Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
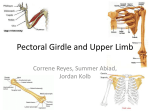
Shoulder Girdle Region Neumann Chapter 5 REVIEW AND HIGHLIGHTS OF OSTEOLOGY & ARTHROLOGY Sternum: Manubrium (sternal notch), Body, Xiphoid process Scapula Glenoid fossa Acromion and Coracoid Processes Spine and Borders Superior & Inferior Angles Alignment/Orientation: lies against the rib cage at a 30 – 40° angle from the frontal plane. Many of its osteokinematics are described relative to the frontal plane - - why? Scapula and Spinous Process spatial relationships: Clavicle: numerous ms. and lig. attachments Humerus (Proximal Half) Head & Neck - The glenoid fossa is about 1/4 to 1/3 the size of the humeral head. Greater tubercle, Lesser tubercle, Intertubercular (bicipital) groove Deltoid tuberosity Angle of inclination 135° Angle of torsion; Retroversion of ~30° (b/c of the plane of the scapula) SCAPULOTHORACIC ARTICULATION Articulation of scapula with thoracic wall. Not a synovial joint; lacks most of the characteristics of a true joint. Stability and position: maintained by muscular attachments (ie. scapular stabilizing muscles) ACROMIOCLAVICULAR (AC) JOINT: Plane (nonaxial) synovial joint between lateral end of clavicle and medial border of acromion. Fibrocartiliage disk (meniscus) in the joint increases congruence/stability and absorbs forces; AC joint is actually a cartilaginous joint through age two. Over time, joint space develops, usually maintaining some fibrocartilage (disk) within the joint. Well into adulthood, the disk gradually degenerates with no apparent impairment of movement (some popping and clicking joint noise may occur). Ligaments: AC Ligament - fairly weak; reinforces joint capsule Coracoclavicular ligaments – composed of 2 strong ligaments: Conoid ligament , Trapezoid ligament Trapezoid ligament inserts more laterally and is oriented more horizontally than the Conoid. Functions: resist depression and medial displacement of scapula; transfers these forces to the strong and stable SC joint. STERNOCLAVICULAR (SC) JOINT Only bony & joint attachment of upper extremity to axial skeleton. Classification varies from irregular Saddle (biaxial) to Plane (non-axial) synovial joint between sternum and clavicle. However, it has 3 degrees of freedom. A Fibrocartilage Disk (meniscus) in the joint increases joint congruence/stability and absorbs forces transmitted along the clavicle. Page 1 Ligaments reinforce the joint capsule and allow limited movement of the clavicle. Anterior and posterior SC ligaments Costoclavicular ligament - from inf. aspect of clavicle to superior aspect of 1st rib Interclavicular ligament - between sternal ends of clavicles GLENOHUMERAL (GH) JOINT Ball and socket triaxial synovial joint formed by articulation of humeral head with glenoid fossa of scapula. This is an unstable but very mobile arrangement. Glenoid labrum - fibrocartilage and dense connective tissue rim that deepens the fossa Capsule / Ligaments: Capsule: Large thin joint capsule attached to margin of fossa and anatomical neck of humerus. Capsule strengthened by ligaments and insertion of rotator cuff tendons. Inf. capsule loose with arm at side - forms axillary pouch. Superior capsule tight with arm at side. Glenohumeral (GH) Ligaments: Superior, Middle & Inferior; thickenings of the capsule. Limit ant-inf movement of humeral head; inferior lig is key stabilizer in 90-90 Ext Rotat position (cocking phase of throw) Coracohumeral: Supports superior portion of joint. Superficial to the Superior GH Ligament Subacromial space: Between the coracoacromial arch (acromion, coracoacromial ligament, and coracoid process) and the humeral head. The Fibro-osseus Arch protects the humeral head and contents of subacromial space from direct trauma from above. Contents: subacromial bursa, supraspinatus tendon, joint capsule, biceps long head tendon. Clinical implications: The greater tubercle of the humerus comes in contact with the acromion during overhead movement of the arm putting pressure on the contents of the subacromial space. These structures within subacromial space are already tightly packed. Inflammation of any of these structures increases the material within the space and causes impingement between adjacent structures. Therefore, the subacromial space is the location of impingement and degenerative pathologies (tendonitis, bursitis...) Bursae: Act to decrease friction during movement between tissues. Subdeltoid and subacromial bursae. Protects and separates the supraspinatus tendon from the acromion, coracoid process, coracoacromial lig. and deltoid muscle. Osteokinematics: Osteokinematics of Scapulothoracic Articulation Elevation & Depression: superior and inferior motion of scapula in the frontal plane Abduction (Protraction) & Adduction (Retraction): motion of scapula in the frontal plane away from or toward the vertebral midline Upward/Downward Rotation in the frontal plane: o Upward - movement of inf. angle of scapula away from vertebral column - tilts glenoid upward. o Downward - movement of inf. angle of scapula toward vertebral column - tilts glenoid downward. (Additional scapular movements: see AC osteokinematics) Osteokinematics of AC Joint ASSOCIATE THESE WITH ACCOMPANYING SCAPULAR AND GLENOHUMERAL MOVEMENTS Amount of motion available at this joint is small BUT IMPORTANT. The Motions are described as Scapular Tipping (sagittal plane) and Scapular Rotation (horizontal plane). Page 2 Scapular tipping - when the scapula elevates and depresses, it also tilts/tips in the sagittal plane Anterior Tipping - the inferior angle moves posteriorly while the superior angle moves anteriorly - necessary for scapula to maintain contact with rib cage during scapular elevation and with extremes of GH internal rotation (observe during posterior reach). Posterior tipping - opposite of anterior tipping; accompanies scapular depression and with extremes of GH external rotation. Scapular rotation in horizontal plane - a turning of the scapula in the horizontal plane that is necessary to maintain contact of scapula with the curvature of rib cage as the scapula slides around the thorax in protraction & retraction. For example – observe the movement of the vertebral border during scapular Abd/Add and during GH Horiz Abd/Add. Osteokinematics of SC joint ASSOCIATE THESE MOVEMENTS WITH ACCOMPANYING SCAPULAR MOVEMENTS Elevation / Depression of clavicle (lateral end) o Always accompanied by scapular elevation / depression o Elevation 3X greater than Depression (~45°/15°) Protraction/Retraction o Ant / post movement of lateral end of clavicle; always accompanied by scapular protraction / retraction. o ROM 15-30° each way Anterior & Posterior Rotation o Technically only Posterior Rotation is available. Total ROM 20-35° Occurs with elevation of the clavicle during overhead movement of arm; caused by tightening of Coracoclavicular ligaments. Osteokinematics of Glenohumeral Joint - 3 degrees of freedom Flexion and Extension (sagittal) Abduction and Adduction (frontal) Medial and Lateral Rotation (transverse) Horizontal Abduction and Horizontal Adduction (transverse) Scaption – abduction in the plane of the scapula Arthrokinematics (roll, slide, spin, convex/concave) Arthrokinematics of A-C Joint: not covering this b/c joint is a plane jt Arthrokinematics of SC joint Application of Convex-Concave Rule describes the following: Elevation/depression: Clavicle is a moving convex surface sliding in the opposite direction as the scapular motion. What sliding motion of the clavicle would you induce to improve elevation of the clavicle? Protraction/retraction: Clavicle is a moving concave surface sliding in the same direction as the scapular motion. What sliding motion of the clavicle would you induce to improve retraction of the clavicle? Rotation: accompanies elevation; not described relative to the Convex-Concave Rule Arthrokinematics of Glenohumeral Joint Application of Convex-Concave Rule describes the following: Humeral head is a moving convex surface sliding in the opposite direction as the distal humerus. o What sliding motion of the humeral head would you induce to improve scaption/abduction of the joint? o What sliding motion of the humeral head would you induce to improve external rotation of the joint? Page 3 Integrated Joint Function in the Shoulder Girdle All joints and muscles of the shoulder girdle complex function together to produce maximum range of movement of the UE, yet also ensure joint stability (esp. at GH joint). Goniometry implications: o AC, SC, & Scap motion is included with AROM measures (flex, ext, abd, IR/ER). o What can AC, SC & Scapular motion do for these GH movements? You may have a need to isolate GH motion for measuring extension, IR/ER rotation, etc.. Why? How? Stability of Glenohumeral joint o Static (arm resting at side, unsupported) Intra-articular pressure - negative intra-articular pressure contributes to stability Superior joint capsule Coracohumeral lig Passive tension/tone in the resting supraspinatus & upper traps muscles o Dynamic (during movement) Rotator cuff muscles (S.I.T.S.) – they are GH joint compressors; keep the humeral head stable and in the appropriate place during movement of the arm. The cuff also has to pull the humeral head down during overhead movement (discussed in Force Couple section below). Force Couples - two or more ms. simultaneously act on a bone in different directions but the resulting torques (at the joint) act in the same rotary direction. Deltoid/rotator cuff - Force couple for abduction; must have a combined movement of upward rolling & downward sliding of the humeral head. If this downward sliding did not occur, the humeral head would be stopped by the acromial arch. Serratus anterior/ Upper & Lower trapezius - for upward scapular rotation, which is necessary to achieve full range of arm abduction/scaptoion by allowing the glenoid fossa to tilt upward. Rhomboids and Pect Minor: Combined Scapulohumeral Motion • We’ll use example of abduction to describe how joints work together (scapulohumeral motion) to produce total motion of the shoulder girdle. o o o o 0- 30° Abd: almost exclusively GH motion - - 25 to 30° ; maybe some minimal scapular mvmt. 30° - 90° Abd: scapular upward rotation & clavicular elevation combines with GH motion to produce the next 60° of abduction; the scapula/clavicle contributes ~30° and the GH joint contributes ~30°. A 1:1 ratio. o When doing abduction or scaption, external rotation of humerus naturally, voluntarily occurs during this phase to clear the greater tubercle from under the acromion. The greater tubercle is moved posteriorly & inferiorly and will not impinge as much on the structures in the subacromial space. 90° - 180° Abd: GH motion again predominates. Scapular rotation during this period is accompanied by posterior rotation of clavicle (clavicle rotation caused by tension in coracoclavicular ligs). The scapula contributes ~30° and the GH joint contributes ~60° to the Abd AROM. This is a 2:1 ratio. Summary: For full abduction of the arm, the ratio of GH contribution to Scapula contribution is 2:1 ratio. GH accounts for ~120°, Scapula/Clavicle accounts for ~60°. Page 4 Patho-Kinesiology: Scapulothoracic: Scapular winging - most often result of nerve injury and paralysis of either the serratus anterior, trapezius, or rhomboid muscles. Scapular dyskinesis Scapular dyskinesis is an abnormal position or motion of the scapula during coupled scapulohumeral movements (esp. flexion and scaption). It occurs in relation to problems involving the GH joint. The specific problem is inhibition or disorganization of activation patterns of scapular stabilizing muscles. Clavicle fx: more prevalent than SC joint sprains; mid-shaft fx is common, usually from lateral force. Medial cord and ulnar nerve compression is a risk from mid-shaft fx. AC Joint sprain: The joint configuration, along with tendency of clavicle to ride higher than acromion, favors displacement of the acromion downward and under clavicle. (inferior and medial). “Shoulder separation” Glenohumeral Subacromial Impingement Syndrome Represents a spectrum of pathology ranging from subacromial bursitis to rotator cuff tendinopathy and full-thickness rotator cuff tears. Causes range from postural, to cumulative trauma, to ms weakness, to bony changes. Muscle/tendon strain, -itis, -opathy, & tear: Biceps long head tendon rupture Rotator cuff - traumatic tear vs. degenerative tear Glenohumeral Instability: Dislocation (anterior-inferior) results in hypermobility and dramatically increases risk for recurrent subluxation or dislocation. Global laxity is different than global instability. Glenohumeral Adhesive Capsulitis (Frozen shoulder): inflammation of the synovium (synovitis), loss of the inferior capsular looseness, a thickened and fibrotic capsuloligamentous complex, capsular adhesions to the humeral head, decreased synovial fluid, subacromial bursal adhesions and musculotendinous contracture. Glenohumeral Labrum injury: tears on the top part are known as Superior Labral Anterior Posterior (SLAP) lesions. Tears in the front part of the labrum that extend to the bottom are known as Bankart lesions. Require surgical repair. Thoracic Outlet Syndrome A region of the shoulder girdle where the neurovascular bundle leaves the thoracic region and enters the upper extremity. Specifically, the neurovascular bundle is the brachial plexus and subclavian/axillary artery. It is susceptible to compression at 3 locations: Between anterior and middle scalenes Under the clavicle (posture) Under Pectoralis Minor at coracoid process attachment (posture/flexibility) Page 5 MUSCULATURE MUSCLE Upper Trapezius Middle Trapezius Lower Trapezius Levator scapulae Rhomboideus major Rhomboideus minor Serratus Anterior Pectoralis minor Anterior Deltoid Middle Deltoid Posterior Deltoid Supraspinatus Pectoralis major Latissimus dorsi Teres major Infraspinatus Teres minor Subscapularis Coracobrachialis Biceps (long head) Triceps (long head) CONCENTRIC ACTION (from neutral position) Elevates and upwardly rotates scapula Adducts scapula Depresses and upwardly rotates scapula Elevates and downwardly rotates scapula Adducts and downwardly rotates scapula Adducts and downwardly rotates scapula Abducts and upwardly rotates scapula Depresses and downwardly rotates scapula Flexes, medially rotates and horizontally adducts humerus Abducts humerus Extends, laterally rotates and horizontally abducts humerus Abducts and externally rotates humerus Adducts, flexes, horizont. adducts & medial rotates humerus Adducts, extends & medially rotates humerus Adducts, extends & medially rotates humerus Laterally rotates humerus Laterally rotates humerus Medially rotates humerus Flexes and adducts humerus Flexes humerus (synergist) Extends humerus PRIME MOVERS OF THE SCAPULA (Summary of Muscle Action- concentric contraction) MOVEMENT MUSCLES Elevation Depression Adduction Abduction Upward Rotation Downward Rotation Upper Trapezius, Levator Scapulae Lower Trapezius, Pectoralis Minor Middle Trapezius, Rhomboids (L. Trap some) Serratus Anterior Upper & Lower Trapezii, Serratus Anterior Rhomboids, Pectoralis Minor, Levator Scapulae PRIME MOVERS OF THE HUMERUS (Summary of Muscle Action - concentric contraction) MOVEMENT MUSCLES Flexion Extension Abduction Adduction External Rotation Internal Rotation Horizontal Abduction Horizontal Adduction Anterior Deltoid, Pectoralis Major, Coracobrachialis, Biceps long head Posterior Deltoid, Latissimus Dorsi, Teres Major, Triceps long head Middle Deltoid, Supraspinatus Pectoralis Major, Latissimus Dorsi, Teres Major, Coracobrachialis Infraspinatus, Teres Minor, Supraspinatus, Posterior Deltoid Subscapularis, Pectoralis Major, Anterior Deltoid, Latissimus Dorsi, Teres Major Posterior Deltoid, Infraspinatus, Teres Minor Pectoralis Major, Anterior Deltoid Remember the stabilizing role of scapular muscles Page 6 Movement Analysis: Describe the scapular, glenohumeral, AND elbow joint movements (osteokinematics only; not arthrokinematics). Describe the muscles contracting during the performance of the activity. Be sure to describe the joint and muscle activity occurring during both parts/phases of the exercise (such as the up and down phase of a pushup). Describe the muscle contractions as either isometric, concentric, or eccentric; differentiate between prime movers and synergists Starting position: Up Phase: Down Phase: Synergists: Starting position: Up Phase: Down Phase: Synergists: Starting position: Up Phase: Down Phase: Synergists: Starting position: Up Phase: Down Phase: Synergists: Page 7 Starting position: Up Phase: Down Phase: Synergists: Starting position: Up Phase: Down Phase: Synergists: Starting position: Up Phase: Down Phase: Synergists: Starting position: Up Phase: Down Phase: Synergists: Starting position: Up Phase: Down Phase: Synergists: Page 8