Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
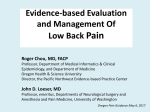
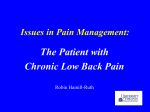
Low back pain Introduction to Primary Care: a course of the Center of Post Graduate Studies in FM PO Box 27121 – Riyadh 11417 Tel: 4912326 – Fax: 4970847 Aim: At the end of this presentation, the participants will have knowledge on the management of low back pain. Objectives: At the end of this session, the trainees should; • be able to discuss the prevalence of disc mediated low back pain and current techniques for diagnosis • be able to develop a structured approach to history taking and physical examination in patients with low back pain • be able to review the major types of mechanical back pain, and describe common etiologies • be able to explain the difference between simple and complex low back pain • be able to describe emerging interventional and biological therapies to treat low back pain Timing Definitions • Acute LBP lasts for < 6 weeks • Sub-acute LBP lasts for 6-12 weeks • Chronic LBP lasts for > 12 weeks • Acute & Sub-acute account for 90% of LBP Epidemiology • 75% of adults will experience LBP at some point in their lives • 5th most common cause of all physician visits • Peak incidence 20-40 years old; More severe in older patients • 85% of patients have no definitive anatomic cause or imaging finding • Most cases are self limited with serious problems in < 5% • Most common cause of work-related disability for individuals < 45 years old • Low back pain among Saudi school workers in Jeddah • The results of this study show • a prevalence of 26.2% with low back pain • Saudi medical journal 1998 • A response was obtained in 5,743 (97.4%). Their mean age was 34.14 ± 15.16 (range 16-99). Back pain was reported by 1,081 (18.8%), wherein 499 (8.8%) were men, and 574 (10%) were women. Back pain was more prevalent in married (23.3%) individuals than unmarried (6.4%). • How common is back pain in Al-Qaseem regoin • Saudi Med J 2003 Causes of back pain LBP: Risk Factors • Heavy lifting and twisting • Obesity • Poor physical fitness/conditioning • History of low back trauma • Psychiatric history(chronic LBP) The European guidelines also classify acute back pain into three categories. These are1: Serious spinal pathology • – This includes infection, malignancy, fracture, and inflammatory causes such as ankylosing spondylitis Nerve root pain – The sciatic nerve becomes trapped or irritated either in the lumbosacral spine or the muscles of the lower back or buttock, if they go into spasm secondary to pain – It may take up to two months for the patient's symptoms to resolve Non-specific low back pain – This is back pain that is not due to either serious spinal pathology or nerve root pain – It is often triggered by a minor sprain or strain of the back – Pain may be mechanical - worsened by certain movement or postures – Pain usually improves within two weeks. When you assess patients who present with back pain you • should: • Rule out serious pathology by asking about red flags • Ask about nerve root pain • Examine all patients - usually a brief examination is sufficient • Examine other joints close to the back such as the hip joint for pain – Pain can be referred from the hip joint to the back. Red Flags • • • • • • • • Retention of urine or incontinence Onset over age 55 or under 20 Symptoms of systemic illness - weight loss, fever Morning stiffness Severe progressive pain A prior history of cancer Intravenous drug use Prolonged steroid use yellow flags • An inappropriate perception of back pain – The belief that back pain is harmful and disabling – The belief that passive activity such as bed rest is better than staying active • Lack of support at home and social isolation • Mental health problems such as depression, anxiety, and stress • Problems at work such as job dissatisfaction • Claims for compensation and benefits. Examination • • • • • LOOK FEEL MOVE STRAIGHT LEG AND FEMORAL STRETCH TEST POWER,TONE,SENSATION + REFLEXES LOOK • Examine standing-look for deformity such as increased or decreased lordosis, obvius scoliosis, soft tissue abnormalities eg. Hairy patch, scars FEEL • Spinous processes and paraspinal tissues for any local tenderness or spasm • Palpate vertebral column for point tenderness MOVE • Flexion-try to touch toes with your legs straight and note how far eg. To knees,ankles, mid shin • Extension-straighten up and lean back as far as you can • Lateral flexion-reach down to each side touching the outside of each leg and record amount of flexion • rotation Straight Leg Raising L4,5,S1 Power/tone/sensation/reflexes • Power-grade 0-5, test all joint movements • Tone- should include anal tone esp. if red flags • Sensation- esp. perineal/perianal • Reflexes-knee L3,4 ankle L5,S1 plantar S1,2 Motor Testing Deficit should align with areas of pain • Toe Walk tests calf muscle (S1) • Heel Walk tests ankle and toe dorsiflexion (L4, L5) • Single squat and rise (L4) • Ankle Jerk (S1) • Knee Jerk (L4) Sensory Tests Deficits should align with areas of pain • Light touch on – Medial foot (L4) – Dorsal foot (L5) – Lateral Foot (S1) When to Image • • • • Consider in all ages if any trauma Consider in older adults with any falls Pain not improved over 4 to 6 weeks If there is a history of chronic steroid use or osteoporosis • If there are any “Red Flags” and suspicion for cauda aquina, infection, cancer How to image • X-ray – Fracture, tumour, infection • CT – – – – Suspect disc herniation that is being considered for surgery Detail an unstable fracture Clarify abnormality seen on bone scan If spinal stenosis suspected & want to localize pathology • MRI – Extent of tumour – Recurrent or unremitting post surgery radicular pain – Cauda equina Management of LBP • • • • • • Keep moving! (only a few days rest at most) Heat/cold Decrease bending and lifting Frequent position changes NSAID/Acetaminophen Low impact aerobic exercise – Walking, swimming • Education regarding proper lifting, bending techniques • Progression of more specific strengthening exercise – Core muscles • Gradual progression back to normal activity Treatment Options for Mechanical LBP Scheduled oral NSAIDS are recommended; there is strong evidence that they significantly reduce pain For NSAIDs – remember ease of use and cost – none more effective than another Tylenol avoids the GI and renal issues found with NSAIDS, however some studies found it less effective for pain than NSAIDS May need opioids for severe pain; side affects include drowsiness and addiction; administer for 1-2 weeks only Treatment Options • Strong evidence that muscle relaxants such as Flexeril, Soma or Skelaxin are helpful – most beneficial in first one to two weeks of treatment – most effective when combined with NSAIDS – side affects include drowsiness and dizziness – evaluate risks vs. benefit Treatment Options • Superficial heat therapy has been helpful in reducing LBP – provides muscle relaxation and analgesia • Evidence to support use of ice is inconclusive • Physical Therapy appears to be helpful in subacute LBP – 2-6 sessions – Beneficial for pateint education and activating exercise programs Treatment Options • Epidural steroid injections may be helpful in patients with radiculopathy who do not respond to 6 weeks of conservative treatment – should be preceded by MRI or CT – recommendation is 1-3 injections – most effective when combined with medication and physical therapy Treatment Options • Bedrest is not recommended, there is strong evidence to stay active, however activity may need to be modified • If bedrest is necessary for severe pain, it should not last longer than 2-3 days • There is insufficient evidence to support massage • There is mixed evidence on efficacy of acupuncture Treatment options • Some evidence that spinal manipulation results in short-term improvement in pain but is less effective than usual methods (analgesics, muscle relaxants, PT) • “Back schools”, lumbar supports, traction and ultrasound have not been shown to be effective Treatment Options • Despite the high rate of spinal surgery, evidence shows only a small number of patients have improvement Summary of treatment recommendations Van Tulder M and Koes B. Low back pain (acute & chronic). Clinical Evidence 2006 Effectiveness Acute low back pain Chronic low back pain Beneficial Advice to stay active, NSAIDs Exercise therapy, intensive multidisciplinary treatment programmes Trade-off Muscle relaxants Muscle relaxants Likely to be beneficial Multidisciplinary treatment programmes (for subacute low back pain), spinal manipulation Analgesics, acupuncture, antidepressants, back schools, behavioural therapy, NSAIDs, spinal manipulation Unknown Analgesics, acupuncture, back schools, behavioural therapy, electromyographical biofeedback, epidural steroid injections, lumbar supports, massage, multidisciplinary treatment (for acute low back pain), temperature treatments, traction, TENS Electromyographical biofeedback, epidural steroid injections, local injections, lumbar supports, massage, traction, TENS, Unlikely to be beneficial Specific back exercises — Ineffective, or harmful Bed rest Facet joint injections 3 WHO's three step ladder to use of analgesic drugs www.who.int/cancer/palliat ive/painladder 2 1 Complications • Development of chronicity and depression • Disability and loss of employment • CAUDA EQUINA SYNDROME- when disc material is pushed into the spinal canal and compresses the bundle of lumbar and sacral nerve roots. Permanent neurological sequelae can occur if not treated as emergency Prognosis • In one month, 35% have no symptoms • In 3 months, 85% have no symptoms • In 6 months, 95% have no symptoms • Remember, the etiology of LBP is usually not identified (85%) but almost all patients get better! When to refer Referrals • Not improving in 4 to 6 weeks • Deficit in more than one root • Progressive root loss • Loss of bladder and/or bowel function • Red flag suggesting fracture, tumour, infection – Get imaging & refer to spine surgeon Who to refer to? Referrals • Joint inflammation and/or other joint involvement – Order baseline labs & refer to rheumatologist • UMN symptoms & signs – Refer to neurologist and/or spine surgeon • Persistent LBP – Refer to physiatrist or spine surgeon • Spinal stenosis suggested – Refer to physiatrist or spine surgeon • Chronic pain syndrome features – Multidisciplinary pain clinic referral Denniston PL, ed. Official Disability Guidelines. 11th ed. Encinitas,Calif.: Work Loss Data Institute, 2005. Who needs Surgery? • Unstable Spine Acute fractures with Neurologic deficit. • Severe Stenosis – After failure of aggressive non-operative tx. • Tumor? • Progressive Neurologic deficit Thank you