Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
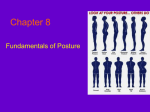
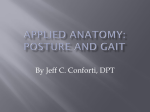
PODIATRIC GAIT ANALYSIS Southerland stated that ‘no other group of health care professionals spends as much time in their professional education learning “biomechanics.” Furthermore, ‘clinical gait evaluation is a fundamental skill for podiatric physicians.’1 Gait analysis forms part of the overall assessment of the locomotor system. The main objective of the overall assessment focuses on the position and alignment of the body and the relationship of the foot to the ground during gait. This involves discriminating between normal and abnormal gait indicators using visual or computerized gait analysis. Gait depends on the repeated Video capture from “The performance of the lower limbs of a effect of gait on Chronic sequence of motions that Musculoskeletal Pain.” Howard Dananberg DPM. simultaneously advance the body 1992. Langer Foundation for along a desired line of progression Biomechanics and Sports while maintaining a stable weight Medicine Research. bearing posture. In order for normal gait to occur a person must be able to accomplish the following four objectives: 1. Each leg must be able to support the body’s weight without collapsing. 2. Balance must be maintained, either statically or dynamically, during the single support phase. 3. The swinging leg must be able to advance to a position where it can take over the supporting role. 4. Sufficient power must be provided to make the necessary limb movements and to advance the trunk. The effectiveness of normal gait depends on free joint mobility and muscle action that is selective in both timing and intensity. Therefore, pathological conditions of the muscles, bones, joints, sensory nervous system, central motor control, and the cardiopulmonary system will alter the mode and efficiency of gait. With a detailed knowledge of normal function of the foot and lower limb, the chiropodist/podiatrist becomes able to identify the significant deficits of abnormal gait. THE FIVE COMPONENTS OF GAIT: 1. Source of motion Muscles provide force for desired motion. Muscle dependent on the nerve supply. Therefore, the source of motion is the motor unit. 2. Articulated levers The skeleton with its complex articulations and connecting ligaments provide the needed mobile lever system. Joint anatomy, dictates the directions motion can occur. Bone length proportionally magnifies the motor units’ actions. Fibrous tissue flexibility determines joint freedom of movement. 3. Awareness of motion needed Information is needed as to the position (proprioception), velocity, force and direction of motion. The information is continually sensed by peripheral receptors and transmitted by sensory pathways to neural control centres. 4. Control source to provide the desired motion Upper motor neurons arise from neural control centres that coordinate sensory input with anticipated motion. This results in muscles that contract with appropriate timing and intensity. There are numerous sites within the brain and spinal cord where a pathological process can introduce control deficits. 5. Energy to move Muscles use oxygen to generate energy needed for force production. Availability of an adequate oxygen supply depends on the state of the cardiovascular system. Classification of injury or disease of the structures essential for gait: 1. 2. 3. 4. 5. Structural Impairment - biomechanical etiology Motor Unit Insufficiency Combined Motor and Sensory Impairment Central Control Dysfunction Energy Lack The focus of this outline is the structural impairments (biomechanical) of the foot and lower limb and their affect on gait. During a normal gait cycle, the joints should be free to move and possess optimal joint alignment. This depends on fibrous tissue mobility, architectural accuracy of the bones and articular cartilage smoothness. This should be evaluated during a static biomechanical examination and if possible examined utilizing objective gait analysis techniques. The four remaining classifications which are important for the chiropodist/podiatrist to realize, but may not be identified until further investigation by a family physician, psychiatrist, or orthopaedic surgeon. This paper assumes these injuries are not present if the problem is of a biomechanical etiology. However, the discussion may point to these classifications as an alternative etiology for the gait problems observed. Power of Gait The power of gait is generated by the interplay of the factors in the flowchart outlined below: SOURCE OF POWER FOR WALKING Elastic Energy * Pendulum Action * Kinetic Energy Swing phase action Lever Effect of Stance Limb Heel, Ankle, and Forefoot Rocker Pull of swing limb Momentum Gravity Elastic energy response There are many muscles in the lower extremity that use eccentric muscle contractions to store potential energy to be utilized during a subsequent concentric muscle contraction as kinetic energy. The table below outlines the timing of eccentric and concentric muscle contractions of the flexors and extensors of the hip, knee, and ankle during the gait cycle. For example, the hip flexors stretch (eccentric contraction) and store elastic energy during single support and use the stored energy to initiate the concentric contraction occurring during preswing that powers the swing leg forward. Terminal Stance Pre Swing Ecc Conc Knee Flex Ecc Conc Ankle Pl. Ecc Conc Hip Ext Late Swing Ecc Loading Response Conc Mid stance Hip Flex Knee Ext Ankle Dors. Ecc Ecc Conc Early Swing Conc Ecc Conc The diagram to the left depicts the muscle activity during loading response to terminal stance. The hip extensors store potential energy during late swing phase and release kinetic energy during a very powerful concentric during the loading response phase. Diagram from Perry, J., “Normal and Pathological Gait, Disorders of the Foot Churchill and Livingstone, 1985. Energy Transfer The vertical displacement of the pelvis during stance allows for the exchange between kinetic energy and potential energy. This is illustrated in the diagram to the right. The diagram below illustrates when the exchange between potential and kinetic energy occurs in relation to the vertical ground reaction force graph Highest point of centre of body mass High Potential Energy 12.00 10.00 Lowest point of centre body mass High kinetic energy 8.00 Force N/KG 6.00 Vertical Ground Reaction Force 4.00 2.00 -2.00 Stride % 96 90 84 78 72 66 60 54 48 42 36 30 24 18 6 12 0.00 0 C of Mass Forward Progression Forward progression of the stance leg is accomplished by the lever effect of the stance leg. The progression of the stance leg can be stopped by any problem with either the heel, or ankle, or forefoot rockers. Lever Effect of Stance Leg Pull of swing limb and momentum The momentum of the swing limb helps with the progression of the stance leg and aids in the vertical displacement of the pelvis. Diagrams from Perry, J., “Normal and Pathological Gait, Disorders of the Foot Churchill and Livingstone, 1985 Conservation of Momentum The power of gait is really about the conservation of momentum. There is a dissipation of kinetic energy if stance leg and foot functions normally. If the power of motion is blocked for some reason this energy must be dissipated. The dissipation of energy occurs at the weakest link. Excessive STJ and MTJ pronation is a visible form of power dissipation. Requirements to conduct a gait analysis Upon completion of a static biomechanical examination, the chiropodist/podiatrist should get the patient to walk to observe any obvious or subtle changes from normal gait patterns. The data acquired from both the static examination and the gait analysis should correlate to give the chiropodist a total clinical picture. If possible, you can even correlate the static and vidio gait data to an F Scan/EMED Pedar test. The main problem while observing gait is to train your eye to focus in on problem areas within the whole kinetic chain from head to toe. Initially, you may need a video camera to detect these changes, but with repeated practice you can observe even the most subtle sagittal and frontal plane changes in gait with the naked eye. Most articles concerning gait analysis focus on the trunk, hips, knees and ankles, but fail to mention the area of the body the chiropodist is concerned with. This part of the outline will deal with the upper body, hips, knees and ankle, but will focus on the indicators of abnormal gait within the foot. The outline assumes knowledge of how the trunk, hips, knees, ankles and foot normally function during gait. The walkway • Hard surface, straight & level • Good lighting • Minimum length 8-12 m • The ability to view in both the frontal and sagittal planes • Minimum width 1.1 m • Can use treadmill plus/minus camera The patient • Shod & unshod with patellae visible • Clothing should be worn to make observations easy and • Needs to walk back and forth several times looking straight ahead and letting arms swing naturally • A bisection of the posterior calcaneus and posterior aspect of leg is often helpful to aid visualization • A mark on the medial side of the navicular is also helpful Patient walking speed • Many parameters of gait vary with walking speed (eg kinematics) • Controlling cadence reduces variability but may reduce the validity of the observations • Use own judgment e.g. athlete versus non-athlete The analysis • Requires a systematic and logical approach observing the gait patterns • Initially - gross review of gait to sense the ‘flow of action’ • Followed by specific analysis in the frontal & sagittal planes to identify significant gait deviations • Observe one segment at a time comparing R & L sides for symmetry of timing and joint positions • Start at the foot, and progressing sequentially upward (or vice-versa) • Separately observe events occurring during each of the periods of gait (e.g. contact, midstance, propulsion • Problem identification and subsequent treatment. Problem identification Finally, it may be helpful to remember that an abnormal or subtle change in gait may be performed for one of two reasons: 1. The subject has no choice, since the movement is forced upon them due to weakness spasticity or deformity. 2. The movement is a compensation which the subject is using to correct for some other problem which therefore needs to be identified. 3. May be observing effects not causes 4. The observed gait pattern is not the direct result of a pathological process, but the net result of a pathological process and the patient’s attempt to compensate for it’ (Whittle, 1996) INDICATORS OF ABNORMAL GAIT HEAD TILT AND SHOULDER DROP • • • • • • head tilt suggests a leg length difference (LLD) normally, the eyes should be level the position of the head depends on the amount of compensation in the spine for the leg length difference normally, the shoulders should be level if shoulder drop is present, this is suggestive of a LLD there are many combinations of head tilt and shoulder drop (Figure 1) lateral trunk bending may be observed. FIGURE 1 no compensation • cervical compensation partial thoracolumbar compensation complete compensation make sure the side of the shoulder drop has the lower hand, since right or left handedness can cause a rounding of the shoulder muscles producing an apparent shoulder drop. ARM SWING • arm swing reflects shoulder motion which reflects opposite pelvic rotation • increased arm swing on one side reflects, increased pelvic rotation on the other side • classically, if there is a LLD, the long leg will circumduct to prevent toe drag resulting in a greater arm swing on the side of the short leg. • the short leg has been observed to move excessively in keeping up with the step of the long leg, resulting in the arm swing being greater on the long side. ARM ABDUCTION AND ELBOW FLEXION • look for arm abduction, if present, this suggests an uncompensated or partially compensated LLD • the arm is held more abducted to increase inertia on the side of the long leg where the centre of gravity is deviated towards the short side • elbow flexion on one side decreases the moment of inertia of this side therefore increasing speed INCREASED LUMBAR LORDOSIS Many people have increased lumbar lordosis but it is only considered a gait abnormality if the lordosis is used to aid walking. Lordosis is usually observed from the side and generally peaks at the end of the stance phase on the affected side. http://www.seattlechildrens.org Common causes of increased lordosis • flexion contracture of the hip • hip joint immobility preventing the femur from extending from its flexed position -> extension of lumbar spine • imbalance between the hip extensors and abdominal muscles HIP HEIGHT • • • • • • • • • looking for signs of LLD or Trendelenberg’s gait place pants on hips evenly using the ASIS as your reference the ASIS may be uneven due to pelvic incongruities in this case, use the iliac crest levels as your reference when evaluating hips, look for a height difference from the front and back view structural LLD will show the longer limb higher at the hips on both views a functional LLD due to foot pronation on one side will show a drop in the anterior hip area and an elevation in the posterior hip area of the more pronated foot this is due to an anterior-posterior tilt around the hip joint with midstance pronation the combination of structural and functional is difficult to sort out visually TRENDELENBERG’S GAIT OR LATERAL TRUNK BENDING When standing on one leg, the centre of gravity (in front of S2) is brought over the weight bearing foot by the gluteal muscles on that side tilting the pelvis. The pelvic tilt results in elevation of the buttocks on the other side (Figure 2.A). The bending of the trunk towards the side of the supporting limb during stance phase is known as lateral trunk bending or Trendelenberg’s gait (Figure 2B). The purpose of this movement is to reduce the forces in the abductor muscles and the hip joint during single support stance. Trendelenberg’s gait can be applied to people with an antalgic gait or weak hip abductors. A positive Trendelenberg’s sign appears when the buttock on the nonPrimal Pictures weight bearing side fails to rise (Figure 2C). Lateral trunk bending is best observed from the front or back. During double support, the trunk is upright, however when the swing leg leaves the ground, the trunk will lean across towards the side of the stance phase leg (Figure 2B). This lateral trunk bending will end at the next double support phase if the problem is unilateral. If bilateral, there is a waddling gait with excessive shoulder sway. FIGURE 2 A. SINGLE STANCE Normal B. STABLE Lateral Trunk Bending C. UNSTABLE STANCE Inactive hip abductors Positive Trendelenberg’s Causes of Trendelenberg’s Gait 1. Painful hip • amount of pain in hip depends on the force transmitted through the joint • lateral trunk bending will reduce the total joint forces 2. Hip abductor weakness • hip abductors not able to contract with sufficient force to stabilize the pelvis during single support (positive Trendelenberg’s sign) • lateral trunk bending is employed to reduce the force that the hip adductors are attempting to oppose 3. Abnormal hip joint • congenital hip dislocation and coxa vara will lead to difficulties in stabilizing the pelvis • the effective length of the hip abductors is reduced because the greater trochanter of the femur moves upward toward the pelvic brim -> hip abductors contract with a reduced tension • this combination of reduced muscle length and tension is a powerful incentive to walk with lateral trunk bending 4. Unequal leg length • the pelvis tips downwards on the side of the shortened limb as the body weight is transferred to it • this exaggerated pelvic tilt is accompanied by a compensatory lateral bend of the trunk (Figure 1). 5. Wide walking base >100mm • a wide walking base may be caused by an abducted hip, a valgus knee, or the fear of falling • lateral trunk bending can be used to keep the centre of gravity over the supporting leg • a waddling gait results from this lateral trunk bending. SHORT LEG GAIT In order for natural walking to occur the stance leg needs to be longer than the swing phase leg. It this does not occur, the swing leg will collide with the ground. Conversely, if the stance leg is too long, it cause the swing leg to excessively reach before heel strike possibly causing a greater impact at heel strike. There are three types of short leg gait, each of which is caused by a different etiology: 1. Structural leg length difference is caused by a difference in bone length in either the femur or the tibia. 2. Functional leg length difference is usually caused by a neurological problem affecting the muscles of the hip, thigh, tibia and ankle. This results in the leg not being able to adjust to the appropriate length in either the stance phase or swing phase of gait. This occurs in a CVA patient. 3. Unilateral excessive pronation at the STJ due to a compensation for another problem will cause the leg to be shorter during its stance phase. This in turn causes the opposite swing leg to become much longer. Compensations for short leg gait: • • • • • head tilt shoulder tilt waist drop lateral trunk bending greater arm swing usually on short leg side • excessive internal rotation Swing phase adjustment (long leg) Stance phase adjustment (short leg) • • • • • • knee flexion hip flexion steppage circumduction equinus vaulting hip hiking COXA VALGA / VARA • • • check out distal 1/3 of femur normally 8° coxa vara compare with static examination HIP ROTATION The hip is able to make large rotation in the transverse plane to compensate for problems which the knee and ankle cannot compensate. Transverse plane hip compensations or problems results in a in-toed or out-toed gait. There are three causes of abnormal hip rotation: 1. Muscle weakness • • 2. spasticity or weakness of the muscles which rotate the femur about the hip joint cerebral palsy may include an element of internal or external rotation since there can be weak medial or lateral hamstrings. Foot placement problems • • 3. foot problems such as pes cavus or pes planus will produce abnormal rotation at the hip weak peroneals cause an inverted foot and a weak tibialis posterior cause an everted foot. Both these problems cause abnormal hip rotations. Compensatory hip rotation • • • external hip rotation can overcome weak quadriceps, this alters the line through the knee external hip rotation can be used to facilitate hip flexion using the hip adductors as flexors external rotation can be used to compensate for ankle equinus GENU VALGUM / VARUM • • check proximal 1/3 of tibia compare with static examination does middle of knee cap line up with the 2nd & 3rd toes during gait TRANSVERSE ROTATION OF KNEE • • • • • • • • Knee flexion at contact will cause the tibia to internally rotate (remember the screw home mechanism). Bisect the patella with big dot to visualize knee rotation. At heel contact, the knees/patella should be slightly external to neutral on the transverse plane. During stance, the knee should internally rotate 5° from the heel contact position of the knee. Try to develop the knack of observing the knee right at heel contact. Observe if the knee is functioning excessively internal or external, compared to your findings to the static hip rotation measurements. If hip rotation is normal on static, but knees are excessively external, look for an internal malleolar position or a short leg where the hip will externally rotate to compensate. Asymmetrical internal rotation signifies a functional or combined LLD where one foot is pronating more than the other. EXCESSIVE INTERNAL KNEE ROTATION • • Draw line down anterior middle aspect of shin, this allows for visualization of tibial internal rotation. Excessive pronation will hold the knee in its most internal position which results in delayed supination of the STJ and knee extension during terminal stance. EXCESSIVE KNEE FLEXION – EXTENSION Try to visualize sagittal knee motion at heel contact from a side view. At heel contact, the knee should be completely extended followed by 20° flexion to absorb shock of heel strike and to allow tibial internal rotation Effects of excessive knee flexion: • • • • uses up the available ankle joint dorsiflexion too soon therefore, this disrupts the ankle rocker mechanism. does not interfere with shock absorption may prevent normal extension of the knee during terminal stance with time you will observe excessive knee flexion by observing the lack of transverse skin creases just above the superior pole of the patella with incomplete knee extension Causes of excessive knee flexion: • • • • • • flexion contracture of the knee-hamstrings and gastrocnemius flexion contracture of the hip-iliopsoas spasticity of knee flexors, may cause anterior trunk bending since the quadriceps will be weak prevention of plantar flexion of the ankle during heel contact compensation for a long leg during stance compensation for functional hallux limitus Effects of excessive knee extension: • • • prevents shock absorption occurring with knee flexion at heel strike the knee may rock into hyperextended state (Genu recurvatum) may prevent ground clearance of the toes just after toe off Causes of excessive knee extension: • • • • • quadriceps weakness leading to anterior trunk compensation compensation for an equinus state in children quadriceps spasticity weakness in knee flexors causing excessive extension at heel lift compensation for a boney equinus in children Re-extension of the knee and hip during terminal stance is a very important event for the progression of the stance leg just before opposite heel strike. Video capture from “The effect of gait on Chronic Musculoskeletal Pain.” Howard Dananberg DPM. 1992. Langer Foundation for Biomechanics and Sports Medicine Research. SIGNS OF EXCESSIVE SHOCK TRAVELLING UP THE LEGS: Your best bet is to listen for the sounds of the feet for sounds of excessive pounding and observing the back of the patients shirt or neck area for abnormal shock waves. TIBIAL VARUM / VALGUM • • check distal 1/3 of tibia compare with static examination HEEL POSITION / MOTION – CONTACT • • • • • • if you see eversion of the calcaneus at contact, you are probably observing more than 5° of motion. observe the position of the calcaneus just before heel strike. evaluate if there is a high , low, or medially deviated STJ axis if you see a lot of STJ motion evaluate if there s a low STJ axis if there is a lot of talar bulge with hardly any STJ motion, evaluate if there is a high STJ axis if there is talar bulge with a lot of STJ motion, evaluate if there is medially deviated axis HEEL POSITION - MIDSTANCE/PROPULSION • Normally, the calcaneus should invert during midstance. • Look for signs of resupination. BASE OF GAIT • • • Measured from medial heel to medial heel. A wide base of gait is inefficient probably compensating for some instability. A narrow base of gait can cause an increase in rearfoot varus leading to shock absorption problems if the calcaneus cannot evert enough. • A wide base of gait sustains the pronatory torque at the STJ midstance since it takes longer to get the centre of body mass over the supporting leg. POSITION OF TOES • • • During contact, the proximal phalanges should be 5-10° dorsiflexed on the metatarsals. At midstance, the toes and the metatarsals should be parallel. If the proximal phalanges are dorsiflexed 5-10° or lesser, toe deformity is present from opposite side toe off to same side heel lift, this is a sign of forefoot instability. ABDUCTORY TWIST • • • • • • • • • • • • • • • Abductory twist is actually a misnomer; it was originally thought to be an abduction of the forefoot on the rearfoot secondary to STJ and MTJ pronation. In reality, this abductory twist is an adduction of the rearfoot after the heel rises. To understand the concept of abductory twist involves an understanding of pelvic rotation during midstance. During midstance, the pelvis begins to externally rotate from its most internal position. At the end of midstance (30% of stride), the foot should begin to supinate. If the foot remains pronated, it holds the tibia internally rotated while the femur externally rotates around the pelvis. Horizontal torque is produced at the knee. As the heel lifts, the pronated STJ can no longer hold the tibia in the extremely internally rotated. Only the friction in the area of the plantar forefoot is trying to prevent the external rotation. Therefore, the tibia and foot are forcefully and externally rotated around the metatarsal heads producing an abductory twist to the forefoot and adductory twist to the rearfoot. The STJ must be maximally pronated before an abductory twist occurs. This motion is exaggerated in uncompensated or partially compensated forefoot varus which requires abductory twist to allow the hallux to contact the ground in propulsion. Look for heel adduction at heel lift as the patient walks away from you. Does one foot have more abductory twist Watch the total motion of the whole twist not the end result. H. Dananberg has postulated that abductory twist is as a result of a sagittal plane blockade in the 1st MPJ. The avoidance of the 1st MPJ will result in the abductory twist as the person will follow the line of least resistance. This will result in the person using the low gear axis for toe off. ANGLE OF GAIT • • • Normally, the angle of gait is 7-10° abducted. Angle of gait is governed by the hip motion available, the amount of femoral or malleolar torsion present plus or minus the adduction or abduction of the whole foot on the body of the talus. The angle reflects the summation of these hip, femur, tibia and foot transverse plane measurements. • If this does not add up to the angle of gait, look for errors in the summation or the body is increasing the angle of gait for some other deformity, i.e. short leg. • During the swing phase of gait, the patella should remain within the sagittal plane. • If the patella during swing functions: 1. EXTERNALLY - external torsion of femur or an external positioned problem of the hip joint is present. 2. INTERNALLY - internal torsion of femur of an internal positioned problem of the hip joint is present. • The angle of gait during stance is primarily due to an external torsion of the tibia. If the knee, during swing, faces straight ahead but the: 1) angle of gait is increased, then an increased malleolar torsion is present. 2) angle of gait is decreased, then a decreased malleolar torsion is present. An abducted angle of gait (>10°), causes a pronatory torque at the moment of heel strike and is sustained through until propulsion. LATERAL ARCH • • • • • Excessive abduction of the forefoot on the rearfoot at the calcaneo- cuboid joint. Make sure a prominent styloid does not mislead you. Lateral side of the foot should lift up in one motion. In a badly subluxed calcaneo-cuboid due to an equinus state, the heel will rise first, then the cuboid/5th metatarsal next. This is suggestive of a rocker bottom foot. MECHANICS OF HEEL LIFT Prior to visual heel lift (42% of stride): 1. The knee becomes extended; the gastrocnemius muscle maintains flexor tension to prevent hyperextension. 2. The tibia accelerates in an anterior direction as the gastrocnemius, soleus and deep posterior decelerate the tibia. 3. The trunk moves forward over the stance foot shifting weight from heel to forefoot allowing the heel to gradually become non weight bearing until visible heel lift occurs. 4. The gastrocnemius, soleus, and deep posterior muscle group begin to decelerate ankle joint dorsiflexion as weight is relieved from heel. 5. The gastrocnemius contraction flexes the knee at opposite heel strike. 6. The tibia continues its forward momentum and ankle joint dorsiflexion is stopped. 7. Visible heel lift occurs at the point at which the eccentrically contracting gastrocnemius and soleus, overcomes the ankle dorsiflexion moment caused by forward tibial momentum and the centre of gravity posterior to the 1st MPJ. 8. Heel lift is dependent on 1st MPJ dorsiflexion Observation of Visual Heel Lift Visual heel lift is easier to observe relative to the swing leg, therefore, heel lift is early, normal or late as compared to the opposite foot. Normal heel lift should occur prior to heel contact of the opposite foot. Late heel lift occurs if there is a forefoot instability, therefore, heel lift on the stance side will be delayed until after contact of the opposite foot. Early heel lift generally occurs around the time when the opposite swing leg is passing the stance foot Early heel lift can be caused by an equinus state. Early heel lift can be: 1. double - severe gastrocnemius equinus 2. abrupt - classical 3. rolling - rocker bottom foot If an equinus state is not present Check to see if the following are present as they all lead to an early heel lift: 1. Cavus foot may limit ankle joint dorsiflexion since a high calcaneal inclination angle places the talar neck up against the anterior aspect of the tibial ankle mortise as the STJ supinates. 2. Neuromuscular disease may cause hyperinnervation of the calf muscles causing the heel to pop up earlier. 3. Osseous limitation at the ankle joint. 4. STJ axis deviated off sagittal plane if STJ axis becomes more perpendicular in rotation to the sagittal plane, more sagittal plane motion will be available. As STJ supination proceeds, more talar dorsiflexion will occur causing bone to bone contact. 5. Calf/Hamstring/Iliopsoas tightness • • • calf tightness limits ankle joint dorsiflexion hamstring tightness causes knee flexion which causes the tibia to tilt forward and uses up available ankle joint dorsiflexion iliopsoas tightness holds knee in flexed position tilts tibia forward and uses up available ankle joint dorsiflexion SIGNS OF RESUPINATION 1. Heel inversion • • difficult to observe with naked eye using video slow motion, not difficult to observe 2. Arch height elevation use navicular tuberosity as a point of reference 3. Tibial rotation • • tibial rotation easiest sign to observe if the tibia stays internally rotated throughout midstance, look for arch height elevation in propulsion 4. Plantar prominence of the first metatarsal head in propulsion • • • normally, the 1st metatarsal will plantarflex in terminal stance and preswing with STJ supination look for evidence of functional hallux limitus such as avoidance or low gear toeoff this must be distinguished from plantar flexion of the 1st metatarsal on the hallux If no resupination occurs during propulsion, combined with a vertical or low gear toe off, the gait is deemed appropulsive. Watch for resupination in swing phase, if no resupination is observed in midstance or propulsion but the calcaneus everts during contact. Check if one side stayed pronated longer. PATHOLOGICAL GAITS Earlier, I stressed that this outline would focus on the structural impairment, which may affect foot during gait. Motor unit insufficiency, combined motor and sensory impairment central control dysfunction and energy lack were not discussed. The following types of pathological gaits can be classified into one of the above 5 classifications. ANTALGIC GAIT • avoidance of pain from ambulation • quick soft steps SPASTIC GAIT • unbalanced muscle action leading to deformity • scissor like gait where there is adduction and internal rotation of hips • with an equinus of the feet and flexion at the knees ATAXIC GAIT Spinal: • • • • • proprioceptive pathways of spine or brainstems are interrupted loss of position and motion sense wide base of gait may slap feet at heel contact must watch feet Cerebellar: • • • coordinating functions are interfered with wide base of gait unsteady irregular gait PARKINSONIAN GAIT • trunk bent forward • legs and arms are stiff • short steps with shuffling • centre of gravity is being chased PARALYTIC GAIT • muscle paralysis or weakness due to nerve, muscle, osseous pathology body weight used to provide the pull or stabilization needed Gluteus medius lurch • Trendelenberg’s gait in which the truck shifts over to the side of weak muscle when in stance • minimizes fall of swing phase side of pelvis Gluteus maximus lurch • trunk lurches back on stance side hyperextending • the purpose of the posterior truck bending is to compensate for ineffective hip extensors during stance. Posterior trunk bending produces an external extension moment on the hip Hip flexors • trunk moves back on the affected side as that side leaves stance • gives momentum to swing phase • also used if the knee is unable to flex (anterior trunk bending) Quadriceps • trunk moves forward on the stance phase side in an effort to keep the knee in extension for weight bearing • anterior trunk bending produces an external extension moment on the knee Ankle dorsiflexors • drop foot gait, steppage gait • knee must be brought higher during swing to allow for ground clearance Triceps • no propulsion for toe off STIFF KNEE GAIT Limb must swing outward in semicircular movement for foot to clear the ground. Stance limb may go up on toes spastic hemiplegia. PSYCHOGENIC GAIT Astasia abasia Comptocormia unable to stand or walk without assistance, but have normal use of legs in supine position. functional bent back syndrome. Both are termed conversion hysterias. There is some underlying psychological problem which causes gait disturbance. Usually dramatic results once the psychological problems have been resolved. REFERENCES 1. Blake, R.L., “Evaluation of Gait”, J. Amer. Pod. Med. Assoc., 1981 71:6, 341. 2. Blake, R.L., “Positives in Biomechanical Gait Evaluation”, 3rd year Clinical Notes, California College of Podiatric Medicine, 1985. 3. Levy, L.A., Heatherington, V.J., “Principles and Practice of Podiatric Medicine”, Churchill Livingstone, 1990. 4. McRea, R., “Clinical Orthopaedic Examinations”, 2nd ed., Churchill Livingstone, 1983. 5. Morris, J. and Scherer, P., “Pathomechanics Syllabus”, California College of Podiatric Medicine, 1991. 6. Perry, J., “Normal and Pathological Gait, Disorders of the Foot”, Chapter 5, Churchill and Livingstone, 1985. 7. Robins, J., “Clinical Handbook of Podiatric Medicine”, 2nd ed., Ohio College of Podiatric Medicine, 1983. 8. Orien, W.P., Root, M.L., Weed, J.H., Clinical Biomechanics Volume II, “Normal and Abnormal Function of the Foot”, Clinical Biomechanics Corporation, 1977. 9. Seibel, M.O., “Foot Function”, William and Wilkins, 1988. 10. Turlik, M., 2nd year Biomechanics Notes, Ohio College of Podiatric Medicine, 1990. 11. Whittle, M., “Gait Analysis, An Introduction”, Butterworth Henemann, 1991. 1 Valmassy R.L : Clinical Biomechanics of the Lower Extremities , St. Louis, 1996, Mosby, Chapter 7, pp. 149. Gait evaluation in clinical biomechanics, by C.C. Southerland, Jr.