Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
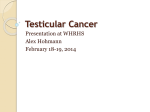
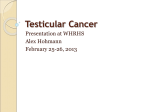
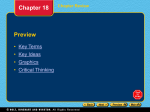
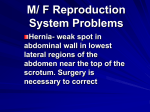
284jumonline.qxp:Layout 1 3/17/09 2:30 PM Page 549 Case Report False Diagnosis of Ruptured Testes in a Case of Traumatic Dislocation Caroline A. Kilian, BS, David A. Paz, MD, Sameer A. Patel, MD, Matthew J. Austin, MD, Katherine M. Richman, MD, Dolores H. Pretorius, MD T esticular trauma can be a surgical emergency, and in general, surgical intervention must be performed within 3 days of the trauma for testicular salvage.1,2 Both sonography, with and without color Doppler imaging, and computed tomography (CT) are useful diagnostic tests to evaluate the scrotal contents and abnormalities. Straddle injuries, often from motorcycle accidents, can rarely cause testicular dislocation and are usually accompanied by scrotal hematoma and pelvic fracture.3 With abdominal CT and color Doppler sonography, the dislocated testicle and its blood flow are usually located, although at the initial time of injury, they may go undetected.3 Victims typically are in their second and third decades of life, and the dislocation is most likely secondary to accidental trauma. We present a case in which a patient was thought to have shattered testes and was emergently taken to the operating room, where the testes were found to have normal blood flow bilaterally but to be displaced superiorly by a scrotal hematoma. Case Report Abbreviations CT, computed tomography Received October 16, 2008, from the University of Arizona, Tucson, Arizona USA (C.A.K.); and Department of Radiology, University of California, San Diego, La Jolla, California USA (D.A.P., S.A.P., M.J.A., K.M.R., D.H.P.). Revision requested November 7, 2008. Revised manuscript accepted for publication November 25, 2008. Address correspondence to Dolores H. Pretorius, MD, Department of Radiology, University of California, 9300 Campus Point Dr, 7756, La Jolla, CA 92037 USA. E-mail: [email protected] A 22-year-old Mexican man was making an illegal attempt at crossing the Mexican border into the United States when he landed on a metal pipe, had a probable straddle injury, as evidenced by perineal blood, and was initially seen at a clinic on the border. He was transferred to the trauma bay at our institution, where physical examination revealed a large scrotal hematoma. Initial urinalysis results were negative for blood, and a retrograde urethrogram revealed no evidence of active extravasation. Pelvic CT revealed a large scrotal hematoma and air consistent with a right pneumohemiscrotum. Further evaluation with sonography revealed a band of hypoechoic material extending bilaterally with trace to no internal flow and hyperemic scrotal skin (Figure 1); initially this was thought to represent shattered testes. In retrospect, the testes were not in the images provided because of their displacement superiorly. © 2009 by the American Institute of Ultrasound in Medicine • J Ultrasound Med 2009; 28:549–553 • 0278-4297/09/$3.50 284jumonline.qxp:Layout 1 3/17/09 2:30 PM Page 550 False Diagnosis of Ruptured Testes in Traumatic Dislocation Figure 1. Sonography of the scrotum. A, Sagittal image showing a hypoechoic structure in the scrotum measuring 6.1 × 2.9 cm, which was originally thought to represent the left shattered testicle. B, Transverse midline view of the same region as shown in A revealing that the hypoechoic structures seen on both sides actually connect and reside within the scrotal skin rather than the scrotal sac. C, Color Doppler image of same area as in B showing minimal flow within the hypoechoic structures. No images were actually able to show intact testes. A Urologic exploration for possible orchiectomy revealed a scrotal hematoma with small but otherwise normal testes bilaterally and no damage to the spermatic cord. Both testes were delivered back into the scrotum after copious irrigation, and the scrotum was closed. The patient was ambulating the next day and was discharged with narcotic pain medication and a Foley catheter with a leg bag, and outpatient follow-up was scheduled. In reviewing the CT scan and additional reformatted images, the testes were present within the inguinal areas, measuring 3.8 × 2.8 × 2.2 cm on the right and 3.7 × 2.7 × 2.2 cm on the left (Figures 2–4). Discussion B C 550 Terminology used to evaluate patients with testicular trauma includes testicular rupture, fractured/shattered testicle, testicular hematoma, testicular hematocele, testicular avulsion, and dislocated testes. Mimickers of testicular rupture include a massive extratesticular hematocele and an intratesticular hematoma.4 Additionally, these mimickers can accompany traumatic testicular dislocation. In the setting of large swelling and hemorrhage, it is not always clear whether the trauma has led to rupture of the tunica albuginea of the testes or damage to the scrotum. It is known that testicular rupture occurs in 50% of patients with traumatic hematocele.5,6 Sonography has traditionally been the primary tool used for evaluation of testicular trauma because of low cost, portability, accessibility, lack of ionizing radiation to the area, the multiplanar approach, the real-time nature, and the ability to assess for blood flow with color and pulsed Doppler imaging. Sonography is used to evaluate all of the scrotal contents, but the testes must be in the field of view to make an accurate diagnosis. The sonographer must scan the entire scrotum and the inguinal regions to look for the testes; this was not done in the case presented here because the scrotum was large and filled with blood, and it was thought that the testes were ruptured. Absence of a normal testis and mixed echogenic debris imaged within the scrotum should suggest fragments of a shattered testis.7 Color Doppler imaging should be used to assess for testicular blood flow, even in fragments, to assess for possiJ Ultrasound Med 2009; 28:549–553 284jumonline.qxp:Layout 1 3/17/09 2:30 PM Page 551 Kilian et al A B Figure 2. Contrast-enhanced CT of the lower pelvis. A, Axial image at the level of the lower pelvis showing an enlarged scrotum with heterogeneous attenuated fluid noted within the scrotal skin as well as hematoceles (arrow). B, Axial image more cephalad showing ovoid soft tissue densities in the subcutaneous tissues of the groin, representing superiorly dislocated testes (arrows). ble salvage.7 Guichard et al8 studied 22 cases of testicular fracture with 6 false-positive results, as was seen in our case. The specific sonographic criteria used to diagnose testicular rupture/ fracture in their series included heterogeneous parenchyma, loss of contour definition of the testis, and a breached tunica albuginea.8 Color Doppler sonography is also useful for diagnosing testicular dislocation; however, the sonographer must image the inguinal regions to identify the testes.3 Lack of blood flow can be seen in a hematoma or an infarction as well as in testicular rupture by detecting a disruption in the normal capsular blood flow of the tunica vasculosa.4 Figure 3. Reformatted CT. A, Magnified coronal reformation showing an enlarged scrotum with a large hematoma in the skin as well as hematoceles (short arrow). The testes reside superiorly in the subcutaneous tissues of the groin (long arrows). B, Magnified parasagittal reformation showing superiorly located testes (long arrow), likely secondary to a trauma-induced spasm of the cremasteric muscle. Note the fluid-filled scrotum (short arrow) that correlates with the hematoma seen on sonography. A J Ultrasound Med 2009; 28:549–553 B 551 284jumonline.qxp:Layout 1 3/17/09 2:30 PM Page 552 False Diagnosis of Ruptured Testes in Traumatic Dislocation Figure 4. Surface-rendered 3-dimensional CT reformation showing contour abnormalities in the regions of both subcutaneous tissues of the groin (arrows), representing the testes dislocated superiorly. Multiplanar reformatted images from CT offer great potential in evaluating patients with trauma; however, there are currently only a few cases reported in the literature describing the benefits of this new technology. Reformation techniques have been used in evaluating for skeletal trauma; however, they have only recently been used to evaluate the abdomen and pelvis.3,9–12 In the case presented here, the reformatted images were very helpful in retrospectively diagnosing the type of scrotal injury and in better understanding the relationship of the testes, scrotum, and inguinal region (Figures 3 and 4); this has also been reported by Ezra et al.5 Unfortunately, the reformatted images in this case were obtained after the patient had been taken to the operating room, and we suspect that if they had been obtained initially, the dislocation of the testes would have been identified. Testicular dislocation is relatively uncommon, having been reported in approximately 75 cases before 20085; it occurred only once in 33 men with scrotal trauma in a series reported by 552 Guichard et al.8 Ko et al13 reported that testicular dislocation was initially missed in 9 patients with groin trauma. Testicular dislocation, initially described in 1936 by Herbst and Polkey, is most frequently associated with straddle injuries, yielding superolateral displacement secondary to a mass effect.14 In motorcycle trauma, as in our case, the traumatic impact of the gasoline tank is the most common culprit, with most dislocations occurring immediately, although it may progressively develop over days to weeks and rarely reduces spontaneously. Dislocation may be unilateral or bilateral, may be deep or superficial, may include torsion of the spermatic cord, and may have migration of the dislocated testis to the abdomen in the setting of an inguinal hernia.8,14 Ezra et al5 reported that the ductus deferens, spermatic veins, and testicular artery may also be dislocated with the testis. A spasm of the cremasteric muscle has been implicated as a contributing factor to testicular dislocation, as well as underlying anomalies (a wide external ring, an indirect inguinal hernia, and atrophic testes) that can be additional predisposing factors.3 Additionally, undescended testes, whether preexisting or due to a trauma-induced spasm of the cremasteric muscle, should be discovered before surgery. Clinical assessment of dislocation often begins with the physical examination, which reveals a palpable painful mass in the inguinal, prepubic, or crural location, but severe trauma with pain and altered anatomy can often limit reliability. Tsai et al3 suggested that it is important to look for dislocation and rupture of the testes when there is a scrotal hematoma because hematoceles and hematomas are common injuries that accompany testicular dislocation. Imaging studies used for evaluation include sonography and CT, as discussed above. Urologic consultation and early reduction is recommended, as was performed in this case. This is important to prevent sequelae such as infertility and histologic malignant changes.3 In conclusion, sonography has traditionally been the primary mode of diagnosis for scrotal trauma; however, the use of CT (with 3-dimensional reformatting) may be helpful in improving the accuracy of posttraumatic scrotal diagnosis. Hematoceles and hematomas often accompany J Ultrasound Med 2009; 28:549–553 284jumonline.qxp:Layout 1 3/17/09 2:30 PM Page 553 Kilian et al testicular dislocation but may also mimic the injury. Straddle injuries can cause testicular dislocation that, without the use of proper imaging modalities, can be confused with testicular fracture or a shattered testis. Coupling sonography and CT can yield a more accurate and rapid diagnosis, thereby minimizing posttraumatic sequelae with an increased likelihood of testicular salvage. References 1. Gross M. Rupture of the testicle: the importance of early surgical treatment. J Urol 1969; 101:196–197. 2. Cass AS. Testicular trauma. J Urol 1983; 129:299–300. 3. Tsai HN, Wu WJ, Huang SP, et al. Bilateral traumatic testicular dislocation: a case report. Koahsiung J Med Sci 2002; 18:95–98. 4. Kim SH, Park S, Choi SH, Jeong WK, Choi JH. Significant predictors for determination of testicular rupture on sonography: a prospective study. J Ultrasound Med 2007; 26:1649–1655. 5. Ezra N, Afari A, Wong J. Pelvic and scrotal trauma: CT and triage of patients. Abdom Imaging 2008. http://www. springerlink.com/content/rk020614510l4574/fulltext.pdf. 6. Munter DW, Faleski EJ. Blunt scrotal trauma: emergency department evaluation and management. Am J Emerg Med 1989; 7:227–234. 7. Wittenberg AF, Tobias T, Rzeszotarski M, Minotti AJ. Sonography of the acute scrotum: The four T’s of testicular imaging. Curr Probl Diagn Radiol 2006; 35:12–21. 8. Guichard G, El Ammari J, Del Coro C, et al. Accuracy of ultrasonography in diagnosis of testicular rupture after blunt scrotal trauma. Urology 2008; 71:52–56. 9. Lawrentschuk N, Bolton DM. Occult renal segmental arterial injury after trauma. Urology 2005; 65:386–387. 10. Rees O, Mirvis SE, Shanmuganathan K. Multidetector-row CT of right hemidiaphragmatic rupture caused by blunt trauma: a review of 12 cases. Clin Radiol 2005; 60:1280– 1289. 11. Radwan MM, Abu-Zidan FM. Focussed Assessment Sonograph Trauma (FAST) and blunt abdominal trauma: surgeon’s perspective. Afr Health Sci 2006; 6:187–190. 12. Goodman DA, Tiruchelvam V, Tabb DR, Agarwal N, Rhoads JE Jr. 3D CT reconstruction in the surgical management of hepatic injuries. Ann R Coll Surg Engl 1995; 77:7–11. 13. Ko SF, Ng SH, Wan YL, Testicular dislocation: an uncommon and easily overlooked complication of blunt abdominal trauma. Ann Emerg Med 2004; 43:371–375. 14. Dondelinger R. Imaging and Intervention in Abdominal Trauma. New York, NY: Springer; 2004. J Ultrasound Med 2009; 28:549–553 553