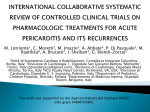
Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
CARDIOCHIRURGIA P46 MARKERS OF BRAIN INJURY IN CHILDREN BEFORE AND AFTER CARDIOPULMONARY BYPASS D. Bertini 1, M. Padalino 2, C. Ori 1, G. Lamonica 2, M. Simonato 2, D. Pittarello 2, S. Pecoraro 2, V. Vida 2, G. Stellin 2, P.E. Cogo 3 1 Department of Medicine, Anesthesiology and Intensive Care Unit, Padua, 2 Pediatric and Congenital Cardiac Surgery, University of Padua, Padua, 3 DMCCP, Ospedale Pediatrico Bambino Gesù, Roma, ITALY Scopi della ricerca. The increased survival of children with congenital heart disease (CHD) undergoing corrective surgery is associated with long-term neurocognitive deficits in medium and long term. The aim of the study was to determine if three specific markers of brain damage, Glial Fibrillary Acidic protein (GFAP), Phosphorylated Neurofilament Heavy Chain (pNF-H) and Ubiquitin C-terminal hydrolase 1 (UCHL-1), were altered after cardiopulmonary bypass (CPB) run, trying to figure out whether there were differences between cyanotic patients, and children with non-cyanotic or univentricular heart. Metodi Impiegati. GFAP is an intermediate filament protein, expressed by numerous cell types of Central Nervous System (CNS), including astrocytes, which is involved in many processes, including cell communication and the functioning of blood brain barrier. GFAP has also been shown to be important in repair after CNS injury. pNF-H is a neurofilament belonging to Class IV of the Intermediate family (IF) protein and is limited in axons. It has been evaluated as a biomarker of neurodegeneration. UCHL-1 is a deubiquitinating enzyme highly specific to neurons and to cells of the neuroendocrine system. We studied 33 children with CHD without chromosomal abnormalities. We correlated the above mentioned markers with features and timing of surgical procedures and physiological parameters of organs and cerebral perfusion. Infants were divided into 3 groups: 1) cyanotic (when preoperative arterial saturation was < 90%) (Number=14) 2) Not cyanotic (number=12) and 3) univentricular heart (number=7). We collected blood samples from superior vena cava before and after CPB, before the modified ultrafiltration. Neurological markers were assessed by ELISA. Cerebral O2 saturation, mixed venous saturation, arterial oxygen tension, and clinical and hemodynamic parameters were recorded. In 8 children we measured the neuromarkers also at the end of hypothermia, and rewarming phases. Risultati e Conclusioni. GFAP and UCHL-1 blood levels were significantly higher after CPB when compared with the preoperative values (p<0.05). GFAP was significantly higher in the cyanotic group (p<0.05). Time on CPB significantly correlated with GFAP and pNF-H levels after CPB (R=0.44, p=0.01; R=0.43, p=0.01). A tendency to increase with prolongation of cross clamp time is demonstrated for GFAP and pNF-H biomarkers (R=0.39, p=0.03; R=0.45, p=0.01). Time spent on hypothermia significantly correlated with GFAP levels after surgery (R=0.54, p=0.002), while degree of hypothermia was inversely correlated with pNF-H (R=0.35, p=0.05). The evaluation of markers behavior during different CPB phases established higher concentrations of pNF-H and UCHL-1 at the end of CEC. Values remained almost constant at the end of hypothermia and of warming time. Conclusions. CPB was associated with a marked elevation of brain injury markers; the glial damage markers were more elevated in cyanotic children. The damage depended on CPB duration and degree and time spent on hypothermia. A follow up of neurocognitive challenges of our patients is needed to integrate clinical data to laboratory results. P47 FATTORI PREDITTIVI DI SANGUINAMENTO E TRASFUSIONE DI EMODERIVATI DOPO INTERVENTO CARDIOCHIRURGICO IN BAMBINI AFFETTI DA DIFETTI SETTALI E TETRALOGIA DI FALLOT E. Bonafiglia 1,3, P. Biban 2, B. Ficial 1, C. Ng 3 1 Patologia e Terapia Intensiva Neonatale, Azienda Ospedaliera Universitaria Integrata, Verona, 2 Pediatria e Terapia Intensiva Pediatrica, Azienda Ospedaliera Universitaria Integrata, Verona, ITALY, 3 Cardiac Intensive Care Unit, Great Ormond Street Hospital, University College London, London, UNITED KINGDOM SCOPI DELLO STUDIO Il sanguinamento a seguito di interventi a cuore aperto (OHS) rimane ancora un evento frequente; le cause sono multifattoriali: alterazioni emostatiche coinvolgenti i sistemi delle piastrine, della coagulazione, della fibrinolisi ed altro. Sebbene diminuite negli anni, le richieste di trasfusioni costituiscono, tuttavia, ancora un problema rimarchevole in termini economici e di rischi medici (e.g reazioni avverse, infezioni virali). La politica trasfusionale è altamente variabile nei diversi centri e non esistono linee guida mediche comuni. L’obiettivo principale del nostro studio è stato: identificare eventuali fattori demografici e peri-operatori predittivi di sanguinamento dopo OHS in bambini affetti da difetti settali (ASD,VSD) e Tetralogia di Fallot (TOF) al fine di caratterizzare i gruppi di pazienti a maggior rischio di trasfusione. Obiettivi secondari sono stati: analizzare l’incidenza di sanguinamento e di trasfusione nelle prime ore post-operatorie in coorti di pazienti omogenee per tipo cardiopatia, categoria di rischio RACHS-1, intervento chirurgico e protocollo di gestione peri-operatoria. METODI Lo studio si è svolto da febbraio ad agosto 2012 presso la Terapia Intensiva Cardiotoracica del Great Ormond Street Hospital, University College London, UK. Sono stati inclusi pazienti in età pediatrica sottoposti ad intervento chirurgico correttivo radicale di ASD, VSD e TOF. Sono stati raccolti i seguenti dati dei pazienti: - Pre-operatori: età, peso, comorbidità, diagnosi, eventuale terapia assunta, emocromo pre-operatorio. - Intra-operatori: tipo di correzione chirurgica, categoria di rischio RACHS-1, team medico-perfusionista, durata di circolazione extracorporea (CPB) e di clampaggio aortico (CC), grado di ipotermia, soluzioni prime e dosi infuse di eparina e di emocomponenti. - Post-operatori: emocromo post-operatorio, perdita di sangue misurata da drenaggio toracico, tipo e quantità di emocomponenti trasfusi. E’ stato utilizzato il medesimo protocollo anestesiologico e perfusionale in sede intra-operatoria e il medesimo protocollo trasfusionale per l’assistenza post-operatoria. I dati sono stati analizzati con il programma SPSS 20. Si è utilizzato un livello di significatività di p<0,05. RISULTATI E CONCLUSIONI Abbiamo raccolto i dati di 73 pazienti (15% ASD, 23% VSD, 29% ASD+VSD, 33% TOF). Il 55% della nostra coorte di pazienti ha ricevuto nel post-operatorio almeno una trasfusione e di questi il 48% ha necessitato di emazie. I nostri dati mostrano che esistono associazioni significative tra sanguinamento postoperatorio ed età, peso, ipotermia, valori pre-operatori di Hb, durata di CPB, categoria di rischio RACHS-1. L’analisi di regressione multivariata dei nostri dati mostra che il sanguinamento postoperatorio ha due fattori causali: il tempo di CC e il valore di conta piastrinica post-operatoria, che insieme spiegano il 30% circa del sanguinamento. I risultati del nostro studio confermano un’ipotesi avanzata da recenti lavori in letteratura di una ridotta funzionalità delle piastrine dopo CPB. La stima del rischio determinato dal CC comporta potenziali implicazioni cliniche: da un lato, la necessità di ridurre al minimo i tempi di CC; dall’altro, la possibilità di prevedere i pazienti a maggior rischio di instabilità emodinamica, al fine di individualizzare l’approccio terapeutico in termini di strategie emostatiche e trasfusionali. Altro risultato interessante fornito dall’analisi di regressione multivariata dei nostri dati è che la durata di CC sembra essere anche il maggiore fattore predittivo di trasfusione di emazie. Al momento il nostro è l’unico studio in letteratura che considera coorti di pazienti omogenee per tipo di cardiopatia, categoria di rischio RACHS-1, intervento chirurgico e protocollo di gestione peri-operatoria. Il nostro studio offre una prima evidenza di un ruolo causale del tempo di CC e dei valori di conta piastrinica post-operatoria nel determinare il sanguinamento in popolazioni di pazienti sottoposti a OHS. P48 “LOW COST” CARDIAC ECMO SUPPORT IN CHILDREN: ANALYSIS OF EFFECTIVENESS, COSTS AND OUTCOMES C. Tessari 1, M. Padalino 1, V. Vida 1, A. Guariento 1, P. Cogo 2, M. De Frnaceschi 1, F. Zanella 1, G. Stellin 1 1 Paediatric and Congenital Cardiac Surgery Unit, University of Padova, Medical School, Padua, 2 Paediatric Intensive Care Unit, Bambino Gesù Hospital, Rome, ITALY Background: extracorporeal membrane oxygenation (ECMO) support is recognized as a valid resuscitation therapy for children with congenital heart disease. However, concerns have been raised about the appropriateness of such an aggressive therapy, especially in light of the high costs and potential for long term neurologic disability. Aim: to evaluate effectiveness and clinical outcomes of extracorporeal membrane oxygenation (ECMO) support for care of critically ill children by means of an organization without a dedicated ECMO team, in a medium volume centre. Materials and methods: “Low cost” ECMO is meant as ECMO initiated without additional costs related to the organization of a specific dedicated ECMO team. A retrospective single-centre study of all ECMO runs from January 2001 to July 2012 was performed. ECMO supports were subdivided in 3 groups:1.Emergent (ECPR) when implanted after cardiac arrest; 2. Postcardiotomy (PC-E), when implanted in OR for unsuccessful weaning off CPBP; elective (E-E), when implanted in patients with low cardiac output syndrome with no cardiac arrest occured. Statystical analysis was oriented about evaluation of characteristics of patients, location of implantation of ECMO looking for complications, discharge and follow-up conditions. Calculation of financial saving was done according to our institutional costs for perfusionist and medical personnel, if dedicated 24 hours a day for the mean ECMO run duration. Results: a total of 128 ECMO were implanted in 121 patients with a median age of 104 days (range 1 day- 18 years) and a median weight of 4.7 kg (range 2.4-8.9). The majority (115/128) were implanted for cardiac reasons: E-E in 47, PC-E in 45, and ECPR in 36. Median duration of ECMO run was 6 days (min 0- max 52 days). Weaning off ECMO was successful in 52%, while hospital discharge was 30,5%. Twelve patients were converted to ventricular assisted device or cardiac transplant (successful outcome in 73 % ). Financial gross evaluation demonstrated that “low cost “ ECMO allowed our institution to save up to 1.276.969 euros, in 10 years. At statistical analysis, patients <30 days of age and <3 kg have a worse prognosis (p <0.03) because of higher risks of complications; ECMO run duration >7 days increases risk of infection (p < 0.005) and decrease the possibility to wean off ECMO (p = 0.002); when implanted in a cardiac surgery unit, ECMO is characterized by a statistically significant better outcome (p =0.05). Neurological complications are associated to neurological causes of death but not to neurological problems into the follow-up period. Conclusions: despite absence of an ECMO team, clinical results of “low cost “ ECMO are comparable to European centres with ECMO team, with no additional costs related to personnel dedicated to ECMO. The “ low cost” ECMO assistance can rescue up to a third of patients in whom death is otherwise certain. This experience is valuable in light of increasing cuts of national health institutions, but further improvement can be expected with better patient selection and appropriate timing and location for ECMO initiation. P49 OUTCAMES AND RISKS FACTORS FOR MORBILITY AND MORTALITY OF EXTREMELY PREMATURE NEONATES WITH CRITICAL CONGENITAL HEART DISEASE V. Vangi 1.2, Y. Corsini 1, E. Berti 1, R. Moschetti 2, U. Bottone 2, L. AitAli 2, G. Festa 2, I. Spadoni 2, G. Rossi 3, B. Murzi 2 1 AOU Careggi, Firenze,2 Ospedale Fondazione Monasterio, Massa, 3 CNR, Pisa, ITALY Although the outcome of neonatal cardiac surgery has dramatically improved in low body weigth neonates (LBW) less tha 2,5 Kg, still data relative to very low body weigth (VLBW), less than 1,5 Kg, are unavailable. VLBW is a population of prematures who is now growing due to improved perinatal skill strategies. Aim of this research was to describe the outcomes and identify risk factors for morbility and mortality in VLBW prematures with critical congenital heart disease (CCHD) defined as a defect requiring early surgical or transcatheter intervention admitted to our hospital . Prematures who met these two criteria, were included in this retrospective cohort study , period 2009-2012.Data were analyzed with Chi sq analysis. The study included a total of 31 prematures , 22 LBW and 9 VLBW.The differences, between the two groups and versus a group of 35 neonates with body weigth more than 2,5 Kg (NBW,)were analyzed. The diagnosis of VLBW included : 1 T.Atresia;1 TGA; 2 PA/VSD; 1 TOF; 1 CoA; 2 congenital complete heart block (CCHB); 1 VSD. Median gestational age in VLBW was 30 wks, 36 in LBW; 38 in NBW. Gestational age (GA )below 32 wks was significantly high in VLBW ((87%) in comparison to LBW (10%) and NBW (0%). The incidence of small weigth for gestational age (SGA) was significant in premature(33% in VLBW ; 52% in LBW) compared to NBW ( 3%). Prenatal diagnosis, presence of a duct dependent lesion, PGE infusion and time in ICU showed not significant differency between the groups. Variables which resulted significantly different were( 1) inotropic support : 89% VLBW ; 50% LBW; 80% NBW (2) surfactant therapy : 100% VLBW ; 9% LBW (3)duration ( range in days) of ventilatory support : 5-54 VLBW ;0-71 LBW; 0-27 NBW (4)mean age (months) at intervention : 2 VLBW; 0,3 LBW; 22 NBW (5)mean weigt( Kg) at surgery : 1,8 VLBW, 2,2 LBW; 3,1 NBW (6)palliative cardiac surgery : 88,9% VLBW; 22,7% LBW ; 22,9% NBW. Total hospitalization, expressed in days, was very long in VLBW: median 94 (5-148) in comparison to LBW 15(5-78) and NBW 21 (1-58). 2/9 VLBW ( 1 T. Atresia,1 TOF) were supported with PGE prior to the palliative intervention for 55 and 85 days respectively. 1/9 with CCHB was supported with a temporary external pacemaker for 3,4 months prior definitive implantation. 1/9 VLBW with PA/VSD underwent multiple procedures including one hybrid procedure . As major complications we observed 1 IVH , pacemaker insertion for post- op development of complete A-V block. Early mortality in the VLBW was 1/9 with CCHB, not significantly different respect to LBW . 4/9 VLBW were transferred from the cardiac surgery center to the neonatology unit of another hospital due to problems concerning growth while waiting for other surgical procedures.They were then subsequently reoperated upon and discharged at home at 4 to 5 monts of age. There are not late death with a follow up 6 months to 4 years. Conclusions: VLBW prematures less than 1,5 Kg, although studied in a relatively small number , seem susceptible of good surgical results in term of morbility and mortality; nevertheless massive ICU support and prolonged hospitalization remain crucial in order to overcome the adjuntive problems related to extreme prematurity.The management of these patients need an enlarged team comprehensive of all the multidisciplinary expertises .Verification of this preliminary report in a larger group is warranted. P50 EARLY AND LATE SURGICAL OUTCOMES OF ADULT PATIENTS WITH CONGENITAL HEART DISEASE: A SINGLE-CENTER EXPERIENCE G. Perri, A. Polito, G. Brancaccio, E. Cetrano, S.B. Albanese, A. Carotti Dipartimento Medico-Chirurgico di Cardiologia Pediatrica, Ospedale Pediatrico Bambino Gesù, Roma, ITALY Objective: As the number of grown-up congenital heart disease (GUCH) patients is progressively increasing, a thorough knowledge of factors associated with worse outcomes in this population is mandatory. Our aim was to evaluate early and late outcomes of a population of GUCH patients who underwent surgical treatment at our Institution. Material and Methods: We retrospectively analyzed 199 GUCH patients who underwent surgery between January 1996 and December 2012. The follow-up was complete in 90.5% of patients. Median time of follow-up was 26.1 months (range 0 – 179.2). Mean age at surgery was 251.3 months (range 207 – 571.1). Results: Fifty-one patients (25.6%) underwent primary surgical correction while 148 (74.4%) underwent re-intervention. The most common procedures were and LVOTR (66 patients, 41,1%) and RVOTR (42 patients, 21.1%). The overall survival at 5 years was 98.5% (95% CI 90.0-99.8). Freedom from re-intervention was 93.8% (95% CI 88.1-96.8) and 64.9% (95% CI 46.9-78.1) at 1 and 5 years respectively. Longer CPB time was independently associated with increased hospital mortality (OR, 95% CI: 1.004, 1.001-1.006, p 0.01). Previous surgery was independently associated with increased hospital morbidity (OR, 95% CI: 2.86, 1.22-6.69, p 0.01). We could not find any risk factors associated long-term survival and re-operation. Conclusion: In our experience, surgery in GUCH patients is commonly aimed at ventricular outflow tract reconstruction. Adequate peri-operative management is required to reduce post-operative morbidity and mortality in this population of patients. P51 REPAIR OF CONGENITAL AORTIC VALVE DISEASE BY BICUSPIDIZATION RESTORES PHYSIOLOGICAL PROPERTIES OF THE NATIVE AORTIC ROOT F. De Rita 1, G. Lucchese 1, G. Puppini 2, S. Hoxha 1, L. Rossetti 3, C. Sandrini 3, G. Faggian 1, A. Mazzucco 1, G.B. Luciani 1 1 Division of Cardiac Surgery, University of Verona, Verona, 2 Division of Radiology, University of Verona, Verona, 3 Division of Cardiology, University of Verona, Verona, ITALY Objective. Repair of congenital aortic valve (CAoV) lesions has gained widespread acceptance as alternative to valve replacement in the young. Two strategies exist to repair CAoV: creation of a three-leaflet anatomy (tricuspidization) or maintenance/creation of a two-leaflet anatomy (bicuspidization). To determine whether bicuspidization of CAoV may restore physiological properties of native aortic root, a prospective MRI study on patients undergoing repair was undertaken. Methods. Between 10/2010 and 10/2012, 9 consecutive patients had CAoV repair. Seven healthy, gender- and size-matched volunteers served as control. Patients underwent clinical, echcocardiographic, pre-operative and pre-discharge MRI assessment. Mean patient age was older than control (50±19 vs. 30±2, p=0.01), however gender (8/1 vs. 6/1, M/F) and BSA (1.8 ± 0.1 vs. 1.9 ± 0.2) were comparable. Diagnosis was aortic insufficiency due to bicuspid aortic valve (BAV) in 8 (4 antero-posterior, 4 latero-lateral) and to quadricuspid valve in 1. Repair consisted in valve bicuspidization in all, associated with supra-coronary ascending aortic graft replacement for aortic aneurysm in 4 (44%) Additional procedures were atrial septal defect, mitral valve repair, myocardial revascularization, each in 1 patient. The sinus of Valsalva segment was preserved in all. There was no mortality nor morbidity. No patient had more than mild residual insufficiency or stenosis at post-repair echocardiogram, while MRI to define morphology and physiology of the aortic valve and root. End-points for the study were: systolic and diastolic dimensions of the annulus, sinus, sino-tubular junction and ascending aorta; wall shear stress at the same 4 levels, measured by pressure strain elastic modulus (PSEM: [(Ps-Pd)/(Ds-Dd)]*Dm); opening angle of cojont cusp (CCOA). The latter 2 end-points were further assessed by univariate analysis based on geometry of BAV (antero-posterior vs. latero-lateral) and on presence of an aortic vascular graft. Results. Post-repair systo-diastolic diameters were significantly reduced compared with preoperative, at all 4 LVOT levels, but remained greater than control. Post-repair PSEM were significantly reduced at the sino-tubular junction and aortic levels (2515 ± 1476 vs. 1062 ± 405 vs. 887 ± 141 g/cm2, pre vs. post-repair vs. control, p=0.01, p=0.03), but remained greater than control. In patients having associated ascending aortic replacement, however, PSEM returned identical to control values (2478 ± 651 vs. 829 ± 281 vs. 907 ± 147 g/cm2, pre vs. post-repair vs. control, p=0.007, p=ns). Furthermore, PSEM at aortic level was surprisingly lower in repaired patients carrying aortic grafts compared to those retaining native aorta (829 ± 281 vs. 1350 ± 174, p=0.02). CCOA was smaller than control tricuspid valves, as expected, but was significantly smaller in latero-lateral BAV compared with antero-posterior (68.6 ± 2.3° vs. 63.5 ± 2.5°, p=0.03). This resulted in greater asymmetry of coaptation angle (<160°)(1/5 vs. 4/4, AP vs. LL, p=0.02) and ascending aortic flow profile (2/5 vs. 4/4, AP vs. LL, p=0.05). Conclusions. CoAV repair by bicuspidization allows to reduce LVOT dimensions and to restore elasticity of the native aortic root, when the ascending aorta is replaced by vascular graft. The ability to restore a valve opening angle and coaptation symmetry, which affect symmetry of aortic flow, is influenced by BAV geometry. P52 SURGERY FOR TOTAL ANOMALOUS PULMONARY VENOUS CONNECTION: A 22-YEAR EXPERIENCE IN A SINGLE INSTITUTION M. Padalino 1, G. Cavalli 1, M. De Franceschi 1, D. Mancuso 2, N. Maschietto 3, V. Vida 1, O. Milanesi 3, G. Stellin 1 Pediatric and Congenital Cardiac Surgery, Department of Cardiac Thoracic and Vascular Sciences, Padua, 2 Division of Cardiology, Public Hospital, Cittadella (PD), 3 Pediatric Cardiology, Department of Women and Children's Health, Padua, ITALY Background: Total Anomalous Pulmonary Venous Connection (TAPVC) is a rare congenital heart disease, whose surgical repair is reported to be associated with high mortality and reoperation rates. We aim to identify predictors of operative and late mortality, and impact of associated cardiac anomalies on early and late outcomes. Methods: all patients who underwent surgical repair for TAPVC from 1989 to 2012 were included. We considered as isolated TAPVC those patients (Group 1) with no Congenital Heart Defects (CHD) other than simple ones (i.e. PDA, PFO and ASD). All other associated CHD, such as AVSD, DORV, HLHS, functionally single ventricle(SV) physiology, or Scimitar Syndrome associated with TAPVC entered the complex group of patients (Group 2).We reviewed medical records and telephone interviews were performed to assess clinical condition in the follow-up. Results: 46 patients were included in the study (M/F: 26/20, median age 26 days, range 15-59, median weight 3,350 kg, range 2,980-4,470). Group 1 (isolated) included 30 patients (65%), while group 2 (with associated CHD) included the remaining 16 pts (35%). TAPVC was found to be obstructive in 33%; single ventricle physiology was associated in 11 patients, heterotaxy syndrome in 8. Anatomical types of TAPVC were as follows: supracardiac in 48%, intracardiac in 20%, infracardiac in 20% and mixed in 12%. Overall operative mortality was 17% (8/46); however, it was significantly higher in Group 2 vs Group 1 (75% vs 17.2%, p value < 0.01), as was higher incidence of postoperative complications (87% vs 31 %, p value 0.001). In addition, operative death was significantly related to low weight at surgery (lower than 3kg, p=0,02), single ventricle physiology (p=0,013) and association with other CHDs (p=0,002). At a median follow up of 3 years (0.01-21.7 yrs, 91% complete), there were 8 late deaths (21%) and 15 patients (40%) had major adverse event during follow up. Multivariate analysis of event free survival showed worse outcome in patients with associated CHD (Group 2, p value 0.0001), with mixed type TAPVC (p=0,005), obstructive TAPVC (p=0,087) and history of postoperative complications (p=0,03) Conclusion: early and long term outcomes of isolated TAPVC are excellent . However, surgical mortality and morbidity are still consistent in patients with TAPVC and associated cardiac anomalies. <FILE IMAGE='131_20130626124508.jpg'> P53 SINGLE CENTER EXPERIENCE WITH LEVOSIMENDAN ADMINISTRATION AFTER PEDIATRIC CARDIAC SURGERY R. Giordano, G. Palma, S. Palumbo, S. Cioffi, V. Russolillo, M. Mucerino, V. Poli, C. Vosa Dept. of Advanced Biomedical Sciences, Division of Adult and Pediatric Cardiac Surgery, University of Naples Federico II, Naples, ITALY Background: Low cardiac output after cardiopulmonary bypass is a well known problem in the early postoperative course after complex congenital heart surgery that affects the postoperative recovery of about 25% of patients. It may cause prolonged mechanical ventilation, increased risk of infection and sepsis, longer stay in the intensive care unit, and increased mortality. We conducted a single center case-control retrospective study of patients undergoing cardiopulmonary bypass to determine the effect of levosimendan in the management after pediatric cardiac surgery. Methods: From January 2008 to December 2012, during two different periods, a total of 92 pediatric patients undergoing elective cardiac surgery with cardiopulmonary were included in this study. The control group included 67 patients who underwent surgery between January 2008 and December 2010 and arrived in the intensive care unit with high inotropic score (IS> 30). During this period no levosimendan was used. The levosimendan group was comprised of children operated between January 2011 and December 2012. From then onwards, a dose of 0.1 µg/kg/min of levosimendan was given for 72 hours by infusion to 25 patients arrived in the intensive care unit with high inotropic score (IS> 30). All other parameters that may influence the perioperative management, in particular anesthesia and CPB course, were not modified during the two periods under review. Results: Four patients (5.9 %) died in the control group (2 postsurgical severe left ventricular dysfunction, 2 multiple organ dysfunction syndrome) and one (4 %) in the levosimendan group (postsurgical severe left ventricular dysfunction) (p = 0.59). Among the hemodynamic outcome only postoperative heart rate tended to be lower in levosimendan patients. As metabolic outcome, mixed venous oxygen saturation was lower in control group at 12, 24 and 48 h (respectively, p = 0.0034, p = 0.001 and p = 0.03) and lactate levels tended to be lower in the levosimendan group with difference at 6, 12,18, 24 and 48h (respectively, p = 0.004, p = 0.0001, p = 0.0001, p = 0.0002, p = 0.001 ). Inotropic score was lower in the levosimendan group in each detection up to 72 hours (40±8 vs. 45±10, p = 0.027 at 6h, 20±4 vs. 30±6, p = 0.0001 at 72h). Finally, we found lower intubation time (p = 0.006), intensive care unit and total hospital stay (p = 0.002 and p = 0.004) in levosimendan group. With regard to the pharmacodynamic properties, particularly of the metabolite of levosimendan with a persistence of approximately one week, no early or late adverse effects were reported. Conclusion: Our initial experience in this retrospective study provide further evidence that levosimendan may be used as inotropic substance in the field of congenital cardiac surgery with a positive effect in the postoperative management, but further studies, larger and randomized, are necessary to determine the efficacy, safety, and optimal dosing in children following cardiac surgery in comparison with placebo or other inotropic drugs. P54 NECROTIZING ENTOROCOLYTIS IN PATIENTS UNDERGOING EARLY HYBRID PROCEDURE FOR COMPLEX CONGENITAL HEART DISEASE S. Morelli, L. Manuri, S. Agati, M.B. Saitta, D. Poli, G. Pongiglione, E. Iannace, P. Guccione, F.S. Iorio Centro Cardiologico Pediatrico del Mediterraneo, Taormina, ITALY Objective. Necrotizing enterocolitis (NEC) is primarily a disease of the premature infants with widespread implications for neonates. Among children at term, however, congenital heart disease may be an important predisposing factor for this condition, particulary those with ductus dependent systemic circulation. Despite hybrid procedure became a promising option for palliative treatment of HLHS patients, NEC is still diffusely reported. We report our experience on neonates undergoing “early” single stage hybrid procedure focusing on incidence of NEC or major gastrointestinal complications. Materials and Methods. From October 2011 to February 2013, 20 consecutive patients underwent “early” single stage hybrid procedure for palliation of HLHS and variants at our Institution. At the time of procedure median age was 1 day (range 1 to 5), median weight 3 Kg (range 2,2 to 4,2 Kg). All patients underwent procedure while on Prostaglandines (PGE1?) continuous infusion at a range dose from 0,001 to 0,02 mcg/kg/min. According to our protocol, patients that performed fast-track extubation received enteral feeding after 6 hours, while intermittent enteral feeding (2 to 15 ml/h during 20 hours per day) was established in the case of prolonged mechanical ventilation. Results. All patients survived to the procedure and were successfully discharged from Hospital. Median ICU length of stay was 7 days (1 - 70 days) and median in-hospital length of stay was 16 days (6 - 70 days). All of them received perioperative vasodilators infusion with fenoldopam, milrinone, while in three cases short term epinephrine infusion was used and one of them added levosimendan. Two patients required tracheostomy and one postperative temporary peritoneal dialysis was used. No patients showed signs or symptoms of NEC or major gastrointestinal complications. Conclusions. “Early” single stage hybrid approach outcome for HLHS patients was relevant in terms of mortality and morbidity. It allows us to operate on neonates before establishment of enteral feeding and as a part of the approach it translate in a NEC free experience. P55 ATRIAL MYXOMA IN WILLIAM SYNDROME AFTER CARDIAC SURGERY: A NEW ASSOCIATION F. Fratta 1, C. Iacono 1, A. Rea 1, G. Capozzi 1, M. Palladino 1, G. Di Salvo 1, G. Caianiello 2, M. Russo 1 1 Cardiologia Pediatrica, SUN, AO Monaldi, Napoli, 2 Cardiochirurgia Pediatrica, SUN, AO Monaldi, Napoli, ITALY Background: Williams-Beuren Syndrome (WBS) arises when there is a genomic microdeletion at human chromosome 7q11.23 (Mouse 5G2), resulting in various cardiovascular, developmental, metabolic, and mental disorders. WBS individuals have a combined prevalence of cardiovascular disease of 84% that includes supra- and sub-aortic stenosis (SVAS); aortic, pulmonary, and m itral valvular disease; aortic coarctation; hypertension; and, less commonly, myocardial infarction. To date, cardiac masses (tumors) have not been reported in patients with WBS. Case report: We report the case of a 15 years old girl who had a fetal diagnosis of mitral dysplasia. At birth a mitral dysplasia with aortic coarctation was detected by ultrasonography and she underwent surgical correction (decoarctation with patch). At 2 yo, for facial dysmorphysms , failure to thrive, and cognitive development, a clinical diagnosis of WBS was suspected, and then confirmed by FISH analysis. At 7 years a balloon angioplasty was performed for aortic re-coarctation. At 10 years following the evidence of severe mitral regurgitation, she underwent mitral surgical valvuloplasty with residual moderate regurgitation. At the age of 13 yrs, a posterior mitral leaflet prolapse with severe regurgitation was detected by echocardiography, requiring a new annuloplasty with rigid prosthetic rings. After the last operation she was followed up by semestral clinical and echo evaluations, showing trivial-moderate mitral regurgitation, dilated left atrium, normal isthmus flow. At last follow-up , a 3x2 cm mass was identified on the right atrium , attached to the edge of tricuspid valve. The mass was prolapsing through the tricuspid valve into the right ventricle without obstructing the inflow. The mass was excised, and histological evaluation revealed an atrial myxoma. DISCUSSION: To the best of our knowledge, this is the first report of an atrial myxoma in patients with WBS. Cardiac abnormalities in WBS include supra- and sub-aortic stenosis (SVAS); aortic, pulmonary, and m itral valvular disease; aortic coarctation; hypertension; and, less commonly, myocardial infarction. Cardiac tumors are rare CV abnormalities with an incidence of less than 0.1 percent, and they have previously not benn reported associated to WBS. On the other hand, patients with other syndromes associated to cardiac involvement (such as RAS-MAPK syndromes, including Costello and CFC) are at increased risk of CT It is important to early recognize CT since they are associated with significant complication It is not known whether atrial mixoma, and CT in general, are bystanders in WBS, or may be part of the clinical spectrum of the disease. Williams syndrome results from mutations involving the elastin gene on chromosome 7q11.23. This gene's protein product gives blood vessels the stretchiness and strength required to withstand a lifetime of use. The elastin protein is made only during embryonic development and childhood, when blood vessels are formed. Because they lack the elastin protein, people with Williams Syndrome have disorders of the circulatory system and heart defects. We wonder whether and how this gene could be involved in cell proliferation and susceptibility to cardiac tumors in WBS. P56 EXTRACELLULAR MATRIX GRAFT FOR CARDIAC AND VASCULAR RECONSTRUCTIVE SURGERY, PRELIMINARY CLINICAL RESULTS O. Milanesi, G. Torin, M. Padalino, V. Vida, N. Maschietto, R. Biffanti, A. Cerutti, B. Castaldi, G. Stellin A.O. Università di Padova, Cardiologia e Cardiochirurgia Pediatrica, Padova, ITALY Background: Porcine extracellular matrix graft (Cormatrix®ECM) has been widely used in clinical setting to repair pericardium, but no reports exist to date showing its use and efficacy in vascular and cardiac repair. Aim: To evaluate Cormatrix®ECM material as a possible patch for clinical use in reconstructive cardiac surgery. Methods: We reviewed the report of the last clinical and echocardiographic evaluation of 23 patients affected by: Tof, PV stenosis isolated or in association with other CHD, AS, PAPVD, other CHD, operated on at our Institution between December 2009 and December 2012, in whom Cormatrix® ECM patch was used during reconstructive surgery. We included in our evaluation only patient in whom Cormatrix® ECM patch was employed for RVOT or PV/PAs reconstruction, with at least 1 echo examination after discharge home Results: 14 patients met the enrolment criteria, affected by Tof 10 cases, DORV sub pulmonary VSD + sub AoS + AoCo 1 case, complete A-V septal defect, PS and RV hyoplasia 1, asplenia syndrome+ single RV + PS 1. Median age at operation was 4.8 months (1-66). Cormatrix® ECM patch was used for RVOT reconstruction in ToF patients, PV reconstruction in 2 cases, PAs patch augmentation in 2. At a mean follow-up of 15,3 months (2-24) severe RVOT stenosis requiring treatment was present in 2 ToF patients, one in association with signs of persistent inflammation and pulmonary haemorrhage requiring pneumonectomy. Absent or trivial pulmonary regurgitation was recorded in 2 ToF, mild in 2, moderate in 4, in one associated with moderate stenosis, the last 4 with RV dilatation. One patient each in the group of PV reconstruction and PAs augmentation presented severe recurrent stenosis, requiring hemodynamic manoeuvres. We conclude that at a short term follow-up the performance of Cormatrix® ECM patch for RVOT or PV/PAs reconstruction seems suboptimal. Further clinical experience and longer follow-up are needed to judge the adequacy of this material. P57 ANTITHROMBIN III IS PROGNOSTIC OF CLINICAL OUTCOME IN PEDIATRIC EXTRACORPOREAL MEMBRANE OXYGENATION G. Lucchese 1, S. Hoxha 2, A. Prioli 1, G. Faggian 1, A. Mazzucco 1, G.B. Luciani 1 1 Division of Pediatric Cardiac Surgery, University of Verona., Verona, 2 Division of Pediatric Cardiology, University of Verona, Verona, ITALY Objective. Heparin remains the predominant anticoagulant during extracorporeal membrane oxygenation (ECMO). Heparin binds to antithrombin III (AT) causing inactivation of thrombin and other proteases involved in blood clotting. AT is consumed during ECMO and low levels could be observed early at admission to the intensive care unit (ICU). This study investigates the association between AT activity at admission to the ICU and outcome in the pediatric cardiac ECMO population. Methods. Between 2002-2013, records of 25 consecutive infants and children undergoing V-A ECMO were retrospectively assessed. All patients were anticoagulated with continuous heparin infusion and AT was maintained >70%. Results. Twenty-five patients underwent 28 ECMO (3 second run) and 80% were post-cardiotomy. Median age was 31d (4d-17y), with a median weight of 3.4 kg. Seventeen (61%) patients were successfully weaned and hospital survival rate was 32%. As seen with univariate analysis, initial AT<70% was significantly associated with higher blood loss, prolonged mechanical ventilation time and ICU stay, higher incidence of surgical reexploration, post-weaning low cardiac output syndrome (LCOS) and hospital mortality. When corrected for the other explanatory variables, low levels of AT remained independently associated with prolonged ICU stay, higher incidence bleeding and LCOS (p<0.05). Conclusions. Low levels of AT during ECMO are associated with poor outcome. AT is predictive of prolonged ICU stay, higher mortality, bleeding and cardiac dysfunction. A direct biochemical effect of AT activity at myocardial level may be hypothesized, but the exact mechanism is still unclear. P58 AORTO-AORTIC FISTULA ASSOCIATED TO AORTIC INCOMPETENCE: CASE REPORT F. Gandolfo 1, A.D.M. Secinaro 2, E. Cetrano 1, A. Carotti 1 1 Ospedale Pediatrico Bambino Gesù, IRCCS – DMCCP, Cardiochirurgia, Roma, 2 Ospedale Pediatrico Bambino Gesù, IRCCS, Dipartimento di Imaging, Roma, ITALY Aims of the study To describe the case of isolated severe aortic incompetence in a 4-year old child with occasional finding of ascending aorto-aortic fistula. Methods A 18 kg body weight and 0.66 m² BSA female presented to our observation for severe insufficiency of tricuspid aortic valve (vena contracta 6 mm, holosystolic reverse flow in the abdominal aorta) and dilation of the left ventricle (LVIDd 4.6 cm, Z-score 5.2) with good systolic function (FE 64%). At CMR and CT scan an unexpected eversion of the aortic wall was evident in correspondence of the antero-lateral left wall of the ascending aorta and in contiguity with the sino-tubular junction near the intercoronary commissure (fig 1). Asymmetric dilatation of the ascending aorta at the level of the lesion coexisted with loss of the sino-tubular junction. Coronary arteries were normal. Results Surgical treatment consisted of an autograft aortic root replacement with complete resection of the diseased segment of the ascending aorta. Postoperative course was uneventful and 2D-ECHO after 2 months showed good biventricular function with trivial aortic incompetence. Histological examination of the aortic specimen documented a 0.7 cm polypoid formation with rearrangement of the wall, disappearance of elastic fibers, and fibroelastic proliferation with vorticoid pattern. There was no evidence of any active inflammatory process. Conclusions Diagnostic hypotheses of the fistula included infectious pseudoaneurysm, primitive aortopaty, aortic trauma. According to the finding of thickening of the aortic cusps in correspondence of the fistula, aortic insufficiency may have been caused by the turbulence produced by the bloodstream across the fistula directed from the distal to the proximal port respect to the valve. The lesion described can be taken into consideration in the differential diagnosis of non-rheumatic isolated aortic incompetence in childhood. <FILE IMAGE='664_20130626124832.jpg'> P59 THE BLALOCK-TAUSSIG MODIFIED SHUNT VIA MEDIAN STERNOTOMY: THE COSTS TO PAY FOR A BALANCED PULMONARY BLOOD FLOW D. Troise, V. Cassano, G. Epicoco, C. Lasaracina, C. Mancini, F.P. Annecchino Pediatric Cardiac Surgery Department, Bari, ITALY Objective: Even though the indication for shunt operation has decreased with a growing number of intracardiac repairs performed in infancy, surgical approaches to the patients affected with congenital heart disease with obstructed pulmonary outflow still include Blalock-Taussig modified shunt (BTMS). Nowadays an increasing number of surgical Institutes prefers to perform the shunt via a median sternotomy instead of the “traditional” lateral thoracotomy, in order to: 1) avoid pulmonary arteries distortion and unbalanced pulmonary blood flow 2) avoid the developing of aortopulmonary collateral circulation 3) manage the ductal patency 4) reduce the surgical scars with its cosmetic and functional consequences The aim of this study is to evaluate the preoperative, perioperative and postoperative risk factors that may interfere with the outcome of BTMS via median sternotomy. Methods: From January 2009 to April 2012 21 patients received a BTMS via median sternotomy The patients scheduled to repair were affected with Tetralogy of Fallot (8 cases), pulmonary atresia and intact septum (7 cases), tricuspid atresia (3 cases), heterotaxy syndrome (1 case), Tetralogy of Fallot and pulmonary atresia (2 cases). Mean age was 39 days (range 3 to 124 -median 8 days), mean weight was 3,6 Kgs (range 2,5 to 5,3- median 3,35 Kgs). All procedures were performed without the need of a cardiopulmonary by-pass (CPBP); except 1 case. Periprocedeural factors with potential inference on early outcome were idientified and correlated with the early outcome Results: The early mortality rate was of 4,7% (1 case) not related to the shunt disfunction, the major adverse cardiovascular events (MACE) were severe hemodynamic instability in 3 cases, and sternal dehiscence in 1 case. Acute shunt thrombosis was observed in 4 of 20 (20%), none leading to death. In cases of prosthetic failure a 2nd MBTS was performed: in 3 cases via median sternotomy and at the same site (1 case with the aid of CPBP for systemic hypotension) and in the last case via lateral approach. At a follow-up of 23 months the late mortality rate was of 5% (1 case) and it was not related to the shunt thrombosis. Acute shunt thrombosis was not significantly correlated with the size of the prosthesis, the surgeon, the cardiac lesion, the size of the pulmonary arteries, the surgical approaches and an “atypical” vascular pattern Conclusion: In the Aristotle basic score the level of difficulty of the BTMS is marked as 2.3 (that is to say simple), but the shunt thrombosis, in our experience, is not an unfrequent complication and when it happens it may lead to stormy The closure of the patent arteriale duct, at the time of the implantation of the prosthesis, has an intriguing role in the appropriateness of the correction