Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
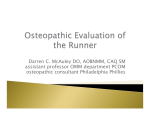
Derm Dec NH 2 13/12/2005 12:14 Page 1 A guide to skin conditions of the feet Dermatological foot problems can often be misdiagnosed and hence mismanaged, writes Hilda O’Shea Forum Dermatology Figure 1. Athlete’s foot – tinea pedis. Figure 2. Paronychia. FOOT PROBLEMS present in a dermatological context in general practice frequently. They often be misdiagnosed and hence mismanaged. This article describes the most common skin conditions of the feet I would see on an average week in general practice. Often these conditions are picked up incidentally during the course of a consultation for some other complaint. Athlete’s foot – tinea pedis This is the commonest dermatophyte infection in the developed world. Three species that predominantly reside on humans are Trichophyton rubrum, Trichophyton mentagrophytes and Epidermophyton floccosum. Together they are responsible for the majority of cases. They can be responsible for toenail infections and often occur simultaneously. Toe web infection It can present as toe web maceration; look especially between the fourth and fifth toe. This is the commonest presentation and age of onset is usually in the teens. Males are affected more frequently than females. Tight-fitting shoes and moist conditions favour growth of the fungus. It’s usually asymptomatic, but it can be very itchy and foul smelling, with exacerbations in hot, humid weather. Treatment is with topical anti-fungals. It can be complicated by secondary infection with staphylococcus aureus and haemolytic streptococci, with development of impetigo or erysipelas. These require a broad spectrum of antibiotics, orally, to clear, as well as topical anti-fungals, eg. Daktarin twice daily for three weeks and/or Lamisil once daily for one week. Figure 3. Pitted keratolysis Application of aluminium chloride 20% may eliminate the hyperhidrosis. The rate of recurrence is high. Papulo-squamous hyperkeratotic plantar infection – ‘Moccasin’ type Characterised by erythematous, scaly lesions affecting the soles of usually one foot and is usually caused by Trichophyton Rubrum. Differential diagnosis is psoriasis or juvenile plantar dermatosis. This usually needs systemic treatment with, for example, Lamisil 250mg daily for two weeks or Sporanox 200mg twice a day for one week. Vesico-pustular plantar infection Affects the side and sole of the foot, with a cluster of blisters, itchy and spreading. It is usually caused by Trichophyton mentagrophytes. Differential diagnosis here is pustular psoriasis. Treatment is with topical anti-fungals initially and then with systemic Lamisil later if the skin scrapings are positive. Paronychia With this, the base of the nail is inflamed and swollen. It may be acute or chronic and it often occurs in association with an ingrowing toenail. The commonest pathogen here is Candida, which can be mixed with staphylococci. Treatment has to be combined: oral Erythrocin for two to three weeks, Fucidin cream daily and oral anti-fungals for one to two weeks. Soaking – potassium permanganate twice daily for five days – can be a great help too. Pitted keratolysis This keeps turning up and is very satisfactory to treat. It presents as a honeycomb appearance on the sole of the foot. FORUM December 2005 41 Derm Dec NH 2 13/12/2005 12:14 Page 2 Forum Dermatology Hyperhidrosis is often present too and malodour. Treatment is both topical and systemic: antibacterial cream, eg. Fucidin and Erythrocin 500mg twice daily for one week. Prevention of recurrence can be accomplished with control of hyperhidrosis and keeping feet cool and dry with frequent change of cotton socks and open shoes; sandals if possible. Patients should not wear the same shoes continuously – dry them out and wear boots for short periods only. Juvenile plantar dermatosis This is characterised by dry fissured dermatitis of the plantar surface of the forefoot. Occurs in young boys aged three to 15 years and is associated with wearing occlusive footwear, ie. trainers and nylon socks. It is related to friction. The plantar surface is dry, red and glazed with a cracked appearance. It is symmetrical on both feet. Treatment is with topical preparations such as coal tar creams and white soft paraffin. Topical steroids are of no benefit. If fissures are the problem, superglue can be applied and that will relieve the pain. Psoriasis of the foot This presents as a scaly, red, well demarcated plaque on the side of the feet or soles, with sparing of the instep. Differential diagnosis is for Tinea Pedis and hyperkeratotic plantar eczema. Usually there is psoriasis at other sites and a positive family history to help with the diagnosis. Other presentations include pustular psoriasis of the foot, again usually symmetrical and affecting the instep. It is mainly characterised by erythematous plaques with white and yellow pustules on the soles and older lesions being a red-brown colour. This occurs mainly in the older population. It responds well to topical steroids and plenty of emollients. More severe cases may need referral for retinoids or methotrexate. All the above cases should have skin scrapings taken to rule out or confirm fungal infection. When mycology is positive, anti-fungals can be started. Skin scraping is a simple test to perform: just scrape the skin lightly with the back of a scalpel blade and let it fall onto dark paper, preferably black (can be bought in art shop and cut up into little squares). It’s well worthwhile and can produce positive results when least expected and make treatment more specific. The other pitfall to avoid is applying steroid cream blindly and hoping for the best; if it’s a fungal infection, it will surely make it worse – Tinea Incognito. In very small children look for scabies lesions on the soles of the feet. Hilda O’Shea is in practice in Cork city To Subscribe to Forum World of Irish Nursing & Midwifery Irish Journal of Psychological Medicine Extenza Turpin Stratton Business Park, Pegasus Drive, Biggleswade, Bedfordshire SG18 8QB, England Tel: +44 01767 604951 Fax: +44 01767 601640 Email: [email protected] www.extenza-turpin.com