., USA define a TMD patient. With time and demonstrate that people with chronic with exposure to both protective ex- TMD differ from people without TMD University of Florida, College of Dentistry, and Pain Research and Intervention Center of Excellence, Gainesville, Fla., USA posures (e.g., treatments) and negative across multiple phenotypic areas influences (e.g., tobacco smoke), there including, but not limited to, sociode- are temporally dependent changes in mographic factors, clinical variables, the severity of self-reported facial pain, psychological functioning, pain disability, and related comorbid condi- sensitivity, and autonomic domains. tions. The successful diagnosis and The strongest associations with TMD William Maixner, DDS, PhD1 Roger B. Fillingim, PhD2 Anne E. Sanders, PhD3 Eric Bair, PhD1,4 Joel D. Greenspan, PhD5 Richard Ohrbach, DDS, PhD6 Ron Dubner, DDS, PhD5 Luda Diatchenko, MD, PhD1 Shad B. Smith, PhD1 Charles Knott, MPA7 Gary D. Slade, BDSc, PhD1,3,8 1 2 Department of Epidemiology, University of North Carolina at Chapel Hill, Chapel Hill, N. Car., USA 3 Department of Biostatistics, University of North Carolina at Chapel Hill, Chapel Hill, N. Car., USA 4 of multiple genes and the activity of treatment of TMD patients requires an were observed for measures related Department of Neural and Pain Sciences, and Brotman Facial Pain Clinic, University of Maryland Dental School of Dentistry, Baltimore, Md., USA understanding of the risk factors (ge- to bodily tenderness (e.g., pressure netic and environmental) that mediate pain thresholds; Fig. 1) and salience of the biological processes regulating the symptoms (e.g., somatic awareness). Department of Oral Diagnostic Sciences, University at Buffalo, Buffalo, New York, USA expression of intermediate phenotypes Weaker associations with chronic that define the signs and symptoms of TMD emerged for measures of mood, Battelle Memorial Institute, Durham, N. Car., USA TMD. Empowered by years of knowl- autonomic function, temporal regula- edge generated from both clinical and tion of pain, and genetic variants. The basic science discoveries, we have broad range of phenotypic domains begun this quest. that distinguish chronic TMD cases 5 6 7 Department of Dental Ecology, University of North Carolina at Chapel Hill, Chapel Hill, N. Car., USA 8 PAIN: CLINICAL UPDATES • DECEMBER 2014 1 Fig. 1. Pressure pain thresholds (PPTs) derived at 10 body sites for temporomandibular disorder (TMD) cases (red, N = 186) and a sample of control subjects without TMD (blue, N = 1621) derived from 25,103 questionnaires in the OPPERA study. Bars depict mean and standard error. In all cases, TMD cases have lower PPTs than controls, in both cranial and extracranial sites. (All P < 0.001.) TMD Cases Controls from controls reflects the complex, conditions, a greater number of non- measures emerged as the most impor- heterogeneous, and multidimensional specific orofacial symptoms, and higher tant predictors. TMD incidence was nature of TMD etiopathogenesis, scores on the bodily pain scale from the strongly associated with the SF-12v2 which we have referred to as a “web Short Form-12 Health Survey, version bodily pain subscale, a single question of causation.”9 2 (SF-12v2). The first two measures are about the degree to which pain inter- notable because they are simple check- feres with work. OPPERA investigators also measured the incidence of TMD in a lists of commonly occurring health- prospective cohort study of first-onset related conditions, rather than precise, several genetic associations with TMD TMD.16 The study design permits psychometrically validated measures case status, providing important clues evaluation of the temporal sequence of a specific construct. Specifically, the as to the biological pathways that may between putative cause and develop- checklist of 20 comorbid conditions, contribute to the molecular etiology of ment of TMD, unlike the case-control which was created for the OPPERA TMD.18 The association analysis with study design, which cannot distinguish study, includes both painful conditions chronic TMD provided evidence sup- bidirectional or reverse relationships (e.g., irritable bowel syndrome) and porting two genes previously reported between TMD and risk factors. In the other conditions that are not primar- to contribute to related conditions: prospective cohort study, pain symp- ily painful (e.g. depression). The list serotonin receptor 2A (HTR2A), which toms were monitored closely using of six nonspecific orofacial symptoms encodes a receptor for the neurotrans- quarterly (three-monthly) question- includes aversive sensations of the mitter serotonin; and catechol-O-meth- naires that were completed by 2737 face and jaw that are not primarily yltransferase (COMT), which encodes study participants who had no history painful (e.g., fatigue and stiffness) an enzyme that regulates levels of cat- of TMD at enrollment. Facial pain or that reflect sub-pain symptoms echolamines, including the neurotrans- symptoms occurred at six times the (e.g., soreness or tenderness). These mitters dopamine, epinephrine, and The case-control study revealed expected rate when both headache and other bodily pain were also reported (Fig. 2). The quarterly questionnaires revealed a “symptom iceberg” of facial pain in the community: one third of study participants reported at least one month in which they had facial pain for at least five days per month; moreover, most of them did not seek health care or use analgesics.17 Participants who reported facial pain symptoms were invited to research clinics where trained examiners identified 260 cases of first-onset, clinical TMD—an overall rate of 3.5% of people per annum. Variables from the health status domain made the greatest contribution to predicting incident clinical TMD, followed closely by the psychosocial and clinical orofacial domains. Sociodemographic, pain sensitivity, and cardiac autonomic function domains made smaller contributions. Among the individual variables, three stood out as the most important predictors: a greater number of comorbid PAIN: CLINICAL UPDATES • DECEMBER 2014 Fig. 2. Pain symptom episodes reported in quarterly screening questionnaires in the OPPERA prospective cohort study. Painful temporomandibular disorder (TMD) symptoms were reports of TMD-like pain lasting ≥5 days per month for ≥1 month of the reporting period. Headaches are reports of ≥5 headaches within the most recent month of the reporting period. Body pain was a report of pain in ≥1 of 10 body locations lasting for ≥1 days in the same reporting period. Multiplication numbers in white rectangles represent the ratio of the observed number of overlapping episodes relative to the expected number of episodes that would have occurred had the symptoms occurred independently. 3 norepinephrine. Other genes emerged rs10809907). However, investigators While the pain field has advanced as potential new genetic risk factors for should examine the observed associa- significantly in measuring molecular TMD, including glucocorticoid receptor tions with intermediate phenotypes and phenotypic signatures associated (NR3C1), calmodulin-dependent protein in other cohorts before concluding a with chronic pain conditions, there is kinase 4 (CAMK4), muscarinic cholin- true association. still a substantial need to identify and ergic receptor (CHRM2), interferon- The knowledge generated by these to measure key environmental expo- related developmental regulatory 1 genetic association studies furthers our sures that contribute to the onset and (IFRD1), and G-protein coupled receptor understanding of the putative genetic chronicity of chronic pain conditions kinase 5 (GRK5). architecture and associated molecular such as TMD. In the prospective study, genetic mechanisms that contribute to the on- The initial outcomes of the OP- variants were investigated for their set and persistence of TMD. By impli- PERA study show unequivocally that association with two sets of outcomes cation, these mechanisms might also TMD is a complex disorder that is best related to the risk of first-onset contribute to other common persistent envisaged within a biopsychosocial TMD: clinically classified first-onset pain conditions. Understanding the model of illness, which acknowledges TMD and five “intermediate pheno- molecular basis of etiological pathways the influence of genetic and envi- types” measured at enrollment that will permit the development of new ronmental factors. It is a misnomer, emerged as predictors of clinical therapeutic approaches for treating and no longer appropriate, to regard TMD. The five intermediate pheno- conditions such as TMD, along with TMD solely as a localized orofacial types were: (1) the number of comor- related common chronic pain condi- pain condition. For the majority of bid health condition14; (2) the number tions that are highly prevalent with people with chronic TMD, the condi- of nonspecific orofacial symptoms12; TMD and share common pathophysi- tion is a multisystem disorder with (3) global psychological symptoms2; ological processes. overlapping comorbidity. One of the (4) stress and negative affect2; and A variety of environmental influ- clinical challenges is to distinguish (5) heat pain temporal summation.5 ences or exposures are related to risk incidental findings from those that The latter three measures were latent of TMD onset or chronicity. History have prognostic or etiological signifi- constructs obtained from principal of injury to the jaw, as reported on cance, which will require relatively component analysis. While no single study entry, was associated with TMD large-scale prospective studies that nucleotide polymorphism (SNP) was case status but not with TMD onset. are sufficiently powered to identify significantly associated with risk of Increased TMD incidence was associ- risk factors that predict or contrib- TMD onset, several SNPs exceeded ated with greater digit length ratio ute to the processes that mediate the false discovery rate thresholds for (D2:D4), a marker of elevated estro- transition from acute to chronic pain. association with an intermediate phe- gen relative to testosterone in utero. A clear picture is emerging that TMD notype.19 A SNP encoding a sodium However, digit length ratio did not is a mosaic of diverse symptoms and channel protein (SCN1A, rs6432860) differentiate chronic TMD cases from health-related characteristics that are was significantly associated with controls. Current or former smokers strong predictors of first-onset TMD, nonspecific orofacial symptoms, as had a greater risk of developing TMD and not merely consequences of TMD. was a SNP encoding an angiotensin in comparison to those who had never The degree to which these markers enzyme (ACE2, rs1514280). Another smoked. One mechanism by which of onset predict the transition to a SNP encoding enzymes that catalyze these exposures might influence pain more severe and chronic form of TMD the conversion of arachidonate to is through epigenetic effects on pain- remains an open question. prostaglandin (PTGS1, rs3842803) signaling pathways. Finally, chrono- was significantly associated with logical age, which may represent a global psychosocial symptoms, as was measure of the time epoch that an in- a SNP encoding an amyloid precur- dividual has experienced and biologi- sor protein (APP, rs466448). Finally, cally responded to both negative and temporal summation of heat pain positive environmental exposures, was Case-control and prospective cohort was significantly associated with a positively associated with TMD case studies such as OPPERA can pro- multiple PDZ domain protein (MPDZ, status and the risk of developing TMD. vide important clues regarding the 4 How Can We Translate the Results of Population-Based Cohort Studies into Clinical Practice? PAIN: CLINICAL UPDATES • DECEMBER 2014 etiological mechanisms that contrib- one or more phenotypic measure, ute to the onset and persistence of a has been applied to measures of pain variety of pain conditions. OPPERA sensitivity made using quantitative has collected over 200 phenotypic sensory testing (QST).7 The findings variables and approximately 3500 demonstrate that people can be strati- genetic variables from several thou- fied based on responses to multiple sand individuals. Several interesting stimulus modalities. Several studies findings have and will continue to have reported such analyses in fi- emerge from this data set, but how do bromyalgia, low back pain, and TMD, we translate all of this information including clustering of patients ac- into clinically useful tools that will cording to physical and psychosocial assist clinicians with the diagnosis symptoms,15,20–22 QST responses and and treatment of patients with TMD comorbid symptoms,4,13 and biological and related conditions? First, we must markers and psychologically assessed account for the fact that TMD is a factors.10 Although the nature of the multisystem disorder with overlap- subgroups identified varies across ping comorbidity that is dictated by studies owing to differences in the the nature and types of environ- phenotypes used to generate the mental exposures combined with the clusters, these studies demonstrate individual’s genetic susceptibility to the feasibility of deconstructing the Maree T. Smith, PhD express the mosaic of intermediate heterogeneous TMD population into Pharmacology Australia phenotypes that characterizes a TMD more homogeneous subgroups. Other patient. It is clear that TMD patients, methods of classification are avail- as well as individuals with related able, including latent class analysis chronic pain conditions, represent a and machine learning approaches.6,8 heterogeneous population of patients The genetic and associated molecular reporting orofacial pain. Advanced pathways that underlie the identi- methods of data analysis need to be fied affected subgroups have not yet applied to the multiple phenotypic been adequately assessed. Neverthe- domains (psychological, pain sensitiv- less, the identification of diagnostic ity, autonomic, and clinical) to reveal subgroups using clinically practical more homogeneous subgroups within measures of intermediate phenotypes the population. Each domain can be coupled with the identification of the examined and interpreted indepen- molecular profiles that underlie spe- dently; however, the findings can also cific subgroups holds great promise be examined across domains in order in developing mechanistic diagnostic to identify patient profiles or mosa- protocols and identifying novel bio- ics that reflect differing pathophysi- logical targets and pathways for both ological mechanisms and distinct pharmacological and nonpharmaco- underlying genetic and molecular logical therapeutic interventions. architectures. Statistical approaches can be applied to identify profiles across phenotypic domains that reflect subpopulations of TMD patients. What Is on the Horizon for the Diagnosis and Treatment of TMD and Related Disorders? For example, cluster analysis, a set The OPPERA team believes that the of statistical classification methods future is bright for making major to identify groups of people that headway with respect to new and show similar characteristics across clinically useful diagnostic tools and PAIN: CLINICAL UPDATES • DECEMBER 2014 Editorial Board Editor-in-Chief Jane C. Ballantyne, MD, FRCA Anesthesiology, Pain Medicine USA Advisory Board Michael J. Cousins, MD, DSC Pain Medicine, Palliative Medicine Australia Maria Adele Giamberardino, MD Internal Medicine, Physiology Italy Robert N. Jamison, PhD Psychology, Pain Assessment USA Patricia A. McGrath, PhD Psychology, Pediatric Pain Canada M.R. Rajagopal, MD Pain Medicine, Palliative Medicine India Claudia Sommer, MD Neurology Germany Harriët M. Wittink, PhD, PT Physical Therapy The Netherlands Publishing Daniel J. Levin, Publications Director Elizabeth Endres, Consulting Editor Timely topics in pain research and treatment have been selected for publication, but the information provided and opinions expressed have not involved any verification of the findings, conclusions, and opinions by IASP. Thus, opinions expressed in Pain: Clinical Updates do not necessarily reflect those of IASP or of the Officers or Councilors. No responsibility is assumed by IASP for any injury and/or damage to persons or property as a matter of product liability, negligence, or from any use of any methods, products, instruction, or ideas contained in the material herein. Because of the rapid advances in the medical sciences, the publisher recommends independent verification of diagnoses and drug dosages. © Copyright 2014 International Association for the Study of Pain. All rights reserved. For permission to reprint or translate this article, contact: International Association for the Study of Pain 1510 H Street NW, Suite 600, Washington, D.C. 20005-1020, USA Tel: +1-202-524-5300 Fax: +1-202-524-5301 Email: [email protected] www.iasp-pain.org 5 therapies for treating TMD and related continuing revolution in our under- In addition, we express our gratitude to conditions. New diagnostic methods ca- standing of the molecular basis of pain the participants who have devoted time pable of accurately classifying patients conditions will result in the identifica- and effort in support of this research. into discrete subpopulations based on tion of new subgroup specific drug biopsychosocial phenotypes in addition targets and the development of new Disclosures to anatomically specified criteria will drugs, biologics, and procedures that This work was supported by NIH grant soon become available. We envision are effective in treating large subpopu- U01DE017018. The OPPERA program that these additional tools will provide lations of TMD patients. The success of also acknowledges resources specifically clinicians with a new way of diagnos- this process will require a close symbi- provided for this project by the respec- ing and identifying treatment algo- otic relationship between clinical and tive host universities: University at Buf- rithms based on patient subtype rather basic scientists for the translational falo, University of Florida, University of than only on a diagnosis according to process to be fully effective.1 In our Maryland-Baltimore, and University of anatomical site (e.g., lower back pain, view, the quest for translational pain North Carolina-Chapel Hill. Gary Slade irritable bowel syndrome, or TMD). treatment is in its infancy but shows and Roger Fillingim are consultants Methods that are feasible in the clinical great promise in developing new diag- and equity stock holders, and William setting and that predict the likelihood nostic methods and therapeutics. Maixner and Luda Diatchenko are of clinical pain progression from acute cofounders and equity stock holders in to chronic status are also close at hand. Acknowledgments In parallel with the development of The authors would like to thank the ing research services in personalized methods that permit the identification OPPERA research staff for their pain medication and diagnostics. Other of subpopulations of TMD patients, the invaluable contributions to this work. authors report no conflicts of interest. References 1. Diatchenko L, Fillingim RB, Smith SB, Maixner W. The phenotypic and genetic signatures of common musculoskeletal pain conditions. Nat Rev Rheumatol 2013;9:340–50. 2. Fillingim RB, Ohrbach R, Greenspan JD, Knott C, Diatchenko L, Dubner R, Bair E, Baraian C, Mack N, Slade GD, Maixner W. Psychological factors associated with development of TMD: the OPPERA prospective cohort study. J Pain 2013;14:T75–90. 3. Fillingim RB, Slade GD, Diatchenko L, Dubner R, Greenspan JD, Knott C, Ohrbach R, Maixner W. Summary of findings from the OPPERA baseline case-control study: implications and future directions. J Pain 2011;12:T102–7. 4. Giesecke T, Williams DA, Harris RE, Cupps TR, Tian X, Tian TX, Gracely RH, Clauw DJ. Subgrouping of fibromyalgia patients on the basis of pressurepain thresholds and psychological factors. Arthritis Rheum 2003;48:2916–22. 5. Greenspan JD, Slade GD, Bair E, Dubner R, Fillingim RB, Ohrbach R, Knott C, Diatchenko L, Liu Q, Maixner W. Pain sensitivity and autonomic factors associated with development of TMD: the OPPERA prospective cohort study. J Pain 2013;14:T63-74.e1–6. 6. Hastie T, Tibshirani R, Friedman J, Hastie T, Friedman J, Tibshirani R. The elements of statistical learning. Springer; 2009. 7. Hastie BA, Riley JL 3rd, Robinson ME, Glover T, Campbell CM, Staud R, Fillingim RB. Cluster analysis of multiple experimental pain modalities. Pain 2005;116:227–37. 8. Kato K, Sullivan PF, Pedersen NL. Latent class analysis of functional somatic symptoms in a population-based sample of twins. J Psychosom Res 2010;68:447–53. 9. Krieger N. Epidemiology and the web of causation: has anyone seen the spider? Soc Sci Med 1994;39:887–903. Algynomics, Inc., a company provid- 13.Rehm SE, Koroschetz J, Gockel U, Brosz M, Freynhagen R, Tolle TR, Baron R. A cross-sectional survey of 3035 patients with fibromyalgia: subgroups of patients with typical comorbidities and sensory symptom profiles. Rheumatology (Oxford) 2010;49:1146–1152. 14.Sanders AE, Slade GD, Bair E, Fillingim RB, Knott C, Dubner R, Greenspan JD, Maixner W, Ohrbach R. General health status and incidence of first-onset temporomandibular disorder: the OPPERA prospective cohort study. J Pain 2013;14:T51–62. 15.Scholz J, Mannion RJ, Hord DE, Griffin RS, Rawal B, Zheng H, Scoffings D, Phillips A, Guo J, Laing RJ, Abdi S, Decosterd I, Woolf CJ. A novel tool for the assessment of pain: validation in low back pain. PLoS Med 2009;6:e1000047. 16.Slade GD, Fillingim RB, Sanders AE, Bair E, Greenspan JD, Ohrbach R, Dubner R, Diatchenko L, Smith SB, Knott C, Maixner W. Summary of findings from the OPPERA prospective cohort study of incidence of first-onset temporomandibular disorder: implications and future directions. J Pain 2013;14:T116–24. 17.Slade GD, Sanders AE, Bair E, Brownstein N, Dampier D, Knott C, Fillingim R, Maixner WO, Smith S, Greenspan J, Dubner R, Ohrbach R. Preclinical episodes of orofacial pain symptoms and their association with health care behaviors in the OPPERA prospective cohort study. Pain 2013;154:750–60. 18.Smith SB, Maixner DW, Greenspan JD, Dubner R, Fillingim RB, Ohrbach R, Knott C, Slade GD, Bair E, Gibson DG, Zaykin DV, Weir BS, Maixner W, Diatchenko L. Potential genetic risk factors for chronic TMD: genetic associations from the OPPERA case control study. J Pain 2011;12:T92–101. 19.Smith SB, Mir E, Bair E, Slade GD, Dubner R, Fillingim RB, Greenspan JD, Ohrbach R, Knott C, Weir B, Maixner W, Diatchenko L. Genetic variants associated with development of TMD and its intermediate phenotypes: the genetic architecture of TMD in the OPPERA prospective cohort study. J Pain 2013;14:T91–101.e1–3. 10.Loevinger BL, Shirtcliff EA, Muller D, Alonso C, Coe CL. Delineating psychological and biomedical profiles in a heterogeneous fibromyalgia population using cluster analysis. Clin Rheumatol 2012;31:677–85. 20.Suvinen TI, Reade PC, Hanes KR, Kononen M, Kemppainen P. Temporomandibular disorder subtypes according to self-reported physical and psychosocial variables in female patients: a re-evaluation. J Oral Rehabil 2005;32:166–73. 11.Maixner W, Diatchenko L, Dubner R, Fillingim RB, Greenspan JD, Knott C, Ohrbach R, Weir B, Slade GD. Orofacial pain prospective evaluation and risk assessment study: the OPPERA study. J Pain 2011;12:T4–11.e1–2. 21.Velly AM, Philippe P, Gornitsky M. Heterogeneity of temporomandibular disorders: cluster and case-control analyses. J Oral Rehabil 2002;29:969–79. 12.Ohrbach R, Bair E, Fillingim RB, Gonzalez Y, Gordon SM, Lim PF, RibeiroDasilva M, Diatchenko L, Dubner R, Greenspan JD, Knott C, Maixner W, Smith SB, Slade GD. Clinical orofacial characteristics associated with risk of first-onset TMD: the OPPERA prospective cohort study. J Pain 2013;14:T33–50. 6 22.Wilson HD, Starz TW, Robinson JP, Turk DC. Heterogeneity within the fibromyalgia population: theoretical implications of variable tender point severity ratings. J Rheumatol 2009;36:2795–801. PAIN: CLINICAL UPDATES • DECEMBER 2014