Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Retrograde amnesia wikipedia , lookup
Generalized anxiety disorder wikipedia , lookup
Factitious disorder imposed on another wikipedia , lookup
Wernicke–Korsakoff syndrome wikipedia , lookup
Conversion disorder wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
Munchausen by Internet wikipedia , lookup
Externalizing disorders wikipedia , lookup
History of mental disorders wikipedia , lookup
Dissociative identity disorder wikipedia , lookup
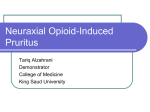
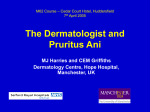
ArchivEuromedica 1st & 2nd Edition 2011 screening for congenital hypothyroidism: how much and at what level? Arch Dis Child. 2011 Apr;96(4):374-9. 5. Demartini B, Masu A, Scarone S, Pontiroli AE, Gambini O. Prevalence of depression in patients affected by subclinical hypothyroidism. Panminerva Med. 2010 Dec;52(4):277-82. 6. Duntas LH, Biondi B. New insights into subclinical hypothyroidism and cardiovascular risk. Semin Thromb Hemost. 2011 Feb;37(1):27-34. 7. Hercbergs AH, Ashur-Fabian O, Garfield D. Thyroid hormones and cancer: clinical studies of hypothyroidism in oncology. Curr Opin Endocrinol Diabetes Obes. 2010 Oct;17(5):432-6. 8. Krassas GE, Poppe K, Glinoer D. Thyroid function and human reproductive health. Endocr Rev. 2010 Oct;31(5):702-55. 9. Atis G, Dalkilinc A, Altuntas Y, Atis A, Caskurlu T, Ergenekon E. Sexual dysfunction in women with clinical hypothyroidism and subclinical hypothyroidism. J Sex Med. 2010 Jul;7(7):2583-90. 10. Kvetny J, Wilms L, Pedersen PL, Larsen J. Subclinical hypothyroidism affects mitochondrial function. Horm Metab Res. 2010 May;42(5):324-7. 11. Todd CH. Management of thyroid disorders in primary care: challenges and controversies. Postgrad Med J. 2009 Dec;85(1010):655-9. 12. Chen HP, He JS, Hu GS. [Analysis on the traditional Chinese medicine syndromes of the patients with autoimmune thyroid diseases. Changes in the thyroid and immune functions in 109 cases] // Zhong Xi Yi Jie He Za Zhi. 1990 Sep;10(9):538-9, 517. 13. Silva JE, Bianco SD. Thyroid-adrenergic interactions: physiological and clinical implications. Thyroid. 2008 Feb;18(2):157-65. 14. Vasilenko A., Luzina- J-L, Sokolova T. Modern NeuroEndocrinImmunological Conception of Acupuntcture International Council of Medical Acupuncture and Related Techniques (ICMART) May, 2005. Psychogenic, somatoform and functional itch: heterogeneity or overlap of the phenomenon? Andrey Lvov, Dmitry Romanov, Svetlana Bobko Introduction Itch or pruritus is one of the most common symptoms in dermatology. About 35% outpatients of the dermatological clinic suffer from itch (Alexander H., 2005). In general population it occurs within prevalence from 8.8% to 13.9% (Wolkenstein P., 2003, Dalgard F., 2005, Halvorsen J.A., 2009). Itch accompanies skin diseases (atopic dermatitis and urticaria) in 100% of cases (Weisshaar E. et al., 2009), psoriasis in 87% of cases (Yosipovich G., 2000; Krueger G., 2001), herpetic infection in 58% cases (Oaklander A.L. et al., 2003) as well as systemic diseases (chronic renal or liver failure, lymphoproliferative diseases, oncological process) and psychiatric disorders. Itch unexplained by any dermatological or somatic cause is considered as psychogenic or functional and equivalent to somatoform one (Harth W. et al., 2006; Misery L., Alexandre S., 2007). Somatoform pruritus is usually attributed to undifferentiated somatoform disorder (DSM-IV-TR; 300.81), that could include not just «sine materia» symptoms, but also cases when physical complaints are in excess of what would be expected from the existing medical condition, i.e. «cum materia». Psychogenic itch is diagnosed in 6.5 % of outpatients of dermatological clinics (Stangier U., Gieler U., 1997) and implicates relation of pruritus exacerbation with psychosocial stress exposure. Objective of the study was to evaluate complex clinical structure of somatoform itch in order to distinguish its psychosomatic variants. Methods. Psychopathological and dermatological observation by 100 Dr. Svetlana Bobko M.D., dermatovenerologist, Ph.D.-student of dermatological department of I.M. Sechenov Moscow State Medical University, studied in clinic for Dermatology and Allergology Philipps-University in Marburg in 2007-2008. PhD thesis Theme”Psychogenic itch: aspects of clinical systematics, complex therapy and prophylaxis” under supervision of professor of dermatological department A.N. Lvov in collaboration with research worker of department for psychiatry and psychosomatics, psychiatrist Phd Romanov D.V.), the co-author of 22 research papers and repeated laureate of competitions for best scientific work among young scientists, was awarded with the medal of the Russian Academy of Medical Scientists for the best scientific work in 2008, member of Moscow society of dermatovenerologists, european academy of dermatology and venerology and international society of dermatology dermatologist and psychiatrist of 40 patients with itch (24 women, mean age - 34,6±11,3 years) in the dermatologic department. Hospital Anxiety and Depression Scale (HADS) was used to evaluate anxious and depressive symptoms. Results Examined subjects were divided into 2 groups: somatoform itch «sine materia» or functional (n=26) and somatoform itch «cum materia» (amplifying and mimicking existing dermatological diseases). (n=14). In the first group without dermatological diseases subjects itch descriptions varied greatly in quality (burning, tingling, stabbing, biting, crawling), localization (generalized, localized) and intensity (up to itch paroxysms). In the second group (atopic dermatitis in 8 cases - SCORAD = 36,7±11,2; psoriasis in 6 cases - PASI = 16,9±4,8) itch was monomorphous and described as just «sensation causing desire to scratch» or burning. The following registered itch characteristics allowed to attribute this variant of somatoform pruritus to «cum mateI.M. Sechenov Moscow State Medical University (Dermatologic department, Department of psychiatry and psychosomatic disorders) Moscow, Russia ArchivEuromedica 1st & 2nd Edition 2011 istered in about a half of patients in both groups (46,1% and 50% respectively). Patients of both groups also had other somatoform complains according to life history and/or at the time point of examination: pathological sensations and vegetative dysfunctions. The functional non-skin symptoms could be single and recurrent (pseudosomatic episodes) or manifest in a form of cardiac or gastric neurosis, hyperventilation or irritable bowel syndrome. Also patients of the sample reveled a kind of constitutional somatopsychic predisposition (neuropatic constitution) with symptomatic lability and multiple somatosensory disturbances, which could be conFigure 1 and 2. Self induced skin lesions caused by itch of the first group of patients. sidered as a predisposing factor to ria» phenomenon and distinguish from typical dermatologimultiple somatoform complains cal itch and «pure» psychogenic pruritus: 1) itch localization including somatoform pruritus. greatly exceeding the atopic or psoriatic eruptions areas; 2) Discussion. itch emerged as a prodromal symptom of psychogenically provoked relapses of dermatoses with typical eruptions only Somatoform itch is a heterogeneous group that includes in several days; 3) itch persisted after eruptions totally dis- 2 variants: functional and amplified itch [6]. Nevertheless, appeared; 4) there were psychogenically provoked transient diagnose of dermatoses doesn’t exclude the possibility of itch flares on somatoform itch: minimal skin lesions could be accompanied a spare skin in by over-intensive itch in case of psychosomatic disturbances. dermatoses re- Psychogenic itch is provoked by stress and can occur in two variants. On the one hand, it could be told about missions. In spite of the heterogeneity of somatoform itch phenomena, on the other differences ob- hand – about overlap due to psychogenic provocation, served patients general constitutional features and comorbid somatoform with these phenomena. two types of Conclusion. Somatoform itch is a heterogenous phenomenon s o m a t o f o r m developing as in a form of «pure» functional condition («sine itch had much materia»), as in dermatological itching diseases («cum in common. materia»). Described two variants have common psychiatric There was a comorbidity and constitutional predisposition. high level of References. comorbid anx- 1. «Pruritus» (Chapter Psychogenic itch) L. Misery, S. Ständer, Springer, ious symptoms 2010 in both groups 2. «Pruritus» S. Ständer 1. Auflage – Bremen: Uni-Med, 2008 with promi- 3. «Pruritus Diagnostic und Therapie von chronisch-systemischem nent «health Hautjucken». anxiety» (HADS Z. Zylicz, R. Twycross, E. Anthony Jones (Teil Somatoformer pruritus), 2004 anxiety sub4. «Treatment of chronic pruritus with the selective Serotonin Rescale score – uptake Inhibitors Paroxetine and Fluvoxamin. Two-arm Proof-of15,4±3,2), but concept study» S. Ständer, B. Böckenholt, F. Schürmezer-Horst et al. no signs of 2009; 89 (1): 45-51 clinically rel- 5. «Functional Itch Disorders or Psychogenic Pruritus: Suggested evant depres- Diagnosis Criteria from the French Psychodermatology Group» L. sion or other Misery, S. Alexandre «Acta Dermatovenerologica», 2007, V. 87: 341severe psychi- 344. atric disorders. 6. «Clinical pictures and classification of somatoform disorders in dermatology» Harth W., Hermes B., Niemier V., Gieler U. European Ps y c h o g e n i c Journal of Dermatology 2006 Nov-Dec 16 (6) 607-14 exacerbations Figure 3 and 4. Amplified itch in patients with Atopic of functional dermatitis (clinical picture of a patient from second itch were reggroup) 101