Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
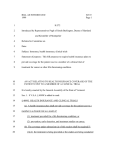
The new england journal of medicine editorials Controlling Research Trials Jeffrey M. Drazen, M.D. Clinical research, especially in the form of large multicenter trials, promotes changes in practice; without the accrual of new knowledge, clinical care will not advance. A deadlock between the National Heart, Lung, and Blood Institute (NHLBI) and the Office of Human Research Protections (OHRP) of the Department of Health and Human Services about the ethics of a clinical trial has the potential to bring much clinical research to a halt. The trial in question is designed to examine the ability of intravenous-fluid management directed by physiological data obtained from a pulmonary-artery catheter to influence outcomes in medical intensive care units. At the request of the OHRP, this trial has been on clinical hold since July 2002. To have a clear sense of the issues at play, it is important to understand the process by which trials sponsored by the National Institutes of Health (NIH) are designed and implemented (Fig. 1). When members of the medical community note a clinical problem that is in need of better research data, they bring it to the attention of appropriate members of the NIH staff. If the problem appears to be important, the staff members draft a request for research proposals and submit it for evaluation by the advisory council of the sponsoring institute. At this stage, there are often many competing proposals, and only the most meritorious survive. The successful proposals are modified to reflect the critique of the advisory council and are advertised to the scientific community in the NIH Guide.1 Interested investigators then compete to participate in the trial on the basis of a specific trial design, past success in trials of a similar nature, and a plan for recruiting patients into the trial. A review committee is convened, and the best groups are chosen. Before any funds are awarded, NIH staff members seek final approval of the program from their advisory councils. The selected investigators meet, debate, and finally agree on a trial design that will answer the clin- n engl j med 348;14 ical questions that have been posed in a way that adheres to best practices. Once the investigators have what they believe to be an optimal trial design, a committee of independent investigators reviews and critiques the specific proposal. This is not a rubber stamp but a tough review. Every point of the trial design is examined closely. More often than not, aspects of the trial need to be rethought to ensure that the data obtained will be clinically useful and that the trial will provide the greatest margin of safety for the patients who will be the research subjects. I know that these committees are tough; I have had a number of proposed research trials sent back for redesign and some scrapped altogether. Everyone involved takes the job — designing a trial that advances the art while ensuring patient safety — very seriously. When the pretrial review ends, the ongoing review begins. Once the trial has been approved, the NIH appoints a data and safety monitoring board that oversees the trial as it is performed. This body provides another layer of review to ensure that the scientific questions are valid, that the patients in the trial receive appropriate treatment, and that the results that emerge as the trial proceeds are analyzed to make certain that the level of risk incurred by participants remains acceptable as new knowledge develops both within and outside the trial. Some of the issues raised by the fact that research subjects are also patients are debated by Miller and Rosenstein2 and by Grunberg and Cefalu3 in this issue of the Journal. After the successful completion of these multiple levels of review (Fig. 1), another review process is held at the local level before the investigators can actually start the work. Individual investigators prepare protocols and consent forms for their institutional review boards (IRBs). Each IRB examines the protocol to be sure that the information to be gleaned from the trial is worth the risk to the sub- www.nejm.org april 3, 2003 1377 The new england journal of medicine Scientific community Idea for research trial Nonmeritorious ideas rejected NIH staff Refines idea and prepares report Nascent Idea NIH Advisory Council Many ideas rejected Examines multiple ideas Advises staff on importance RFAs posted for investigators Investigators respond Review committee evaluates Investigator Competition Proposals returned to Advisory Council for 2nd level of review Investigators not funded Investigators funded Investigators Write Protocol Investigators meet and write definitive protocol Revisions Protocol reviewed by protocolreview committee Final protocol Data safety and monitoring board Initial and ongoing review Implementation Phase IRB approval and monitoring at each site Trial Figure 1. Process of Design, Review, and Approval of Clinical Trials. NIH denotes National Institutes of Health, RFA request for applications, and IRB institutional review board. 1378 n engl j med 348;14 www.nejm.org april 3, 2003 editorials jects who will be participating in it. In the case of patients in the intensive care unit, who are often unable to participate in consent, there are special considerations, as noted by Karlawish4 in this issue of the Journal. The IRB also ensures that the risks are clearly spelled out in the consent document that the patients, or their surrogates, will sign as they complete the transition from patients to patientsubjects. Only when IRB approval is obtained can the trial begin. A trial that makes it through these multiple levels of scrutiny must have merit. The process is designed to ensure that the question to be answered is a clinically meaningful one, that equipoise exists, and that the patients participating in the trial are fully informed about the risks and benefits of that participation. At every level, reviewers are asked to be sure that there is appropriate and adequate protection in place for the human subjects who volunteer to participate. The information derived from the completed trials often sets the direction for clinical decision making for many years to come. Thus, the recent action by the OHRP with respect to the trial of the Acute Respiratory Distress Syndrome (ARDS) Network of the NHLBI is troubling. As reported by Steinbrook5 in this issue of the Journal, the NHLBI, at the request of the OHRP, has put on clinical hold an ongoing ARDS Network trial and is reexamining a completed trial.6 The primary reason for stopping the research is the contention, by investigators not associated with the trial, that the patients in both the completed trial and the ongoing trial have been and are subject to increased risk because one patient group did not receive and is not receiving care according to the “best current standard of practice.”7 The NHLBI has taken these criticisms very seriously, commissioning an independent blue-ribbon panel of five experts — four American and one Canadian — who examined both the completed and the ongoing ARDS Network trials. The panelists unanimously concluded that the trials were scientifically sound, that the results were important for the critical care community, and that the concerns that led to the placement of the trial on clinical hold were not valid. There is always some cause for concern when results of different trials are compared, but in the completed ARDS Network trial — a trial comparing mechanical ventilation using lower and higher tidal volumes — the mortality in the group receiving the larger tidal volume (the group that did less well) was similar to the mortality that would n engl j med 348;14 be expected on the basis of the known severity of their illness. This finding vitiates the argument that patients in the completed trial were put at increased risk. Although the NHLBI convened the blue-ribbon panel, it did so with the advice and consent of the OHRP. On receiving and reviewing the report of these experts, Dr. Claude Lenfant, director of the NHLBI, called the OHRP to say that he wanted to restart the trial. He was told to keep it on hold. Subsequently, the OHRP sent a 29-page letter to the institutions participating in the ARDS Network requesting reams of data concerning the original ARDS Network trial. As of this writing, the uncompleted trial is still on hold. This series of events represents more than a spat between the NHLBI and the OHRP. The action by the OHRP has far-reaching implications for all government-sponsored clinical research. If someone somewhere is unhappy with the design of a clinical trial, he or she could conceivably stop that trial by complaining to the OHRP that it, as designed, places the human subjects involved at increased risk. This foray into the scientific review of a protocol represents new territory for the OHRP. The role of the OHRP is to ensure that the process of research is carried out in accordance with statute and regulation.8,9 The office oversees the function and performance of individual IRBs and the process of informed consent, and it investigates when there is reason to believe that procedures with respect to the protection of human subjects from risks associated with research have not been appropriately followed. The OHRP has done much to restore confidence in the system of IRB review and to foster the integrity of the clinical-research system.10 The NIH has an established record of designing, reviewing, and monitoring clinical trials; it has the scientific expertise and the staffing to assume responsibility for the appropriateness of trial design. If there is concern about the safety of human subjects that derives from the conduct of the trial, rather than from the design of the research, the OHRP should investigate the complaint. Concern about the safety of human subjects that derives from the design of the trial is an issue for the NIH. These are separate and distinct roles. When there are legitimate disagreements among members of the scientific community about trial design with respect to the safety of the human subjects enrolled in the trials, the NIH and the OHRP www.nejm.org april 3, 2003 1379 The new england journal should develop mechanisms to assess the validity of these disagreements and to act accordingly. The methods used to resolve the dispute must be well defined, transparent, and time-sensitive. As a case in point, more lives could well be lost because of the extended interruption of the ARDS Network trial by the OHRP and the resultant delay in getting critical new information to the scientific community than would be saved through a redesign of the trial. The OHRP and the NIH should use their distinct strengths to further the common goal of accruing the knowledge we need to deliver the best care to our patients. Dr. Drazen serves as a member of the National Heart, Lung, and Blood Institute Advisory Council. 1. Office of Extramural Research. NIH guide for grants and con- tracts. Bethesda, Md.: National Institutes of Health, 2003. (Accessed March 14, 2003, at http://grants1.nih.gov/grants/guide/index.html.) 2. Miller FG, Rosenstein DL. The therapeutic orientation to clinical trials. N Engl J Med 2003;348:1383-6. of medicine 3. Grunberg SM, Cefalu WT. The integral role of clinical research in clinical care. N Engl J Med 2003;348:1386-8. 4. Karlawish JHT. Research involving cognitively impaired adults. N Engl J Med 2003;348:1389-92. 5. Steinbrook R. How best to ventilate? Trial design and patient safety in studies of the acute respiratory distress syndrome. N Engl J Med 2003;348:1393-401. 6. The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000;342:1301-8. 7. Eichacker PQ, Gerstenberger EP, Banks SM, Cui XZ, Natanson C. Meta-analysis of acute lung injury and acute respiratory distress syndrome trials testing low tidal volumes. Am J Respir Crit Care Med 2002;166:1510-4. 8. Assurances and IRB registration. Rockville, Md.: Office for Human Research Protections, 2003. (Accessed March 14, 2003, at http://ohrp.osophs.dhhs.gov/irbasur.htm.) 9. Compliance oversight. Rockville, Md.: Office for Human Research Protections, 2002. (Accessed March 14, 2003, at http://ohrp.osophs. dhhs.gov/compovr.htm.) 10. Putney SB, Gruskin S. Time, place, and consciousness: three dimensions of meaning for US institutional review boards. Am J Public Health 2002;92:1067-70. Copyright © 2003 Massachusetts Medical Society. Aldosterone Blockade and Heart Failure Mariell Jessup, M.D. In the fall of 1999, a multicenter, randomized trial examining the effect of spironolactone on morbidity and mortality among patients with severe heart failure was published in the Journal.1 The Randomized Aldactone Evaluation Study (RALES) proved that antagonism of aldosterone had an important role in the management of heart failure, even in patients taking angiotensin-converting– enzyme (ACE) inhibitors. In addition to reducing mortality by 30 percent, small doses of spironolactone resulted in an improvement in ventricular function and enhanced exercise tolerance.2 The rates of death from progressive heart failure and sudden death from cardiac causes were both diminished by an old, inexpensive medicine. This remarkable study has led to intensified research into the mechanisms whereby aldosterone blockade benefits patients with heart failure, to widespread use of spironolactone in a range of patients with heart failure, and to a new trial involving a novel aldosterone antagonist, eplerenone.3 Now is a good time to review the reasons why aldosterone blockade may be effective and the types of patients in whom it should be used. Aldosterone was originally thought to be important in the pathophysiology of heart failure only insofar as it increased the retention of sodium and 1380 n engl j med 348;14 the loss of potassium. It was also believed that optimal doses of ACE inhibitors would suppress the production of aldosterone, since angiotensin II is a potent stimulus for adrenal aldosterone secretion. In fact, both angiotensin II and aldosterone ultimately escape the effects of long-term ACE inhibition, with aldosterone levels showing a more pronounced rebound.4 Plasma aldosterone concentrations may reach 20 times the normal level in patients with heart failure, because of both increased production and a decreased rate of hepatic clearance. In addition to being produced by the adrenal glands, aldosterone is synthesized by human vascular cells and has a number of adverse effects on the vasculature.5 Sustained elevations of angiotensin II and aldosterone concentrations induce abnormal vasomotor reactivity and baroreceptor responsiveness by promoting endothelial dysfunction and oxidative stress. Moreover, intense interest has focused on the role of aldosterone in promoting organ fibrosis. A survival benefit among patients receiving spironolactone in RALES was associated with a reduction in the concentrations of serum markers of collagen synthesis. These and numerous other findings, as reviewed recently,6 emphasize the importance of tissue collagen turnover and fibrosis in heart failure as critical components in cardiac remodeling. www.nejm.org april 3, 2003