Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
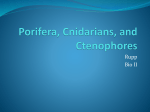
Turkish Journal of Endocrinology and Metabolism, (2005) 2 : 45-47 ORIGINAL ARTICLE Association Between Skin Tags and Colonic Polyps in Patients with Acromegaly Neslihan Kurtulmuş* Sema Yarman** Kadir Demir*** Fırat * Educational and Research Hospital of Vakıf Gureba, Endocrinology Unit, İstanbul ** İstanbul University, Istanbul Medical Faculty, Division of Endocrinology, Metabolism and Nutrition, İstanbul *** İstanbul University, Istanbul Medical Faculty, Division of Gastroenterohepatology, İstanbul The high prevalence of colonic polyps in acromegalic patients is well known. Colonic adenomatous polyps may be precursor lesions for colorectal carcinoma. Skin tags are generally benign skin growths, but it has been reported that there is a correlation between skin tags and colonic polyposis in acromeglic patients. We evaluated association between colonic polyps and skin tags in twenty-five acromegalic patients. The aged over 70, previous colonic disease or polyps, rectal bleeding, positive family history for colon disease and smoking were exclusion criterians in the study. Colonoscopy was performed in all patients and colonic polyps were found in ten of them. Skin tags were detected in eight of ten patients with colonic polyps. The specificity and sensitivity of the presence of polyps with skin tags was high However Fisher’s exact test was not statistically significant. As a conclusion, colonoscopy should be performed in all acromegalic patients especially in those with skin tags. Key words: Acromegaly, colon polyps, skin tag Introduction Acromegaly is a rare disease characterized by enlargements of the acral parts and visceromegaly. Overproduction of growth hormone from a tumour of anterior pituitary gland causes acromegaly (1). Several studies reported an increased prevalence of colonic polyps in acromegalic patients and these patients are known to have an increased prevalence of colorectal carcinoma (2-5). However, risk factors of colonic polyps and colorectal carcinoma in acromegalic patients are still uncertain. Several risk factors are male gender, long duration of disease, high level of insulin-like growth factor, family history of colon cancer, age greater than 50 years, and skin tags (2,6). Skin tags, also known as achrochordon are very common, and are generally benign skin growths. Usually, they are very small, but sometimes are half an inch long and they are Correspondence address: Neslihan Kurtulmuş Vakıf Gureba Hastanesi , Fatih-İSTANBUL Phone : 0 212 534 69 00-1063 Fax : 0 212 311 23 67 located on the neck, armpits, trunk, body folds, or other areas (7). Their origin is unknown. Diagnosis is based primarily on the appearance of the skin growth (7). An association between high number of skin tags (more than three) and colonic polyps in acromegalic patients has been reported (8,9). In this study, we evaluated the association between colonic polyps and skin tags in patients with acromegaly on admission. Subjects and Methods Twenty-five acromegalic patients 14 men and 11 women aged 25 to 70 years (mean, 45.6 ± 11 years), were evaluated for the relation between colonic polyps and skin tags. None of patients had any risk factors for colonic polyps and colorectal cancer such as familial polyposis syndromes, a family history of hereditery colon cancer, a history of inflamatory bowel disease and smoking. We didn’t include patients which has any risc factors for colon polips. Twenty-three patients had active disease. Two patients were in remission. The diagnosis of acromegaly was established by clinical findings and then confirmed by the findings of elevated plasma concentrations of growth hormone (GH) that were not suppressed below 2 ng/ml (by 45 ORIGINAL ARTICLE RIA) after administration of an oral glucose load (100mg) and high serum insulin-like growth factor I (IGF-I) levels and radiological demonstration of a pituitary adenoma. After bowel preparation, total colonoscopy was performed with a fiberoptic colonoscope by an experienced endoscopist in the department of gastroenterology. Colonic polyps were removed endoscopically and examined histologically. Before colonoscopy, each patient was examined spesifically to determine the presence of skin tags (Figure 1). The location and number of skin tags were noted. located on the neck, near the axilla or upper trunk. Because of diagnosis is based primarily on the appearance of the skin growth and they were thought to be simple skin tags, we did not examine these lesions histologically. Skin tags were also present along with colon polyps in 8 of 10 patients. The positivity ratio, false positivity ratio, the sensivity (presence of both skin tag and colon polips), and the specifity (absence of both skin tags and colon polips) were 80%, 47%, 53%, 80% respectively. This result seems to be meaningful. Odds ratio was 4.57 and it showed that patients with skin tags had high risk for colon polyps. However Fischer’s exact test was not stutistically significant. Figure 1. Statistical analysis Figure 2. The degree of association between skin tags and the presence of colonic polyps in acromegalic patients was estimated by the odds ratio, the strength of the association was calculated using the Fisher’s exact test. The specificity (the probability of the presence of skin tags conditional on the presence of colonic polyps) and sensitivity (the probability of the absence of polyps given the presence of skin tags) were evaluated. Results Colonoscopic examination was complete to the cecum in twenty-two patients (%88). All of the patients had dolichomegacolon. Ten of the twentyfive acromegalic patients (%40) had colonic polyps (Figure 2). These polyps were underwent polypectomy. Histologically, seven patients had adenomatous polyps and three patients had hyperplastic polyps. None of the patients had colorectal carcinoma. In skin examination, fifteen of the patients (%60) had simple skin tags. In these patients, the skin tags were most commonly 46 Discussion Acromegaly is associated with an increased prevalence of neoplastic disorders (10). The results of several studies indicate that the frequency of colorectal cancer increased in patients with acromegaly (4,6,10). Adenomatous polyps are the precursor lesions of colonic cancer (2). The removal of adenomatous polyp before it becomes malignant will be benefical for the actual prevention of colonic cancer (10). Skin tags are usually benign and the prevalence of these lesions increase in elderly patients (7). An association between skin tags and colonic polyps in acromegalic patients has also been reported (8,9,11). Thus, skin tag may be a marker for the colonic polyps in patients with acromegaly. Leavit et al. demonstrated a relation between the skin tag and the precence of colonic polyp in male patients (8). In this study, they found that the sensitivity for skin tags in identifying patients at risk for colonic polyps is 80.4% and the ORIGINAL ARTICLE spesificity is 77.1%. In another study, Bhansali et al. showed that the number of skin tags was significantly higher in the group of acromegalic patients with colon polyps. The study of Beitler et al. showed high insidence of colonic polyps in patients with skin tag (11). Our study shows that real positivity ratio is high and specifity ratio is %80. We couldn’t verify this result at the Fischer’s exact test because number of patients were insufficent. Insufficiency generated from the strict criteria applied in choosing the patients. In conclusion, acromegalic patients with skin tags have an increased risk of developing colonic polyps. If we consider potential cancer risk of the polyp, removal of the polyp will reduce the risk of malignancy. As a result of our study we conclude that colonoscopy should be performed in all acromegalic patients especially in those with skin tags. 4. Vasen HF, van Epercum KJ, Roelfsma F, Raue F, Koppeschaar H, Griffioen G, van Berge Henegouwen GP. Increased prevalence of colonic adenoma in patients with acromegaly. Eur J Endocrinol. 131:235-237, 1994. 5. Martino A, Cammarota G, Cianci R, Bianchi A, Sacco E, Tilaro L, Marzetti E, Certo M, Pirozzi G, Fedeli P, Pandolfi P, Pontecorvi A, Gasparrini G, De Marinis L. High prevalence of hyperplastic colonic polyps in acromegalic subjects. Dig Dis Sci. 49:662-666, 2004. 6. Terzolo M, Tappero G, Borretta G, Asnaghi G, Pia A, Reimondo G, Boccizzi A, Cesario F, Rovero E, Paccotti P et al. High prevalence of colonic polyps in patients with acromegaly. Influence of sex and age. Arch Intern Med; 154:1272-1276,1994. 7. Lookingbill DP, Marks JG, editors. Epidermal Growths. In: Principles of Dermatology third Edition. Philadelphia: WB Saunders Company, 2000, 74-77. 8. Leavitt J, Klein I, Kendriks F, Gavaler J, Van Thiel D. Skin Tags: A cutaneous marker for colonic polyps. Ann Intern Med. 98: 928-930, 1983. 9. Bhansali A, Kochhar R, Chawla YK, Reddy S, Dash RJ. References 1. Baumann G. Growth hormone and its disorders. In: Kenneth L. Becker, ed. Principles and Practice of Endocrinology and Metabolism, edited by Kenneth L. Becker, Philadelphia: Lippincott Williams and Wilkins, 2001, 141-145. 2. Ezzat S, Strom C, Melmed S. Colon polyps in acromegaly. Ann Intern Med. 114: 754-755, 1991. 3. Ron E, Gridley G, Hrubec Z, Page W, Arora S, Fraumeni Jr JF. Acromegaly and gastrointestinal cancer. Cancer. 68: 1673-1677, 1991. Prevalence of colonic polyps is not increased in patients with acromegaly: analysis of 60 patients from India. Gastroenterol Hepatol. 19: 266-269, 2004. 10. Delhougne B, Deneux C, Abs R, Chanson P, Fierens H, Laurent-Puig P, Duysburg I, Stevenaert A, Tabarin A, Delwaide J, Schaison G, Belaiche J, Beckers A. The prevalence of colonic polyps in acromegaly: A colonoscopic and pathological study in 103 patients. J Clin Endocrinol Metab 80: 3223-3226, 1995. 11. Beitler M,Eng A,Kilgour M,Lebwohl M.Association between acrochordons and colonic polyps. J Am Acad Dermatol. 14:1042-1044, 1986. 47