Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
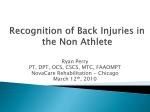
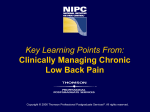
Acute low back pain Opportunities for care (honest) Tim Carey MD MPH Dept of Medicine Sheps Center for Health Services Research UNC Chapel Hill Low back pain • 80% lifetime prevalence • 3% of population seeks care for LBP/yr • Average MD sees 2-4 LBP pts/wk • Medical costs > $25 billion and rising Back pain therapy project TC 3-18 Tim/pres/1/24/97(6) SCIENTIFIC INQUIRY Hypothesis Evidence fails to disprove > Try to disprove > Tentatively accept hypothesis; test implications < Results replicated, implications prove valid < Refine practical application > TOO MUCH BACK PAIN RESEARCH Hypothesis (new test or treatment) > Try to prove hypothesis Weak test offers some support Establish clinic devoted to hypothesis < < > Proclaim fact, devise billing code, form interest group to lobby for support, publicize Figure 2. A contrast between the usual approach to scientific inquiry and too much back pain research. Paradigms of LBP • “Don’t worry-be-happy” - 95% of patients with LBP recover • “The grim slide into disability” - High recurrence rates - Over 1/3 of patients have chronic symptoms TC 2-7 EXPLANATORY MODELS IN BACK PAIN • ALLOPATHIC: RUPTURED DISC, “BLACK BOX” • CHIROPRACTOR: SUBLUXATION OF THE SPINE • PHYSICAL THERAPY: STRENGTH, INFLAMMATION • PATIENT: DISC, ARTHRITIS • SUPPLIERS: WRONG BED, WRONG CHAIR TC 7-11 THE INJURY PARAGIGM • IF THE BACK HURTS, IT MUST HAVE BEEN INJURED • IF SOMETHING IS INJURED, IT NEEDS REST • INJURIES OCCUR THROUGH SOMETHING WE (OR SOMEONE ELSE) DID WRONG • INJURIES ARE PREVENTABLE TC 7-10 Acute low back pain • Affects 8% of population each year • 40% seek care • Second most common symptomatic reason for care seeking at primary care MD offices • 95% functional recovery at 6 months • Recurrence common TC 2-9 Chronic Back Pain • Common, morbid, expensive • Epidemiology unclear due to variable definitions of the syndrome • 1992 estimate of chronic LBP in NC=3.9% – Functionally impairing and – >3 months in duration (or >25 episodes per year) • 2006 estimate 8-9% using same definition • Care seeking also increased Why are physicians uncertain? • Voluminous data • Limited training in LBP in primary care • Specialists see very different diagnostic spectra from each other • Patient expectations may not be congruent with caregiver ability to affect the natural hx of the illness TC 7-18 What hurts? • • • • • • Discs Annulus fibrosis Facet joints Muscles Ligaments Inter-individual variability in sensitivity to somatic input When to see a physician? • • • • • • Unrelenting, severe pain Leg weakness “Red flag’ underlying conditions Significant trauma Symptoms not improving after 2 weeks or so Off work for > 5 days (variable depending on job) Initial evaluation Look for the “red flags” • • • • • • • Weight loss Fever Hx non-skin malignancy Chronic steroid use, osteoporosis Significant trauma Hx IVDA Progressive neurologic deficit Serious causes of acute low back pain • Metastatic malignancy – Primary malignancy • Infectious processes • Cauda equina syndrome – Central disc herniation • Compression fracture • (Spinal stenosis) • (Acute disc herniation) Physical exam • Touch what hurts • Gait, observation, Waddel signs for chronic symptoms • Straight leg raise • Knee jerk • Ankle jerk • Foot dorsiflexion • (Sensory exam) By Gary Larson, It Came From the Far Side TC C-1 Patients Eligibility Requirements Patients with low back pain • Age > 20 and < 75 • < 10 weeks duration this spell • No previous care for this spell • No back surgery or chymopapain ever • No history of non-skin malignancy • Not pregnant • Had home telephone • English speaking NC Back Pain Project TC 7-19 NC Back Pain Project Cohort Study Interview Schedule Index Visit Enrolled Baseline Interview 2 wk 4 wk 8 wk 12 wk 24 wk “All Better” At Interview TC 6-1 Figure 1.-Cox-Model Curves of the Time from the Initial Visit to Functional Recovery among Groups of Patients with Low Back Pain Treated by Various Types of Providers. The confidence intervals overlap (data not shown), with no statistically significant differences among the six strata. Data have been adjusted for base-line differences in functional status (the Roland-Morris score), the presence or absence of sciatica, income, duration of pain before the index visit, workers' compensation status, and educational level. Because of overlap, not all of the six curves are visible From: Carey: N Engl J Med, Volume 333(14).Oct 5, 1995.913-917 Total Outpatient Direct Medical Charges per Episode of Low Back Pain STRATUM MEAN ADJUSTED MEAN* Urban Primary Care $478 $508 Rural Primary Care $540 $474 Urban Chiropractor $508 $783 Rural Chiropractor $554 $611 Orthopedist $809 $746 HMO $365 $435 *Adjusted for baseline functional status sciatia, income, duration of pain, and worker’ compensation TC 7-4 Carey Slides 13/Kathë Recurrence of LBP from 6-22 Months Among Those Completely Recovered by 3 Months (N=754) Percent Recurrence 60 50 40 30 20 10 0 Urban Prim N=137 Rural Prim N=157 p = 0.01 NC Back Pain Project Urban Chiro N=128 Rural Chiro N=166 Practitioner Strata Ortho HMO N=72 N=54 No Recurrence Mild Recurrence Severe Recurrence Imaging procedures • Who needs radiographs (x-rays)? • High vs. low risk patients. • Non-specific ‘wear and tear’ findings common • Guidelines available for 10 yrs but imaging procedures persist. • How many views? - 5 views vs. 3. How much incremental benefit is gained by two additional views? TC 3-30 By Cary Larson, It Came From the Far Side TC C-2 Medications • • • • • • Very commonly used in LBP Analgesia Role of NSAIDS Muscle relaxants Narcotic analgesics Herbal remedies Injection therapy • Limited role in new onset LBP • Modest efficacy in the most optimistic studies • Substantial non-specific effect of any injection Physical therapy • • • • • Evaluation, advice, physical treatments May include manual therapy Minimal standardization Little research in the past Probably not helpful in the first several weeks of acute LBP • May be useful in chronic LBP if the approach is an active one Spinal manipulation • • • • Commonly used across several specialties Excellent patient satisfaction Probably effective compared with no treatment Probably not substantially different in clinical outcome compared with usual allopathic treatment (evaluation, advice, meds) • Somewhat more expensive Acupuncture • Biologic rationale unknown but substantial historical use • Non-standardized intervention, substantial variability among practitioners, across theories • Recent RCT negative when compared with medical treatment or massage Early return to work • Work disability is a large portion of the social cost of LBP • Pure educational programs are ineffective • Mounting evidence that active case management stressing early return to work or modified work reduces cost and improves function • Need to streamline process of modifying work • Early communication with a receptive supervisor is key • Exercise is good Utility of surgery • Modest evidence for substantial improvement in leg pain in sciatica if not improved in 6 weeks of conservative rx • Little consensus as to indications for and results from fusion for chronic LBP – Randomized trial demonstrated modest benefit in disc surgery, degenerative spondylolisthesis IDET Intradiscal electrothermal therapy • • • • • • Novel procedure, percutaneous Heats disc to > 60 deg C Several month rehab necessary Case series data encouraging European RCT of similar procedure negative Urgent need for US RCT PATIENT SATISFACTION How would you rate… MD/HMO Chiropractor Patients Patients (N=1027) (N=606) Percent answering “Excellent” …the information you were given? 30.3 47.1 …the way the doctor treated your back problem? 31.5 52.1 …the overall results of your treatment? 26.5 42.1 (The P value for each question asked is P<0.0001) TC 7-5 PATIENT SATISFACTION Did the doctor who enrolled you in this study… …take a detailed history of your back pain? …do a careful examination of your back? …explain the cause of your back problem clearly (Cont.) MD/HMO Patients (N=1027) Chiropractor Patients (N=606) Percent answering “Yes” 68.4 88.4 79.9 96.1 74.6 93.6 (The P value for each question asked is P<0.0001) TC 7-6 Incidence of Chronic Low Back Pain Developing from Acute Low Back Pain Of 100 patients presenting for acute low back pain: 7-8 will still have significant symptoms 3 months later 25 will have mild back pain but be able to perform their usual daily activities TC 7-7 Where to refer? • Physical therapy can be very helpful, but how to find the right one? - Exercise over modality • Orthopedic/neurologic surgeons - Is an operation needed? • PM+R • Multi-specialty pain management including anesthesiology • Primary care with a hobby - Kaiser-Permanente model TC 6-30 Pain modulating therapy • Tricyclic antidepressants – Dose titration • (SSRI’s) • Possibly SNRI’s • Anti-seizure medication – Gabapentin, etc. Chronic narcotic therapy • Indicated in patients if not operative candidates • Limited RCT evidence shows analgesia but not improved functional status • Requires clear understanding of duration and conditions of renewal • Longer duration analgesics preferred – MS Contin – Methadone, etc. Exercise • Aerobic exercise • Exercise more important than any specific maneuver • Dose (duration) matters • If possible, group reinforcement useful – Cognitive-behavioral therapy – Lay-led groups Hayden, Ann Intern Med 2006 What interventions work? • Surgery for selected patients in avoiding long-term leg pain after minimum of 6 weeks of symptoms • Active physical therapies - exercise - education • Receptive work environment • Medications have only a modest role • Early return to normal activities TC 2-1 What Doesn’t Work -Most modalities provide only transient relief -Traction is not useful •Corsets only occasionally useful •Spinal fusion has a “success” rate of 50% •Epidural steroids, etc. of transient benefit •Spinal manipulation of unclear benefit in chronic LBP TC 7-12 The physicians role • • • • • Evaluation Reassurance Symptom relief Encouragement of return to normal activity Appropriate referral