Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
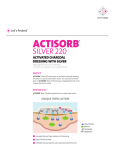
Copyright B 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Sheila K. MacBride, MN, BSc, PG Cert (TLHE), RGN, NDN, Onc Cert Mary E. Wells, MSc, BSc, RN Carole Hornsby, BSc, DCRT Lena Sharp, PhD, MSc, RN Kristina Finnila, RN Lynn Downie, BSc A Case Study to Evaluate a New Soft Silicone Dressing, Mepilex Lite, for Patients With Radiation Skin Reactions K E Y W O R D S Radiation skin reactions are a known side effect of radiation therapy. Moist Cancer desquamation reactions are not only painful but also may be a focus for infection Radiotherapy and can be dose limiting. There is a challenge to find a dressing which is protective, Radiation skin reactions comfortable, and atraumatic to delicate irradiated skin. The primary aim of this Wound care study was to evaluate patient comfort when using Mepilex Lite in the management of dry and moist desquamation. Secondary objectives included safety, tolerance, and influence on healing. Sixteen patients were recruited at 2 centers in the United Kingdom and in Sweden when they had a RTOG score of 3 and 1 symptom measured by the Radiation<Induced Skin Reaction Assessment tool. Digital photography was used at each weekly visit. Patients completed the Radiation<Induced Skin Reaction Assessment, daily diary cards, and open diaries for quantitative and qualitative evaluation. Some patients found that the dressing minimized pain during dressing changes and was easily lifted and adjusted without loss of adherent properties. A new dressing had a soothing or cooling effect on the skin, and some reported a more normal sleep pattern. The dressing had no negative effect on wound healing. The researchers conclude that the dressing provides a promising alternative to existing dressings and is worthy of further research. adiation skin reactions are a known adverse effect of radiation therapy affecting a large proportion of patients who receive radical treatment. Up to 95% of patients receiving radiotherapy to the breast, groins, and perineum or head and neck region experience marked erythema, R which can feel extremely hot, tight, itchy, and uncomfortable.1 Up to a third develop moist desquamation reactions,2,3 which not only are not painful but also provide an obvious focus for infection and can sometimes lead to early cessation of treatment and therefore reduce the dose of radiotherapy delivered. Authors’ Affiliations: School of Nursing and Midwifery, University of Dundee, Dundee, Scotland, UK (Ms MacBride and Ms Wells); Ninewells Hospital and Medical School, Dundee, Scotland, UK (Ms Hornsby and Ms Downie); and Karolinska University Hospital, Huddinge, Stockholm, Sweden (Dr Sharp and Ms Finnila). Corresponding author: Sheila K. MacBride, MN, BSc, PG Cert (TLHE), RGN, NDN, Onc Cert, University of Dundee, School of Nursing and Midwifery, Fife Campus, Forth Avenue, Kirkcaldy, KY2 5YS, Scotland, UK ([email protected]). Accepted for publication July 19, 2007. E8 n Cancer NursingTM, Vol. 31, No. 1, 2008 MacBride et al Copyright @ Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Cancer nurses frequently struggle to find an appropriate wound dressing that provides the protection required to enable patients with severe skin reactions to continue radiotherapy in comfort and also stays in place without causing further trauma. Surveys of radiotherapy practice suggest that a wide variety of wound dressings are used to manage radiation skin reactions and that practice is most often dictated by local preference.4 Recent clinical guidelines advocate the use of dressings that encourage moist wound healing,5Y7 but convincing evidence to support the use of a particular type of dressing is still lacking. Although there have been a number of studies evaluating skin products designed to prevent and alleviate erythema, relatively few have assessed the effects of wound dressings on established and severe radiation skin reactions.8 Rarely have studies considered patient comfort of primary importance. An ideal wound dressing would alleviate symptoms, improve comfort, promote healing, and prevent further skin damage from friction, trauma, or infection. In addition, such a dressing could be left in place during radiotherapy or at least removed for daily treatment without pain or trauma. Because of the increased risk of skin reaction development in skin-fold areas, the dressing would need to conform to awkward areas and be able to retain its shape and position without adhesive. Soft silicone dressings are designed to cause minimal trauma on removal and provide a moist wound healing environment without the danger of maceration of surrounding skin. They are already widely used in the treatment of burns9,10 and other skin lesions.11 They have also been found to protect irradiated skin without causing irritation.12 Mepilex Lite (manufactured by Molnlycke Health Care) is a thin flexible absorbent pad of polyurethane foam with an outer film of polyurethane, which is vapor permeable and waterproof. The backing film is coated with an acrylic adhesive whose function is to keep the dressing intact. The Safetac wound contact layer attaches readily to the skin but can be removed easily without causing damage to healthy tissue. This study was designed to evaluate the comfort and overall experience of using Mepilex Lite in the management of brisk erythema or moist desquamation during radiotherapy treatment. The study was initiated and commercially sponsored by the manufacturer. The study plan was developed by the commissioned researchers. (Karolinska University Hospital, Huddinge). Each center was allocated a convenience quota sample of 10 patients. Ethical approval was sought and obtained in both centers. Eligibility criteria are listed in Table 1. In both centers, a senior radiographer (CH) or nurse/ radiographer (LS, KF) was responsible for assessing eligibility. The Radiation-Induced Skin Reaction Assessment Scale (RISRAS)13Y15 was used to screen patients for entry into the study (see Figure 1). Patients undergoing radiotherapy to the head and neck or breast were recruited if they were experiencing severe erythema and/or moist desquamation along with at least 1 symptom (see Figure 1). Following informed consent, baseline demographic and treatment data were collected including age, sex, medical history, medical treatment, and cancer diagnosis. Digital photographs of the radiation skin reaction were taken, and patients were asked to assess their own symptoms using the self-report scale on the RISRAS. Patients were given a supply of appropriately sized dressings and some Mepitac soft silicone tape to be used if dressings needed additional fixation. Patients were encouraged to wash their skin gently each day with a mild soap and were shown how to apply the dressings to the affected area with the use of a mirror as necessary. Dressing changes were performed according to usual hospital routines, by nurses in clinic or by patients themselves. Dressings were to be used until the skin reaction had healed or for a maximum of 4 weeks after the patient received their last fraction of radiotherapy. All patients who participated in the study were to be followed for at least 15 dressing changes, unless healing took place sooner. Patients were assessed weekly using the RISRAS while on treatment and were asked to return to the treatment center each week after completion of treatment. Each day, patients recorded the number of dressing changes and size of dressings used; the extent to which they were troubled by pain, itching, burning, and sleep disturbance; and the level of comfort they experienced while wearing and removing the dressing on a symptom diary card. Patients were also given an open, unstructured diary in which they were asked to write about the impact of their skin reaction and any experiences of using the dressing. The radiographers/nurses responsible for assessing patients also Table 1 & Inclusion and Exclusion Criteria Inclusion Criteria n Aim of Study The primary aim of the study was to evaluate patient’s comfort with using Mepilex Lite. Secondary objectives included safety, tolerance, and influence on healing. n Methods This series of case studies took place in 2 sites. Patients were recruited from 1 of 2 radiotherapy departments in Scotland (Ninewells Hospital and Medical School) and Sweden Mepilex Lite for Patients With Radiation Skin Reactions Exclusion Criteria & Diagnosis of breast or head and neck cancer & Prescribed radical radiotherapy & Male or female & 18 years and older & Erythema Q 3 and/or moist desquamation 9 0 followed by at least 1 symptom Q 1 according to the RadiationInduced Skin Reaction Assessment Scale & Written consent & Allergy/hypersensitivity to any of the components in the dressing & Assessed as needing a highly absorbent dressing & Clinical staff considered that they would have problems complying with the protocol & Patients previously included in the investigation Cancer NursingTM, Vol. 31, No. 1, 2008 Copyright @ Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. n E9 Figure 1 n The Radiation-Induced Skin-Reaction-Assessment-Scale (RISRAS) modified Patient Symptom Scale. recorded their perceptions of the dressings in the Case Record Form. Digital photographs were taken each week, and any adverse events or changes in dressing use were documented. RISRAS symptom and appearance scores for each patient were added to form a total score, which was plotted on an EXCEL graph. Scores for diary symptoms and dressing changes were analyzed descriptively. Photographs were reviewed to document changes in skin reactions and assess the pattern in which dressings were applied. n Results Two patients were withdrawn from the study because they experienced increased itching after the dressing was applied and a reduction in symptoms when it was removed. These patients were documented as having experienced an adverse device event, thought to be due to individual sensitivity to the dressing. Three further patients discontinued the use of the dressing before the end point had been reached, choosing to use an alternative dressing. Patients often chose to apply the dressings in an individual manner that best suited their needs; for example, most patients used several smaller dressings to allow flexible movement and minimal tension rather than applying 1 larger dressing to the whole area (see Figure 2A). Patient Characteristics and Sample Symptoms Measured by the RISRAS Patients were recruited from both centers during November and December 2003 and January 2004. Center 1 recruited 5 patients, and Center 2 recruited 11 patients (see Table 2). All were white. Figure 3 shows the RISRAS scores of the 11 patients who used the dressings for at least 15 dressing changes, or until healing had occurred. E10 n Cancer NursingTM, Vol. 31, No. 1, 2008 MacBride et al Copyright @ Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Table 2 & Patient Recruitment a Patients 102, 208, and 209 were dropouts. However, patients 102 and 208 still fulfilled the criteria for being evaluable patients. As seen in Figure 4, overall patients experienced consistent improvement in all aspects of their skin reaction after applying the dressing. Some patients (see Figure 2B) demonstrated improved symptoms and even a decrease in their objective skin score after using Mepilex Lite, despite the fact that they had not completed their radiotherapy treatment. Comments from the radiographer/nurses showed that improvements in patients’ skin condition had been faster than expected. Patient Diary Cards The diary cards provided information on the subjects’ perception of comfort when wearing and removing the dressings (see Figure 3a and 3b). The average comfort score for the 15 evaluable patients who completed this question on the diary card was 2 (quite a bit). The average comfort score upon removing the dressing for the 11 evaluable patients who completed this question was 2.4 (2 = quite a bit and 3 = very much). Open Diaries The open diaries were intended to offer a view of the impact of the radiation skin reaction and the application of the dressings on quality of life. Four Swedish and 5 British patients completed diaries, and these were translated into English and reviewed by one of the investigators (SKM). Comments were analyzed for positive or negative orientation. Positive responses included the benefits of the dressing in terms of reducing friction from clothes, bedclothes, and car seat belts; the difference made by the dressings on comfort and activities of daily living; the dressing staying in place and relieving pain (eg, ‘‘And thanks to the dressing, my blouse doesn’t rub against the scar on my chest’’ [patient 204/day 2]). Many commented on the best way to use the dressings for comfort and ease of movement in activities of daily living (eg, ‘‘I don’t feel so tired today as there was not so much painVthe pain even over the 2 or 3 days before using the dressing, had been very wearing and tiring’’ [patient 104/day 2]). Indeed the focus of comments was predominantly the benefit Mepilex Lite for Patients With Radiation Skin Reactions of the dressings in promoting activities of daily living such as exercise and sleep (eg, ‘‘First night, big difference, did not wake from any pain’’ [patient 208/day 1]). Negative comments mainly focussed on the difficulties of managing very moist wounds, where the dressing did not always remain comfortable or stay in place. Some patients also commented that the dressing seemed to remove a superficial layer of skin and were understandably concerned about this, (eg, ‘‘Skin coming away with dressing, but no pain with it’’ (104/day 6)]. There were some more detailed commentaries on patients’ experiences of moist desquamation. Some differences were found between the UK and Swedish responses. Four Swedish patients completing diaries described dealing with the experience in a daily time frame and the relief of being able to manage the skin reaction using dressings. UK patients described the dressing and its contribution to their quality of life, the experience of moist desquamation, and the significance of the radiographer and clinical nurse specialist as a support in the experience (eg, ‘‘The only reason I changed the dressing twice in the last 24 hours was a personal rather than a medical one. It was my son’s 21st birthday party and as it was going to be an effort for me due to fatigue from the radiotherapy, I wanted to be sure that I felt as comfortable as possible’’ [patient 104/day 4]). Not all patients completed the open diaries, and the analysis of positive and negative comments is clearly limited in scope. However, the detailed insights gained do suggest that open diaries may be a useful means of determining the impact of radiation skin reactions on individuals’ quality of lifeVan aspect of research that is largely absent in the literature. n Discussion The optimal management of radiation skin reactions remains a daily challenge for healthcare professionals. Surveys conducted in the last 10 years show that practice is inconsistent and controversies about the most appropriate wound management technique still exist. Recent guidelines5Y7 advocate moist wound healing methods for moderate to severe radiation skin reactions, but evidence to support such advice is limited. A wide variety of dressings have been evaluated,8 and many studies do support the use of hydrogels, hydrocolloids, or films to alleviate discomfort and promote healing, but this is not exclusively the case. Mak et al16 found no significant differences in healing between patients using hydrocolloids and those using gentian violet; although comfort and aesthetic appearance were superior in the hydrocolloid group, wound size was greater, and there was a trend toward higher pain severity. A recent randomized trial3,17 also suggests that we may need to reconsider the place of simple protective dressings and consistent skin hygiene in maintaining skin integrity during radiotherapy. Porock and Kristjanson18 concluded that the choice of topical product should be based on patient preference and comfort, and the conflicting evidence we have to date adds weight to this argument. Cancer NursingTM, Vol. 31, No. 1, 2008 Copyright @ Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. n E11 Figure 2 n (A), Patient 103. This was a 41-year-old lady who had wide local excision of the breast after a diagnosis of breast cancer. The subject was recruited to the study when she had received her 45-Gy prescribed dose of radiotherapy to the breast and surrounding tissue. She continued treatment and received a further 16 Gy in 8 fractions to a field 8 8 cm to the scar area. Aqueous cream had been prescribed for application to the skin within the treatment field. The photographs show the patients’ skin at recruitment, 1 week later, and 2 weeks later at final visit. The RISRAS shows that despite persistent moist desquamation, pain and itch were reduced by the application of the dressing. This patient rated the dressing overall as ‘‘very good.’’ She used the dressings in a patchwork pattern to allow easy movement. Her diary comments that she found the dressing simple to apply and exceptionally comfortable. She also notes immediate relief of symptoms when the dressing was applied, friction from clothing was reduced, and a better sleep gained. (B), Patient 211. This 54-year-old gentleman at the Swedish center was recruited when he had received 62 Gy from 64-Gy prescription to the head and neck region for laryngeal cancer after laryngectomy. Propyless lotion had been applied to the skin reaction when erythema developed. Grade 3 skin reaction therefore occurred during his radiotherapy. The photograph displays the extent of the skin reaction at recruitment. The RISRAS graph illustrates a faster skin healing time than might otherwise have been expected for someone with this dose to this region of the body. The dressings were cut to fit his stoma. He rated the dressing as very good overall and also found conformability of the dressing to be good. In his diary, he noted that application of the dressing reduced pain and tightness associated with his skin reaction. E12 n Cancer NursingTM, Vol. 31, No. 1, 2008 MacBride et al Copyright @ Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Figure 3 n A. Center 01. Question 5: How comfortable was the dressing when it was in place? B. Center 01. Question 6: How comfortable was the dressing to remove? The primary aim of this case study was to evaluate comfort with Mepilex Lite. Our results suggest that most patients found the dressing comfortable to wear and to remove. In many cases, it had a considerable (and sometimes immediate) impact on activities of daily living, including sleeping, wearing clothes, and using a car seat belt. A few patients did experience sensitivity to the dressing, and it is of some concern that 2 patients had to stop using Mepilex Lite because of severe itching (an adverse device event that had not been previously noted by the manufacturers in previous studies). One patient also found that the dressing was inadequate for the amount of exudate produced by her radiation reaction. These findings suggest that it may be appropriate to ‘‘patch test’’ the dressing before applying it over a large area, and that highly exuding wounds may require a more absorbent dressing such as Mepilex or an alginate or foam. Given that most radiotherapy treatment is delivered on an outpatient basis and developments in care delivery require patients to assume greater responsibility for self-care, it is important that dressings can be managed by patients themselves. Our experience suggests that patients in this study were able to apply, change, and adapt dressings to suit their needs, and indeed several patients cut the dressings to shape or used dressings in a ‘‘patchwork’’ pattern to cover affected areas and alleviate discomfort (see Figure 4). Those with large areas of moist desquamation found it more comfortable to use a combination of small dressings rather than one large one, commenting that they felt less tension on their skin. Dressings sometimes curled up or wrinkled in awkward areas such as skin folds, but Mepitac tape was used very successfully to overcome this problem. Some patients suggested that it would be useful to have a template to follow, and it may be that individual templates could be suggested by nurses or radiographers overseeing the patients care. Mepilex Lite for Patients With Radiation Skin Reactions Experienced nurses and radiographers monitoring the use of Mepilex Lite were very positive in their evaluation of the dressings. Their comments largely supported those of patients, agreeing that the dressings were very successful for patients with erythematous and slightly moist skin reactions but were less effective in patients whose reactions were producing large amounts of exudate. The generalizability of this study’s findings is limited by the small number of patients and the fact that there is no control group. However, case studies using multiple methods are useful for the specific descriptive information they provide about individual cases. They can make a significant contribution to theory and practice through ‘‘force of example.’’19 The generalizability of case studies should therefore be judged in terms of the relevance of findings to others, rather than by the statistical generalization of findings to populations.20 We did not attempt to standardize the variable of radiation dose because the aim of the study was to evaluate the comfort and overall experience of using Mepilex Lite in a selection of typical patients undergoing radiotherapy, rather than to draw any specific conclusions about skin reaction development and healing in relation to dose. However, future studies should include larger numbers of patients, with suitable control groups that take account of variables such as radiotherapy dose and other known risk factors.3 It should be noted that only patients with head and neck or breast cancer were included in this study and that those with mild radiation skin reactions or skin reactions requiring a highly absorbent dressing were excluded. The results of this study suggest that Mepilex Lite is worthy of further investigation in patients who are receiving radiotherapy treatment to other sites associated with radiation skin reactions such as the pelvis. However, we believe that we have established proof of principle, that Mepilex Lite provides a safe and attractive alternative to existing dressings and that it provides particular protection and comfort. n Conclusions This small case study suggests that Mepilex Lite promotes comfort in patients with brisk erythema or moist desquamation and that it is safe and well tolerated by patients undergoing radiotherapy treatment. The fact that 2 patients had to stop Figure 4 n RISRAS scores for all subjects in the study. Cancer NursingTM, Vol. 31, No. 1, 2008 Copyright @ Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. n E13 using the dressing due to itching is of some concern, but this contradicts previous research using this and other silicone dressings. Because itching is a feature of the symptom experience, this may be coincidental and further trials should consider testing for silicone sensitivity. Mepilex Lite seems to promote healing and may be left in place during treatment. Mepilex Lite offers a real alternative to current treatments in use for severe erythema and moist desquamation and has many important advantages in terms of comfort, ease of removal, skin protection, and quality of life. 7. 8. 9. 10. ACKNOWLEDGMENTS 11. We would like to acknowledge the genuine support and encouragement from the members of the team at Molnlycke Healthcare, in particular, Bengt, Annelie, and Jens. 12. References 13. 14. 1. Porock D. Factors influencing the severity of radiation skin and oral mucosal reactions: development of a conceptual framework. Eur J Cancer Care. 2002;11:33Y43. 2. López E, Nuńez MI, Guerrero MR, et al. Breast cancer acute radiotherapy morbidity evaluated by different scoring systems. Breast Cancer Res Treat. 2002;73(2):127. 3. Wells M, Macmillan M, Raab G, et al. Does aqueous or sucralfate cream affect the severity of erythematous skin reactions? Radiother Oncol. 2004;73:153Y162. 4. Lavery BA. Skin care during radiotherapy: a survey of UK practice. Clin Oncol (R Coll Radiol). 1995;7:184Y187. 5. Nysted KE, Hill JE, Mitchell AM, et al. The standardisation of skin care in British Columbia: a collaborative approach. Oncol Nurs Forum. 2005; 32(5):1199Y1205. 6. Glean E, Edwards S, Faithfull S, et al. Intervention for acute radiotherapy induced skin reactions in cancer patients: the development of a E14 n Cancer NursingTM, Vol. 31, No. 1, 2008 15. 16. 17. 18. 19. 20. clinical guideline recommended for use by the College of Radiographers. Radiother Pract. 2001;2:75Y84. NQI Scotland. Best Practice Statement: Skincare of Patients Receiving Radiotherapy. Edinburgh: Scottish Executive Health Department; 2004. Wells M, MacBride SK. Radiation skin reactions. In: Faithfull S, Wells M, eds. Supportive Care in Radiotherapy. Edinburgh: Churchill Livingstone; 2003. Platte A, Judkins K. A comparative study of silicone net dressing and paraffin gauze dressing in skin grafted sites. Burns. 1996;22(7): 543Y545. Gotshall S, Morrison IS, Eichelberger MR. Prospective, randomised study of the efficacy of Mepitel on children with partial thickness scalds. J Burns Care Rehabil. 1998;19(4):279Y283. Taylor R. Use of a silicone net dressing in severe mycosis fungoides. J Wound Care. 1999;8(9):429Y430. Adamietz I, Mose S, Haberl A, Saran FH, Thilmann C, Böttcher HD. Effect of self-adhesive, silicone-coated polyamide net dressing on irradiated human skin. Radiat Oncol Invest. 1995;2:277Y282. Noble-Adams R. Radiation-induced skin reactions, 1: an examination of the phenomenon. Br J Nurs. 1999;8(17):1134Y1140. Noble-Adams R. Radiation-induced skin reactions 2. Br J Nurs. 1999;8: 1208Y1211. Noble-Adams R. Radiation-induced skin reactions, 3: evaluating the RISRAS. Br J Nurs. 1999;8(19):1305Y1312. Mak SS, Molassiotis A, Wan W-M, Lee I, Chan E. The effects of hydrocolloid dressing and gentian violet on radiation-induced moist desquamation wound healing. Cancer Nurs. 2000;23(3):220Y229. Macmillan MS, Wells M, MacBribe S, et al. A randomised comparison of dry dressings versus hydrogel in the management of radiationinduced moist desquamation. Int J Radiat Oncol Biol Phys. 2007;68(3): 864Y872. Porock D, Kristjanson L. Skin reactions during radiotherapy for breast cancer: the use and impact of topical agents and dressings. Eur J Cancer Care. 1999;8:143Y153. Flyvberg B. Five misunderstandings about case-study research. Qual Inq. 2006;12(2):219Y245. Lincoln YS, Guba EG. Judging the quality of case study reports. Qual Stud Educ. 1990;3(1):53Y69. MacBride et al Copyright @ Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.