Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
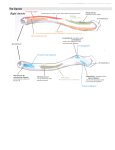
Page 1 of 3 Anatomy Case report Analysis of bony bridge over bicipital groove Abstract Introduction Bicipital groove or intertubercular sulcus is bounded by lesser tubercle medially and greater tubercle laterally. The contents of this groove are long head of biceps brachii, synovial sheath and ascending branch of anterior circumflex humeral artery. The groove is bridged by transverse humeral ligament. This ligament has been found to be ossified. This osseous tissue may damage the contents of bicipital groove during biomechanical movements of the arm. The ossification of this ligament is a new discovery known to the author and bears clinical implications. Hence the study has been carried out. Case report During examination of bones in the osteology lab in the Department of Anatomy, we came across a rightsided humerus showing complete ossification of the transverse humeral ligament. The incidence is 1%. This osseous bridge extended from the lateral margin of the lesser tubercle to the medial margin of the greater tubercle. The horizontal, vertical lengths and thickness of the ossified ligament were 7, 5 and 2 mm, respectively. Discussion The ossified ligament may cause tendinitis of the long head of biceps brachii leading to anterior shoulder pain. It may also cause tenosynovities. Conclusion Knowledge of the ossified transverse humeral ligament may be of immense * Corresponding author Email: [email protected] Department of Anatomy, AIIMS, Virbhadra Marg, Pashulok, Rishikesh, Uttrakhand, India use to clinicians for anterior shoulder pain. It may also cause misinterpretation of radiographs. Introduction The proximal part of the humerus consists of head, greater tubercle, lesser tubercle and bicipital groove. The head is medially directed, greater tubercle is situated on the lateral aspect and lesser tubercle on the anterior aspect of the proximal part of the humerus. Bicipital groove lies between the lesser and the greater tubercles. This groove is bridged by the transverse humeral ligament as described in the standard text books of anatomy but the existence of this ligament has been doubted by MacDonald et al.1 and Gleason et al.2 and replaced by muscle fibres. The groove is occupied by a long head of biceps tendon surrounded by synovial sheath and ascending branch of the anterior circumflex humeral artery. A bony bridge has been observed over the bicipital groove in a humerus. The complete ossification of the transverse humeral ligament or muscle fibres is being reported for the first time. Therefore, it amounts to new variants. This osseous bridge may cause tenosynovitis and tendinitis leading to anterior shoulder pain and may complicate other surgical interventions around this region. Thus, knowledge of this variant may be of utmost use to orthopaedic surgeons, physicians, radiologists and anatomists. This paper analyses the bony bridge over the bicipital groove. Case report During examination of bones in the osteology lab of the Department of Anatomy, a right-sided humerus was found showing complete ossification of the transverse humeral ligament or muscle fibres of the muscles (Figure 1) situated in the vicinity of this bridge. The length, breadth and thickness of the osseous tissue were taken with Figure 1: Ossified transverse humeral ligament in antero-superior view of upper end humerus. Probe is in the canal formed by this ossified ligament. Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY) For citation purposes: Singh R. Analysis of bony bridge over bicipital groove. OA Case Reports 2013 Oct 21;2(13):124. Competing interests: none declared. Conflict of interests: none declared. All authors contributed to the conception, design, and preparation of the manuscript, as well as read and approved the final manuscript. All authors abide by the Association for Medical Ethics (AME) ethical rules of disclosure. R Singh* Page 2 of 3 digital vernier calipers. The photographs were taken, and clinical implications and causes of ossification were analysed. The bridge extended from the lateral margin of the lesser tubercle to the medial margin of the greater tubercle. The horizontal, vertical lengths and thickness of ossified ligament/fibres were 7, 5 and 2 mm, respectively. The incidence of this bony bridge formation over bicipital groove was 1%. There was no other abnormality in the humerus. Discussion The bicipital groove is bridged by the transverse humeral ligament or muscle fibres of subscapularis and supraspinatus muscles and pectoralis major muscle. MacDonald et al.1 observed that what is defined as transverse humeral ligament is not ligament as described in standard text books rather this is a fibrous expansion arising from the posterior lamina of the tendon of pectoralis major overlying the long tendon of biceps in every shoulder of all the 85 shoulders. In 86% of shoulders, fibres from the tendon of subscapularis passed over the long tendon of biceps within this fibrous expansion and inserted on to the greater tubercle of the humerus. According to Gleason et al.2, there is no identifiable transverse humeral ligament, rather the fibres covering the intertubercular groove are composed of a sling formed mainly by the fibres of the subscapularis tendon, with contributions from the supraspinatus tendon and the coracohumeral ligament. Gleason et al.2 confirmed these gross dissection patterns of fibre attachment through histological studies. This revealed the absence of elastin fibres, which are more commonly seen in ligamentous structures and are typically absent from tendinous structures. These studies reveal that the bridging seen over bicipital groove cover the muscle fibres rather than ligament. Causes of formation of bony bridge As the bony bridge was detected in one right-sided humerus out of 100 humeri examined, it is pertinent here to analyse the causes of this bony structure. Partial or complete calcification and ossification of superior transverse scapular ligament3 and transverse acetabular ligament4 have been documented. Standard text books do not describe the ossification of transverse humeral ligament/ muscle fibres and no literature is available on the theory of causes of osseous bridging over bicipital groove. In such a situation, the author attempted to formulate a logical basis for ossification of the tissues bridging the bicipital groove. One of the possibilities of calcification may be calcium metabolism disorder in such persons. Cohen et al.5 described a familial case of calcification of superior transverse scapular ligament affecting a 58-yearold man and his son who had calcification of superior transverse scapular ligament causing entrapment neuropathy of the suprascapular nerve and its attendant clinical symptoms of pain, weakness, atrophy of the supraspinatus muscle. Similarly, calcification and ossification of transverse humeral ligament/muscle fibres may be due to genetic reasons which are to be confirmed by further clinical studies. Formation of bony bridge over the bicipital groove may also be caused by repetitive strain on the subscapularis, supraspinatus muscles and pectoralis major muscle resulting in microtrauma during biomechanical movements of the shoulder and ultimately leading to calcification and ossification of these fibres. Clinical significance It was observed in 1% of subject population. These muscle fibres prevent subluxation of tendons of the long head of biceps during biomechanical movements of the arm ensuring soft stability of the tendon. In movements from external rotation to internal rotation, the tendon is forced medially against lesser tubercle and superiorly against transverse humeral ligament6 during biomechanical movements of the arm, the long tendon of biceps rub against the overlying muscle fibres. As muscle fibres are soft tissues these structures do not damage the tendon during biomechanical movements of the arm. But when these muscle fibres are ossified, the tendon of biceps brachii constantly rub against the bony bridge during movements like repetitive lifting of weight, stretching of arm vertically during exercise, various multidirectional movements in wrestling and in picking up objects from higher places by lifting the arm. This rubbing may lead to inflammation, microtearing and if untreated, it will cause degenerative changes in the tendon of the biceps. An inflamed tendon may lead to anterior shoulder pain. Frequent or repetitive lifting, in case of chronically inflamed tendon of biceps brachii, can lead to spontaneous rupture. The patient complaining of anterior shoulder pain aggravated by lifting activities like carrying objects, shopping bags and reaching overhead objects may invite attention of the clinician towards the above complications. Thus anterior shoulder pain may be caused by bony bridge. A dramatic worsening of symptoms and description of a lump just above the antecubital fossa suggests an acute long head tendon rupture. It may also cause thrombosis of the ascending branch of the anterior circumflex humeral artery running in the bicipital groove creating ischaemia in the structures supplied by this artery. Bicipital groove is often used as an important landmark for proper orientation of humeral prosthesis, especially in the case of a fracture7. The bicipital groove is also used as an anatomic landmark to restore Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY) For citation purposes: Singh R. Analysis of bony bridge over bicipital groove. OA Case Reports 2013 Oct 21;2(13):124. Competing interests: none declared. Conflict of interests: none declared. All authors contributed to the conception, design, and preparation of the manuscript, as well as read and approved the final manuscript. All authors abide by the Association for Medical Ethics (AME) ethical rules of disclosure. Case report Page 3 of 3 humeral head retroversion when treating complex proximal humeral fractures with arthroplasty8. The bicipital groove offers a useful landmark for placement of lateral fin of the prosthesis9. In the presence of ossified transverse humeral ligament/muscle fibres, this groove may not act as a useful landmark for the above procedures. The ossified fibres may cause misinterpretation of radiographs. Thus knowledge of ossification of transverse humeral ligament/muscle fibres may be of paramount importance to physicians for anterior shoulder pain, orthopaedic surgeons for deciding bicipital groove as landmarks in different types of shoulder surgery, radiologists for avoiding misinterpretation of radiographs and anatomists for new variants. Conclusion • Osseous bridge over bicipital groove may be formed by ossification/calcification of transverse humeral ligament/ muscle fibres. • The ossified bridge may cause anterior shoulder pain. • The ossified bridge may obscure the radiological image of the bicipital groove. • Due to presence of the osseous bridge, the bicipital groove may not act as a landmark to locate the position of surgical procedures in and around the bicipital groove. References 1. MacDonald K, Bridger J, Cash C, Parkin I. Transverse humeral ligament: does it exist? Clin Anat. 2007 Aug;20(6): 663–7. 2. Gleason PD, Beall DP, Sanders TG, Bond JL, Ly JQ, Holland LL, et al. The transverse humeral ligament: a separate anatomical structure or a continuation of the osseous attachment of the rotator cuff? Am J Sports Med. 2006 Jan;34(1):72–7. 3. Ticker JB, Diurasovi CM, Strauch RJ, April EW, Pollock RG, Flatow EL, et al. The incidence of ganglion cysts and other variations in anatomy along the course of the suprascapular nerve. J Shoulder Elbow Surg. 1998 Sep–Oct; 7(5):472–8. 4. Bhanu Sharmila P, Shankar KD. Bilateral ankylosis of sacroiliac joint with ossification of sacrospinous, sacrotuberous and transverse acetabular ligaments. IJAV. 2011 Jan;4:123–7. 5. Cohen SB, Dnes DM, Moorman CT. Familial calcification of the superior transverse scapular ligament causing neuropathy. Clin Orthop Rel Res. 1997 Jan;334:131–5. 6. Standring S, editor. Grays anatomy: the anatomical basis of clinical Practice. 39th ed. Spain: Churchil Livingstone; 2006. p823–32. 7. Kontakis GM1, Damilakis J, Christoforakis J, Papadakis A, Katonis P, Prassopoulos P. The bicipital groove as a landmark for orientation of the humeral prosthesis in cases of fracture. J Shoulder Elbow Surg. 2001 Mar–Apr;10(2):136–9. 8. Anqibband L, Zuckerman JD, Flurin PH, Roche C, Wright T. Reconstructing proximal humeral fractures using the bicipital groove as a landmark. Clin Orthop Relat Res. 2007 May;458:168–74. 9. Itamura J, Dietrick T, Roidis N, Shean C, Chen F, Tibone J. Analysis of the bicipital groove for humeral head replacement. J Shoulder Elbow Surg. 2002 Jul–Aug; 11(4):322–6. Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY) For citation purposes: Singh R. Analysis of bony bridge over bicipital groove. OA Case Reports 2013 Oct 21;2(13):124. Competing interests: none declared. Conflict of interests: none declared. All authors contributed to the conception, design, and preparation of the manuscript, as well as read and approved the final manuscript. All authors abide by the Association for Medical Ethics (AME) ethical rules of disclosure. Case report