Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
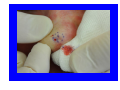
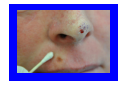
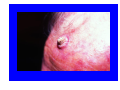
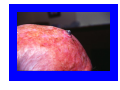
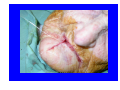
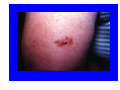
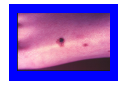
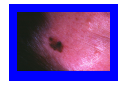
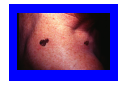
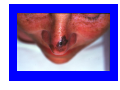
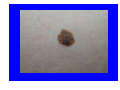
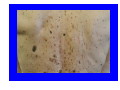
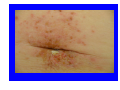
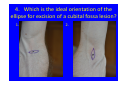
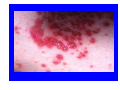
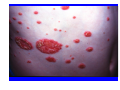
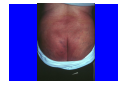
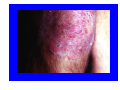
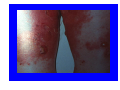
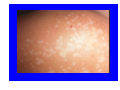
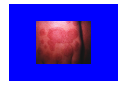
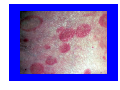
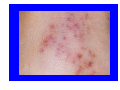
Dermatology: the big picture Dr Philip Clarke Suspicious skin lesions. Diagnosis and treatment. Dr. Philip Clarke Department of Dermatology Launceston General Hospital Is it a presenting problem? • • • • • How long has it been there? Is it changing? Does it bleed? Is it tender? Is the patient concerned? Is it an incidental finding? • Does it look suspicious? • Is the patient aware of it? • Does the patient think it has changed? What is the patient’s risk of skin cancer? • • • • • Personal or family history of skin cancer Past sun exposure Use of a solarium Immunosuppression from illness or medication Organ transplant Types of BCC • Superficial BCC • Morphoeic BCC • Nodular BCC Complications of BCC • • • • Bleeding Locally destructive Ulceration Rarely metastasize Treatment of BCC • Firstly, make sure of the diagnosis. • If the lesion is not to be excised, do a biopsy. • Treatment options: ‐excision ‐liquid nitrogen ‐curettage ‐radiotherapy ‐imiquimod or 5‐fluorouracil ‐photodynamic therapy Danger areas for BCC and SCC • Ears • Nose • Eyes • Scalp Squamous Cell Carcinoma(SCC) • • • • • The second most common of all cancers. Occurs mostly on chronically exposed areas. Mainly the head and hands. Has the potential to metastasize. There is a significant mortality. Subtypes of SCC • SCC. • Keratoacanthoma. • Bowen’s disease(insitu SCC) High‐Risk SCC’s • • • • • Rapidly growing and poorly differentiated. Vascular or perineural invasion. SCC of the ear. SCC of the lip, especially in smokers. SCC of the scalp. High Risk SCC • Patients need regular followup e.g. 3‐6mthly. • Check site and regional nodes. • Look for other skin cancers. Treatment of SCC • Excision. • For metastatic disease;surgery & radiotherapy. • Insitu SCC; ‐excision ‐curettage ‐5‐FU or imiquimod ‐liquid nitrogen 2x30 sec. Melanoma Risk Factors • Sun exposure especially sunburn under 20 years of age. • A large number of moles e.g. over 100. • 6 or more dysplastic naevi. • Family history of melanoma. • Increasing age. Detecting Skin Cancer • Examine the patient in good light. • A small amount of magnification is useful e.g. a binocular loop. • Palpate and slightly stretch any suspicious lesion. What to do next • If a lesion is highly suspicious,excise it or get someone else to cut it out. • If there is some suspicion,measure the lesion and review in 8 weeks. • If the patient is persistently concerned,excise the lesion. Treatment of a Suspicious Lesion • Excise the lesion with a 2mm margin. • Wider excision may be performed in the next few weeks if required. • Do not perform punch or shave biopsies on suspicious pigmented lesions. • Do not freeze pigmented lesions. Characteristics of a Melanoma • • • • • • Irregular border. Irregular colour. Irregular surface. Beware of a changing lesion. Beware of a new lesion. Be very aware of a rapidly growing red raised lesion. Treatment of Melanoma • • • • • melanoma in situ: margin 5mm melanoma < 1.0mm: margin 1cm melanoma 1.0–2.0mm: margin 1–2cm melanoma 2.0–4.0mm: margin 1–2cm melanoma > 4.0mm: margin 2cm Treatment of Melanoma • Regular followup e.g. every 3‐12 months. • Check for metastatic disease and for other primary skin cancers. • There is no place for routine scans. Only perform these if there are clinical suspicions of metastatic disease. Prognosis for Melanoma • • • • Average of 90% five year survival. 99% for insitu melanoma. 40% for a lesion >4mm depth. Worse prognosis with: ‐increasing depth. ‐increasing age. ‐ulceration. ‐mitoses. ‐lesions on the head or neck. Skin Cancer Quiz Dermatology: the big picture GP13 – October 2013 1. The best treatment option for most skin cancers is: 1. Curettage 2. Liquid nitrogen 3. Excision 4. Imiquimod or fluorouracil 2. The recommended excision margin for most BCC’s is: 1. 2. 3. 4. 1mm 2‐3mm 5mm 10mm 3. The recommended excision margin for melanoma less than 1mm depth is: 1. 2. 3. 4. 5. 1mm 2‐3mm 5mm 10mm 50mm(5cm) 4. Which is the ideal orientation of the ellipse for excision of a cubital fossa lesion? 1. 2. 5. A patient presents for the second time in 2 months concerned about a particular lesion. It looks most like a seborrhoeic keratosis. What should you do? 1. Reassure the patient that it is benign and may be left alone. 2. Freeze it off. 3. Biopsy the lesion. What rash is that? Diagnosing and treating rashes Dr. Philip Clarke Department of Dermatology Launceston General Hospital Take a history • • • • • • When did the rash first appear? Is it itchy? Have you had rashes before? Is there a family history of rashes? What have you tried? What do you think it is and what do you think caused it? Is the patient atopic? • Personal or family history of: ‐eczema ‐asthma ‐hayfever ‐urticaria ‐migraines Pattern Recognition • • • • Typical history Typical examination findings Common things happen commonly Beware the pattern that is not quite right Examining a rash • • • • • Good light Feel the rash A small amount of magnification Check for symmetry Check areas we often forget ‐nails ‐scalp/ears ‐creases ‐feet What happens in Eczema? • Impaired barrier function; water loss, prone to irritation and allergy. • Itch!! • Scratching • lichenification Eczema and Allergy • Take some time to explain this to parents. • 90% of children will not have a significant allergy with respect to their eczema. • The history is normally very suggestive. • May need to organize either prick tests or a blood test. Investigations • • • • • • • Possibly none. Swab of skin. Swab of nose. Skin scrapings. Biopsy. Blood tests. Skin allergy tests. General Skin Care • • • • • Regular moisturiser. Low irritant clothing. Avoid soap and other irritants. Avoid over‐heating. Keep showers quick and not too hot. Specific Measures • • • • • Avoid skin irritants. Topical steroid. Treat secondary infection. Avoid relevant allergens. Prevent re‐infection. Bleach Baths • • • • 100 litres of water. 1kg salt. 2capfuls bath oil. Half a cup (125ml) white king bleach. Poor response to treatment • Check for: ‐poor compliance ‐secondary infection ‐an unidentified allergen ‐quantity of topical steroid used ‐correct diagnosis Skin Irritants • • • • • • • Heat. Low humidity. Coarse fabrics. Sand. Soap. Hot water. Stress. Psoriasis and Cardiovascular Disease • There is an association between the two. • Remember to check risk factors including smoking, obesity, lipids, blood pressure and fitness. Psoriasis is a systemic disorder • Skin rash • Arthritis • Cardiovascular disease Psoriasis is an autoimmune disorder. • A T‐cell mediated inflammatory disorder ‐inflamed skin ‐inflamed joints ‐inflamed cardiovascular system Drug history • • • • Regular medication PRN medication Over the counter medication Complementary medication Rashes Quiz Dermatology: the big picture GP13 – October 2013 1.Psoriasis has associations with: 1. Arthritis 2. Cardiovascular disease 3. Diabetes 4. Schizophrenia 5. Depression (you may choose more than one answer) 2. When using topical steroids for eczema, they should be used for: 1. Two to three days only. 2. Up to a week. 3. For as long as the steroid is required. 4. Should be avoided if possible. 3. Eczema is caused by: 1. Allergies. 2. Stress. 3. A combination of genetic and environmental factors. 4. Infection. 4. Diagnose this rash from the history and photograph. 25 year old lady. Slowly spreading pimply rash on the cheek for about 2 months. No previous skin problems apart from a bit of acne. Works on a cattle farm and prepares cattle for showing. 5. Diagnose this rash from the history and photograph 70 year old man. Unwell for 6 months with some weight loss and a cough. Itchy for a few months, with the development of an eczematous and urticarial rash. Blisters have just started to appear in the rash. Chest x‐ray shows a suspicious nodule. Thank you