Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
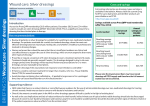
Letter to the editor Acta Dermatovenerol Croat 2012;20(3):197-214 Concurrent Management of Toxic Epidermal Necrolysis with Thermal Water Spray and Non-Stick Dressings Dear Editor, We describe two patients with toxic epidermal necrolysis (TEN) who were successfully managed with Avene thermal spring water spray (ATSW), non-stick dressings and intravenous immunoglobulin (IVIg), without transfer to a burns unit. A 28-year-old Malaysian male with TEN secondary to carbamazepine was treated with i.v. hydrocortisone, IVIg and patient-controlled analgesia. Transfer to a burns unit was considered until learning that debridement, stick-on dressings with mandatory sedation/intubation due to pain was the approach to skin management. To manage his skin whilst conscious and able to sit/stand in the high dependency unit (HDU), we conducted regular fluid release from fresh bullae using sterile needles, leaving the epidermis intact as its own dressing. To cleanse easily we used a Figure 1. Case 1. Erosions, blisters and mucosal involvement 210 spray-on bacteriologically pure thermal spring water spray (ATSW, Avene, France) and non-stick silicone dressings to areas where the skin had sloughed off. The patient was able to self-administer the spray to his skin, mouth and genital areas for comfort, as were his relatives and it was very time-efficient for the nurses compared with opening sterile saline packs. The skin healed without infection or scarring (Figs. 1-4). A 40-year-old Caucasian female with TEN secondary to lamotrigine was commenced on IVIg. Bullae were regularly popped with a sterile needle, denuded areas dressed with non-stick dressings and ATSW to clean her skin. Her skin healed well without scarring and without transfer to a burns unit. Despite the similar clinical presentations of burns and TEN, major differences exist between these two entities (1). TEN affects the superficial layers, originating from the inside and progressing over many days, compared with a thermal burn which is due to a oneoff external trauma, potentially resulting in deeper cutaneous involvement. Immunosuppressive agents can be used in TEN as it is an immune mediated disease, unlike burns. In our experience, burns centers, on the advice of plastic surgeons, treat the skin in TEN patients in the same way as burns patients, with intubation, sedation, debridement of the skin and use of silver coated adhesive dressings. Although silver is typically thought to be safe in burns wounds, its use in TEN is discouraged (2,3). Aggressive treatment such as intubation in patients with mucosal fragility can potentially cause short term and long term complications. In addition, substantial psychosocial support to family members is mandatory if transfer to an intensive care or burns unit ensues (4). Instead, using topical treatments including dressings and sterile water in addition to the dehiscence of blisters can be effective with minimal long term scarring. Thermal spring water, a natural, bacteriologically pure water with low mineral content (5) has been used previously in the management of TEN in conjunction with dressings (6). ATSW is well tolerated and easily applied to mucocutaneous surfaces by nurses, relatives and the patient themselves. It is used as an alternative to showering and bathing and prevents against further sloughing of the skin. Being sterile, non-abra- ACTA DERMATOVENEROLOGICA CROATICA Letter to the editor Acta Dermatovenerol Croat 2012;20(3):197-214 Figure 2. Popping the blisters Figure 3. Case 1. 1 month follow up-chest sive with soothing properties, ATSW can be applied multiple times a day (6) and oral consumption is safe. Based on the treatment of epidermolysis bullosa, our protocol was to pop the blisters with a sterile needle before they were greater than 1 cm in diameter. The blisters were not deroofed as the epidermis acts as its own dressing. Any erosion should be covered with non-stick dressings. Both patients were managed in a ACTA DERMATOVENEROLOGICA CROATICA high dependency setting without transfer to a burns unit and have made good recoveries with no complications. A more conservative approach to managing patients with TEN can result in significant cost savings for hospitals, with less use of interventional and intensive care equipment, and without compromising on patient care. This form of skin care not only saves the cost of ICU/burns units but allowed the patients 211 Letter to the editor Acta Dermatovenerol Croat 2012;20(3):197-214 Figure 4. Case 1. 1 month follow up-back to remain conscious and was easy for the nursing staff to administer. References 1. Wolf R, Davidovici B. Severe cutaneous adverse drug reactions: who should treat, where and how?: Facts and controversies. Clin Dermatol 2010;28:344-8. 2. Frenia ML, Schauben P. Use of silver sulfadiazine in Stevens-Johnson syndrome. Ann Pharmacother 1994;28:736-7. 3. Fuller FW. The side effects of silver sulfadiazine. J Burn Care Res 2009;30:464-70. 4. Makowski SK. Who is at risk for psychological distress? A patient-centered process to identify risk for posttraumatic stress disorder and depression in families of ICU patients. Chest 2011;139:743-4. 5. Merial-Kieny C, Castex-Rizzi N, Selas B, Mery S, Guerrero D. Avene Thermal Spring Water: an active component with specific properties. J Eur Acad Dermatol Venereol 2011;25 Suppl 1:2-5. 212 6. Petkov T, Pehlivanov G, Grozdev I, Kavaklieva S, Tsankov N. Toxic epidermal necrolysis as a dermatological manifestation of drug hypersensitivity syndrome. Eur J Dermatol 2007;17:422-7. Benjamin S. Daniel1,4, George Skowronski2,4, John Myburgh2,4, Mark Hersch3,4, Dedee F. Murrell1,4 Department of Dermatology, St George Hospital, 2Intensive Care Unit, 3Department of Neurology, St George Hospital; 4University of New South Wales, Sydney, NSW, Australia 1 Corresponding author: Professor Dedee F. Murrell Head of Dermatology St George Hospital University of New South Wales School of Medicine Sydney NSW 2217 Australia [email protected] Received: December 27, 2011 Accepted, May 25, 2012 ACTA DERMATOVENEROLOGICA CROATICA