Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Azienda
Sanitaria
Firenze
Quali indicazioni all’impiego della doxorubicina liposomiale Colori compositi
Catia Angiolini
SC Oncologia Medica
Dipartimento Oncologico
(Direttore, Luisa Fioretto)
Background ¤ Conven'onal anthracyclines are the most widely used agents to treat breast cancer in the adjuvant se8ng, as well as in metasta'c disease. ¤ Doxorubicin-‐ based regimens have demonstrated benefits in terms of ORR, TTP, and OS. ¤ Despite its excellent an'tumor ac'vity, however, conven'onal doxorubicin has a rela'vely low therapeu'c index, and its use is limited by acute side effects, as myelosuppression, alopecia, acute nausea and vomi'ng, stoma''s, cardiac events (LVD, myocardi's, arrhythmia) ¤ Cumula:ve cardiotoxicity is a major concern, leading to poten'ally fatal conges've heart failure. Azienda Sanitaria Firenze
2
Anthracycline-‐induced cardiotoxicity ¤ Cardiotoxicity occurs when metabolic free radicals cause lipid peroxida:on. ¤ Ini'ally, damage to the heart is subclinical; however, con'nued treatment will lead to progressive myocyte damage. The resul'ng cumula've cardiac dysfunc'on may become evident during therapy or subsequently in months or years aMer the final doxorubicin dose. ¤ Several factors may poten'ally increase the pa'ent’s risk of developing anthracycline-‐induced cardiotoxicity: higher cumula,ve anthracycline dose increased rate of drug administra,on advanced or very young age medias,nal radia,on female gender preexis,ng heart disease hypertension. Azienda Sanitaria Firenze
3
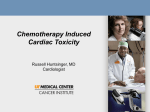
Women aged 66 to 70 years: freedom from congestive heart failure (CHF) by adjuvant
chemotherapy type.
Pinder M C et al. JCO 2007;25:3808-3815
Azienda Sanitaria Firenze
©2007 by American Society of Clinical Oncology
4
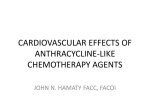
Risk of anthracycline-‐related CHF 1.0
0.9
Doxorubicin Epirubicin 0.8
0.7
Swain et al (2003) 0.6
Von Hoff et al (1979) 48% 0.5
Ryberg et al (1998) 0.4
0.3
26% Limat et al (2003) 0.2
0.1
5% 0.0
0
100
200
300
CHF: Conges've Heart Failure. Azienda Sanitaria Firenze
400
18% 7% 3% 500
600
700
800
900 1000 1100 1200 1300 1400
Cumula:ve dose mg/m2 5
2)-41+T+b121TR' Q)R' J3' 4301.34' )/O+' J)O34' +.'
TX3' ,.43-/R1.N' Q32X).1OQO' ).4' -3S3-O1J1/1TRI'
TX1O' 2X)-)2T3-1`)T1+.' X)S1.N' TX3' )J1/1TR' T+' V-3@
412T'1--3S3-O1J/3'UC').4'T+'Q+.1T+-'TX3'OV321012'
Q).)N3Q3.T';L)J/3'7<';76I7?<^''
QR+'2)-41,QI' /3)41.N' T+' TX3' 2)-41+T+b121TR'
;C1N,'-3'7<';:I57<^'"#$%&'()(*+#,-.')'\143/R',O34'
2X3'Q+'TX3-)V3,T12OI' 1.4,23' Q1T+2X+.4-1)/' 4)@
Q)N3I'2X).N3O'1.'"LZ'V-+4,2T1+.I').4'23//,/)-'
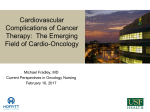
Defini:on of cardiotoxicity based on the mechanisms and reversibility G3HIE/*01%V:)%8$#)+5%)77)+5*%(4%5:)%;6(+"#8$,;%(7%5:)%+:);(5:)#"?),5$+"'%8#,=*%')"8$4=%5(%
+"#8$(5(S$+$56%TW-JBUG
*
+#2"*3*45678&59#9:;6"<:;=">
+#2"*33*47&5(7?@?A5B<:;=">
C"::?:5&*A"9856;(A
0)''*%8)"5:%
0)''*%86*7,4+5$(4%
D%("*&":57"'*
0,;,'"5$1)%
O(5H+,;,'"5$1)%
E"F"&(;B;:;7#
9)#;"4)45
F)1)#*$P')%
+,-./*01%.)7$4$5$(4%(7%+"#8$(5(S$+$56%P"*)8%(4%5:)%;)+:"4$*;*%"48%#)1)#*$P$'$56%TBK-BDUG
!&0#$%&
Azienda Sanitaria Firenze
11-123456&7138197$6$%&71!0#$%$60:1;374<01=1>3?@1AB@C
#%
Florescu, MAEDICA 2013 6
liposomal anthracyclines ¤ Liposome-‐based drug delivery systems are able to modify the pharmacokine'cs and pharmacodynamics of cytosta'c agents, enabling to increase the concentra'on of the drug released into the neoplas'c 'ssue and, at the same 'me, reducing the exposure of normal 'ssue to the drug. ¤ There are several liposome-‐encapsulated doxorubicin formula'ons available which show different pharmacological characteris'cs. The most commonly used are liposomal doxorubicin (Myocet®, LD) and pegylated liposomal doxorubicin (Caelyx®, PLD). Azienda Sanitaria Firenze
7
6
Journal of Drug Delivery
RCTs of liposomal anthracyclines vs. conven:onal anthracyclines Table 2: Trials that directly compared liposomal anthracyclines with conventional anthracyclines, either in monotherapy or combination.
Author
O’Brien et al.
[33]
Harris et al.
[34]
Batist et al.
[35]
Chan et al.
[36]
Sparano et al.
[37]
Trial phase
III
III
III
III
III
Treatment regimen
PLD (50 mg/m2 /4w)
versus
ADR (60 mg/m2 /3w)
LD (75 mg/m2 /3w)
versus
ADR (75 mg/m2 /3w)
LD (60 mg/m2 ) + CTX (600 mg/m2 )
versus
2
ADR (60 mg/m ) + CTX (600 mg/m2 )
LD (75 mg/m2 ) + CTX (600 mg/m2 )
versus
2
EPI (75 mg/m ) + CTX (600 mg/m2 )
Docetaxel (75 mg/m2 )
versus
Docetaxel (60 mg/m2 ) + PLD (30 mg/m2 )
Patients’
characteristics
Stage IV
PFS
OS
RR
6.9 m 21 m 33%
versus versus versus
7.8 m 22 m 38%
3.8 m 16 m
Stage IV
versus versus 26%
(17% ADR previous)
4.3 m 20 m
5.1 m 19 m
Stage IV
(10% ADR previous) versus versus
5.5 m 16 m
(30% CRF)
Toxicity
Cardiac:
4.7 versus 19.6%
CHF: 0% versus 4%
Cardiac: 13 versus 29%
CHF: 5.9 versus 15%
Billingham > 2.5:
26 versus 71%
Cardiac: 6 versus 21%
(𝑃 < 0.05)
CRF: 0 versus 3.2%
7.7 m 18.3 m 46 %
Cardiac: 11 versus 10%
Stage IV
versus versus versus
No CRF
(No ADR previous)
5.6 m 16 m 39 %
Stage IV
(100% ADR
previous)
7 m 20.6 m
versus versus
9.8 m 20.5 m
Cardiac: 4 versus 5%
PPS: 0 versus 24%
PLD: pegylated liposomal doxorubicin; LD: liposomal doxorubicin; ADR: adriamycin; EPI: epirubicin; CTX: cyclophosphamide; PFS: progression-free
survival; OS: overall survival; RR: response rate; PPS: plantar-palmar syndrome; CHF: clinical heart failure; and CRF: cardiac risk factor.
Azienda Sanitaria Firenze
Lao, J Drug Del, 2013 8
Liposome-Encapsulated Doxorubicin Compared
with Conventional Doxorubicin in a Randomized
Multicenter Trial as First-Line Therapy
of Metastatic Breast Carcinoma
Lyndsay Harris, M.D.1,2
Gerald Batist, M.D.3
Robert Belt, M.D.4
5
Douglas
2 Rovira, M.D. 6
Rudolph Navari, M.D.
Nozar Azarnia, Ph.D.7
Lauri Welles, M.D.8
Eric Winer, M.D.1,2
TLC D-99 Study Group
for the
Chemotherapy (dose mg/m ) N. RR (%) 108 26 Myocet® 75
Duke University Medical Center, Durham, North
vs Carolina.
Dana-Farber Cancer Institute, Boston, MassaDoxo 75 116 26 chusetts.
1
2
3
McGill University, Montreal, Quebec, Canada.
4
St. Luke’s Hospital, Kansas City, Missouri.
5
University of Colorado, Denver, Colorado.
6
Simon Williamson Clinic, Birmingham, Alabama.
7
Columbia Presbyterian Medical Center, New
York, New York.
8
Elan Pharmaceuticals, Princeton, New Jersey.
Presented in part at the 34th Annual Meeting of the
American Society of Clinical Oncology, Los Angeles, California, May 16 –19, 1998.
Supported by a grant from Elan Pharmaceuticals,
Princeton, New Jersey.
The following investigators and their institutions
BACKGROUND. The objective of this study was to compare the efficacy and toxicity
OS Cardiac CHF astatic breast carcinoma (MBC).
Toxicity (%) (months) METHODS.
Two hundred twenty-four patients with MBC and no prior therapy(N) for
of the liposome-encapsulated doxorubicin, TLC D-99 (Myocet, Elan Pharmaceuticals, Princeton, NJ), and conventional doxorubicin in first-line treatment of met-
metastatic disease were randomized to receive either TLC D-99 (75 mg/m2) or
doxorubicin (75 mg/m2) every 3 weeks, in the absence of disease progression or
unacceptable toxicity. The primary efficacy endpoint was response rate. Responses
were assessed using World Health Organization criteria and were required to be of
at least 6 weeks’ duration. The primary safety endpoint was cardiotoxicity. Cardiac
function was monitored by multiple-gated radionuclide cardioangiography scan,
and the left ventricular ejection fraction (LVEF) was scored at a central laboratory.
Patients were removed from study if LVEF declined 20 or more EF units from
baseline to a final value of greater than or equal to 50%, or by 10 or more units to
a final value of less than 50%, or onset of clinical congestive heart failure (CHF).
RESULTS. Median age was 54 years in both treatment groups. All relevant prog-
16 20 ns ard Love, University of Wisconsin Hospital, Madison, WI; Dustan Osborn, Western Washington Cancer Center, Olympia, WA; Joseph Aisner, University
of Maryland Cancer Center, Baltimore, MD; Tom
Anderson, Froedtert Memorial Lutheran Hosp, Milwaukee, WI; Dean Butler, Dial Research Associates, Nashville, TN; Paul Calabresi, Rhode Island
Hospital, Providence, RI; Lawrence Feldman,
Mount Sinai Hospital, Chicago, IL; Robert Kerr,
Southwest Regional Cancer Centers, Austin, TX;
Hans Nevinny, Memorial Medical Center, Tulsa,
OK; Craig Reynolds, Ocala Oncology Center, Ocala,
FL; Andrew Schneider, Hematology and Medical
Oncology, Lauderhill, FL; Charles Tweedy, Amos
13 29 p= 0,0001 2 9 p= 0,0001 Michael Garcia, Norwood Clinic Research Center,
Birmingham, AL; Joel Granick, Midwestern Regional Medical Center, Zion, IL; Jonathan Kloss,
Lourdes Hospital Cancer Center, Binghamton, NY;
Michael Roberts, Hematology and Oncology Associates, Phoenix, AZ; Federico Sanchez, Cancer Care
Center, Menomonee Falls, WI; Richard Silver, New
York Hospital–Cornell Medical Center, New York;
Harvey Taylor, Hodges Cancer Center, Lubbock, TX.
Address for reprints: Lyndsay Harris, M.D., DanaFarber Cancer Institute, Room D1210, 44 Binney
Street, Boston, MA 02115; Fax: (617) 632-3709;
Harris et al, Cancer 2002 R e d u c e d C a r d i o t o x i c i t y a n d P r e s e r v e d A n t i t u m o r E f fi c a c y
of Liposome-Encapsulated Doxorubicin and
Cyclophosphamide Compared With Conventional
Doxorubicin and Cyclophosphamide in a Randomized,
Multicenter Trial of Metastatic Breast Cancer
By Gerald Batist, Gopal Ramakrishnan, Chandra Sekhar Rao, Aruna Chandrasekharan, John Gutheil, Troy Guthrie,
Pankaj Shah, Ali Khojasteh, Madhavan Krishnan Nair, Karen Hoelzer, Katherine Tkaczuk, Youn Choi Park,
and Lily W. Lee for the Myocet Study Group
Purpose: To determine whether Myocet (liposomeencapsulated doxorubicin; The Liposome Company,
Elan Corporation, Princeton, NJ) in combination with
cyclophosphamide significantly reduces doxorubicin
2 cardiotoxicity while providing comparable antitumor
efficacy in first-line treatment of metastatic breast
cancer (MBC).
Patients and Methods: Two hundred ninety-seven
patients with MBC and no prior chemotherapy for metastatic disease were randomized to receive either 60
mg/m2 of Myocet (M) or conventional doxorubicin (A),
in combination with 600 mg/m2 of cyclophosphamide
(C), every 3 weeks until disease progression or unacceptable toxicity. Cardiotoxicity was defined by reductions in left-ventricular ejection fraction, assessed by
serial multigated radionuclide angiography scans, or congestive heart failure (CHF). Antitumor efficacy was assessed
by objective tumor response rates (World Health Organization criteria), time to progression, and survival.
Chemotherapy (dose mg/m ) N. RR (%) OS (months) Myocet® 60 + Cy 600 vs Doxo 60 + Cy 600 142 155 43 43 19 16 ns D
OXORUBICIN IS recognized as one of the most
active drugs for breast cancer, but its clinical utility is
limited because of a cumulative dose-dependent cardiac
myopathy that can lead to potentially fatal congestive heart
Results: Six percent of MC patients versus 21% (including five cases of CHF) of AC patients developed
cardiotoxicity (P ! .0002). Median cumulative doxorubicin dose at onset was more than 2,220 mg/m2 for MC
versus 480 mg/m2 for AC (P ! .0001, hazard ratio,
5.04). MC patients also experienced less grade 4 neutropenia. Antitumor efficacy of MC versus AC was comparable: objective response rates, 43% versus 43%;
median time to progression, 5.1% versus 5.5 months;
median time to treatment failure, 4.6 versus 4.4
months; and median survival, 19 versus 16 months.
Conclusion: Myocet improves the therapeutic index
of doxorubicin by significantly reducing cardiotoxicity
and grade 4 neutropenia and provides comparable
antitumor efficacy, when used in combination with
cyclophosphamide as first-line therapy for MBC.
J Clin Oncol 19:1444-1454. © 2001 by American
Society of Clinical Oncology.
Cardiac Toxicity (%) CHF (N) 6 21 p= 0,0001 0 5 p= 0,02 failure. The mechanism of doxorubicin cardiotoxicity involves the formation of a stable complex of drug with ferric
iron, which reacts with oxygen, forming superoxide anions,
hydrogen peroxide, and hydroxyl radicals. These free radicals cause lipid peroxidation.1-4 The injury is initially
Ba'st treatment
et al, J Cresults
lin Oncol 2001 subclinical, but continued
in progressive
Different anthracycline derivates for reducing cardiotoxicity
in cancer patients (Review)
van Dalen EC, Michiels EMC, Caron HN, Kremer LCM
Authors' conclusions This systema'c review of randomised trials provides evidence that nonpegylated liposomal anthracyclines reduced the overall risk of cardiotoxicity (RR = 0.38, 𝑃 < 0.0001) and the risk of This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library
clinical heart failure (RR = 0.20, 𝑃 = 0.02). 2010, Issue
3
http://www.thecochranelibrary.com
Published Van
online: 1
0 M
AY 2
010 Dalen EC et al. The Cochrane Library 2010
Phase III trial of liposomal doxorubicin and cyclophosphamide
compared with epirubicin and cyclophosphamide as first-line
therapy for metastatic breast cancer
S. Chan1,*, N. Davidson2, E. Juozaityte3, F. Erdkamp4, A. Pluzanska5, N. Azarnia6 & L.W. Lee6
On behalf of the Myocet Study Group†
1
City Hospital, Nottingham; 2North Middlesex Hospital, London, UK; 3Kaunas Medical Academy, Kaunas, Lithuania; 4Maasland Hospital, Sittard,
the Netherlands; 5Lodz Chemotherapy Clinic, Lodz, Poland; 6Elan Pharmaceuticals, Princeton, NJ, USA
Chemotherapy N. RR OS Received 16 April 2003; revised 3 June 2004; accepted 15 June 2004
(dose mg/m2) (%) (months) Cardiac Toxicity (%) CHF (N) Objective: To ascertain the efficacy and tolerability of non-pegylated liposomal doxorubicin
(Myocete) and epirubicin combined with cyclophosphamide in the first-line treatment of patients
metastatic breast
7,7 11 18.3 Myocet® 75 + Cy 600 with80 46 cancer.
Methods: One hundred and sixty anthracycline-naı̈ve metastatic breast cancer patients were random vs ised to receive Myocet (M; 75 mg/m2) or epirubicin (E; 75 mg/m2) in combination with cyclopho5,6 10 Epi 75 + Cy 600 sphamide
80 (C; 60039 mg/m2), every 3 weeks10 for up to eight cycles.
Outcome measures:
response = complete + partial response
rates), time to disease
P=0,02 P=0,007 P=0,005 ns Response (overall
progression, overall survival and cardiac function (left ventricular ejection fraction).
Results: Overall response rates were 46% and 39% for MC and EC treatment, respectively
(P = 0.42). MC was superior to EC with respect to median time to treatment failure (5.7 versus
4.4 months; P = 0.01) and median time to disease progression (7.7 versus 5.6 months; P = 0.02).
Median survival times were 18.3 and 16.0 months for MC and EC, respectively (P = 0.504). Unsurprisingly, given an equimolar comparison, neutropenia and stomatitis/mucositis were significantly
more common in patients who received MC. However, there was less injection site toxicity with
Chan et al, Annals Oncol 2004 MC. Both treatments showed a low incidence of cardiotoxicity.
Reduced cardiotoxicity and comparable efficacy in a phase III trial
of pegylated liposomal doxorubicin HCl (CAELYX™/Doxil®)
versus conventional doxorubicin for first-line treatment of
metastatic breast cancer
M. E. R. O’Brien1*†, N. Wigler2†, M. Inbar2, R. Rosso3, E. Grischke4, A. Santoro5, R. Catane6,
D. G. Kieback7, P. Tomczak8, S. P. Ackland9, F. Orlandi10, L. Mellars11, L. Alland11 & C. Tendler11
On behalf of the CAELYX Breast Cancer Study Group
1
Kent Cancer Center, Maidstone, UK; 2Ichilov Hospital, Tel Aviv, Israel; 3Oncologia Medica I Ist., Genova, Italy; 4Frauenklinik der Ruprecht-Karls-Universitat
Vosstrasse, Heidelberg, Germany; 5Oncologia Medica & Ematologie, Istituto Clinico Humanitas, Rozzano (MI), Italy; 6Sha’are Zedek Medical Center, Jerusalem,
Israel; 7Maastricht University Medical Center, Maastricht, The Netherlands; 8Oncology Clinic, Poznan, Poland; 9Newcastle Mater Misericordiae Hospital, Waratah,
10
11
Australia;
2 Hospital Dipreca, Santiago, Chile; Schering-Plough Research Institute, Kenilworth, NJ, USA
Chemotherapy N. RR OS ) (dose mg/m
(%) (months) Received 26 June 2003; revised 16 October 2003; accepted 16 December 2003
Caelix® 50 vs Adria 60 Cardiac Toxicity (%) CHF (N) Background: This study was designed to demonstrate that efficacy [progression-free survival (PFS)] of
21 HCl (PLD)] is non-inferior to4,7 254 CAELYX™33 [pegylated liposomal doxorubicin
doxorubicin with significantly0 less cardiotoxicity in first-line treatment of women with metastatic breast cancer (MBC).
with MBC and normal cardiac function were randomized to Patients
and methods: Women (n = 509)
receive either PLD 50 mg/m (every 4 weeks) or doxorubicin 60 mg/m (every 3 weeks). Cardiac event rates
4 19,6 22 255 38 were based on reductions in left ventricular ejection fraction as a function of cumulative anthracycline dose.
versus 7.8 months, respectively;
Results: PLD
P=0,001 P=0,001 ns with respect to PFS [6.9
ns and doxorubicin were comparable
2
2
hazard ratio (HR) = 1.00; 95% confidence interval (CI) 0.82–1.22]. Subgroup results were consistent. Overall
risk of cardiotoxicity was significantly higher with doxorubicin than PLD (HR = 3.16; 95%CI 1.58–6.31;
P <0.001). Overall survival was similar (21 and 22 months for PLD and doxorubicin, respectively; HR = 0.94;
95%CI 0.74–1.19). Alopecia (overall, 66% versus 20%; pronounced, 54% versus 7%), nausea (53% versus
37%), vomiting (31% versus 19%) and neutropenia (10% versus 4%) were more often associated with
doxorubicin than PLD. Palmar-plantar erythrodysesthesia (48% versus 2%), stomatitis (22% versus 15%) and
mucositis (23% versus 13%) were more often associated with PLD than doxorubicin.
Conclusions: In first-line therapy for MBC, PLD provides comparable efficacy to doxorubicin, with significantly reduced cardiotoxicity, myelosuppression, vomiting and alopecia.
O’Brien et al, Annals Oncol 2003 Key words: cardiotoxicity, pegylated liposomal doxorubicin
Pegylated Liposomal Doxorubicin Plus Docetaxel
Significantly Improves Time to Progression Without
Additive Cardiotoxicity Compared With Docetaxel
Monotherapy in Patients With Advanced Breast Cancer
Previously Treated With Neoadjuvant-Adjuvant
Anthracycline Therapy: Results From a Randomized
Phase III Study
From the Montefiore-Einstein Cancer
Center, Albert Einstein College of Medicine, Bronx, NY; City Oncology Hospital
#62; N.N. Blokhin Cancer Research
Center; and P.A. Herzen Oncology
Research Institute, Moscow; N.N.
Petrov Research Institute of Oncology
Chemotherapy (dose mg/m2) and City Clinical Oncology Dispensary,
Saint Petersburg, Russia; Regional
Oncology Dispensary and State Medical
Academy, Dnepropetrovsk; City Oncology Hospital, Kiev, Ukraine; and OrthoBiotech Oncology Research and
Development, Johnson & Johnson
Pharmaceutical Research and Development, Raritan, NJ.
Docetaxel 75 vs Docetaxel 60 + Caelix® 30 Submitted October 8, 2008; accepted
April 13, 2009; published online ahead
of print at www.jco.org on August 17,
2009.
Supported by Johnson & Johnson Pharmaceutical Research & Development.
Presented in part at the 31st San Antonio
Breast Cancer Symposium, December
10-14, 2008, San Antonio, TX.
Authors’ disclosures of potential conflicts of interest and author contributions are found at the end of this
article.
Clinical Trials repository link available on
JCO.org.
Corresponding author: Joseph A. Sparano,
MD, Montefiore-Einstein Cancer Center,
1825 Eastchester Rd, Bronx, NY 10461;
e-mail: [email protected].
The Acknowledgment and Appendix
are included in the full-text version
of this article; they are available
online at www.jco.org. They are
Joseph A. Sparano, Anatoly N. Makhson, Vladimir F. Semiglazov, Sergei A. Tjulandin, Olga I. Balashova,
Igor N. Bondarenko, Natalia V. Bogdanova, George M. Manikhas, Gennadiy P. Oliynychenko,
Valery A. Chatikhine, Sen H. Zhuang, Liang Xiu, Zhilong Yuan, and Wayne R. Rackoff
A
B
S
T
R
A
C
T
Purpose
To determine whether the combination of pegylated liposomal doxorubicin (PLD) and docetaxel
significantly prolongs time to disease progression compared with docetaxel alone without an
increase in cardiac toxicity in women with advanced breast cancer who had experienced relapse
at least 1 year after prior adjuvant or neoadjuvant anthracycline therapy.
N. RR TTP (%) (months) Patients and Methods
Cardiac Toxicity (%) PPS (%) This international, phase III study randomly assigned 751 patients to receive either docetaxel 75
mg/m2 (n ! 373) or PLD 30 mg/m2 followed by docetaxel 60 mg/m2 every 21 days (n ! 378) and
continued until disease progression or prohibitive toxicity. The primary end point was time to
progression (TTP). Secondary end points were overall survival (OS), objective response rate (ORR),
cardiac toxicity, and safety.
0 4 7 373 26 TTP from 7.0 to 9.8 months (hazard
Results
Treatment with PLD-docetaxel significantly improved median
ratio [HR] ! 0.65; 95% CI, 0.55 to 0.77; P ! .000001) and the ORR from 26% to 35% (P ! .0085).
OS was similar between the two groups (HR ! 1.02; 95% CI, 0.86 to 1.22). The incidence of grade
24 5 9.8 377 35 3 or 4 adverse events were similar (78% v 72%), although a higher incidence of hand-foot
syndrome (24% v 0%) and mucositis/stomatitis (12% v 1%) were observed in the PLD-docetaxel
ns decreases P=0,001 P=0,0001 P=0,008 combination.
Protocol-defined
left ventricular ejection fraction
and congestive heart
failure were reported in 5% and 1% in both treatment arms, respectively.
Conclusion The PLD-docetaxel combination was more effective than docetaxel alone in women with
metastatic breast cancer who had experienced relapse at least 1 year after prior adjuvant
anthracycline therapy without an increase in cardiac toxicity, although mucocutaneous toxicity was
more common.
J Clin Oncol 27:4522-4529. © 2009 by American Society of Clinical Oncology
INTRODUCTION
Despite multiple available treatment options, meta-
cumulative lifetime dose of 500 mg/m2, particularly
among patients who already received an anthracy7-9
Sparano et al J Clin Oncol 2009 cline as part
of neoadjuvant/adjuvant
therapy.
LD PLD doxorubicina liposomiale ~ 150 nm Superficie in PEG (polie'lenglicole) ~ 80 nm PLD
LD
metastatizzato della mammella
cardiaco aumentato
50 mg/m²
Non definito
10 – 33%
3 settimane
Definito
26% – 43%
complessiva (ORR)
Ridotta leucopenia e neutropenia
vs doxorubicina
Ridotta neutropenia di grado 4 (p=0.02)
Nessuno
Più casi di mucosite e stomatite (22%)
Più casi di rash (25%) e eritema (18%)
1. O’Brien et al. Ann Onco. 2004; 2. Keller et al. JCO 2004; 3. Batist G et al. J Clin Oncol 2001; 4. Harris L et al. Cancer. 2002
Azienda Sanitaria Firenze
16
Liposomal Anthracyclines and Trastuzumab ¤ In HER2-‐pos've breast cancer, the addi'on of trastuzumab to chemotherapy significantly increases response rate, 'me to progression, and overall survival compared with chemotherapy alone. However, when trastuzumab is combined with anthracyclines there is an increased risk of cardiac toxicity. ¤ Cardiotoxicity limited the use of anthracyclines in HER2-‐posi've breast cancer, and in consequence non-‐anthracycline-‐based regimens such as TCH were designed in order to avoid late-‐toxici'es, especially in adjuvant se8ng . ¤ As anthracyclines showed a high level of ac'vity in this subgroup of pa'ents, other strategies were developed also to design regimens using less cardiotoxic anthracyclines such as epirubicin (a less cardiotoxic analog than doxorubicin) at limited doses or liposomal anthracyclines in combina'on with trastuzumab. Azienda Sanitaria Firenze
17
y guest on September 23, 2012
apy, and 46.5% received no chemotherapy. Anthracycline and trastuzumab recipients were younger, with fewer
comorbidities than recipients of other chemotherapy or none. Compared with no chemotherapy, the risk of HF/
CM was higher in patients treated with anthracycline alone (adjusted HR = 1.40, 95% CI = 1.11 to 1.76), although the
increased risk was similar to other chemotherapy (adjusted HR = 1.49, 95% CI = 1.25 to 1.77); the risk was highly
increased in patients treated with trastuzumab alone (adjusted HR = 4.12, 95% CI = 2.30 to 7.42) or anthracycline
plus trastuzumab (adjusted HR = 7.19, 95% CI = 5.00 to 10.35).
Risk of Heart Failure in Breast Cancer Patients After
Anthracycline and Trastuzumab Treatment: A Retrospective
Cohort Study
Conclusions
Anthracycline and trastuzumab were primarily used in younger, healthier women and associated with increased
Erin J. Aiello Bowles, Robert Wellman, Heather Spencer Feigelson, Adedayo A. Onitilo, Andrew N. Freedman, Thomas Delate,
HF/CM risk compared with no chemotherapy. This population-based observational study complements findings
Larry A. Allen, Larissa Nekhlyudov, Katrina A. B. Goddard, Robert L. Davis, Laurel A. Habel, Marianne Ulcickas Yood,
from clinical trials on cancer treatment safety.
Catherine McCarty, David J. Magid, Edward H. Wagner; for the Pharmacovigilance Study Team
J Natl Cancer Inst 2012;104:1293–1305
Manuscript received January 05, 2012; revised June 13, 2012; accepted June 18, 2012.
Correspondence to: Erin J. Aiello Bowles, MPH, Group Health Research Institute, 1730 Minor Ave, Ste 1600, Seattle, WA 98101 (e-mail: [email protected]).
jnci.oxfordjournals.org
sion models were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) with adjustment for age
at diagnosis, stage, Cancer Research Network site, year of diagnosis, radiation therapy, and comorbidities.
JNCI | Articles 1293
Among 12 500 women (mean age = 60 years, range = 22–99 years), 29.6% received anthracycline alone, 0.9%
received trastuzumab alone, 3.5% received anthracycline plus trastuzumab, 19.5% received other chemotherapy, and 46.5% received no chemotherapy. Anthracycline and trastuzumab recipients were younger, with fewer
comorbidities than recipients of other chemotherapy or none. Compared with no chemotherapy, the risk of HF/
CM was higher in patients treated with anthracycline alone (adjusted HR = 1.40, 95% CI = 1.11 to 1.76), although the
increased risk was similar to other chemotherapy (adjusted HR = 1.49, 95% CI = 1.25 to 1.77); the risk was highly
increased in patients treated with trastuzumab alone (adjusted HR = 4.12, 95% CI = 2.30 to 7.42) or anthracycline
plus trastuzumab (adjusted HR = 7.19, 95% CI = 5.00 to 10.35).
Conclusions
Anthracycline and trastuzumab were primarily used in younger, healthier women and associated with increased
HF/CM risk compared with no chemotherapy. This population-based observational study complements findings
from clinical trials on cancer treatment safety.
J Natl Cancer Inst 2012;104:1293–1305
Breast cancer is one of the most common cancers in the United
States with an estimated 232 620 new diagnoses in 2011 (1).
Data from clinical trials indicate that anthracycline use is associated with an approximate 2% increase (10–14) in heart failure
Downloaded from http://jnci.oxford
Results
Downloaded from http://jnci.oxfordjournals.org/ by guest on September 23, 2012
Data from clinical trials indicate that anthracycline use is assoBreast cancer is one of the most common cancers in the United
States with an estimated 232 620 new diagnoses in 2011 (1). ciated with an approximate 2% increase (10–14) in heart failure
cardiomyopathy
(HF/CM)
incidence,
and anthracycline
ChemotherapeuticBackground
regimens for invasive
breast
in women thatand/or
Clinical
trialscancer
demonstrated
women
treated for breast
cancer
with anthracycline
or trastuzumab are at
followed
by
trastuzumab
is
associated
with
an
approximate 4%
include neoadjuvant or adjuvant anthracycline
in
combination
with
increased risk for heart failure and/or cardiomyopathy (HF/CM), but the generalizability
of these findings is
increase
(15–19).
Clinical trial
were critical
in their
leading
to
cyclophosphamide (2). A major advance
in breast
treatment
unknown.
Wecancer
estimated
real-world
adjuvant
anthracycline
andfindings
trastuzumab
use and
associations
with inciprescribing
warnings
and
protocols
for
regular
cardiac
function
has been the incorporation of trastuzumab,
a
monoclonal
antident HF/CM.
body against HER2/neu. Approximately 20%–25% of women with monitoring before and during treatment (20–22). However, trials
Methods
We
a population-based,
retrospective
study of(eg,
12 500
diagnosed
with incident, invasive
exclude cohort
older women
agedwomen
≥ 70 years)
and women
breast cancer overexpress
HER2 and
areconducted
recommended
for trastu- typically
breastof
cancer
from January
1, 1999
through
31, 2007,
at eight integrated
Cancerbetween
Research Network health
with
majorDecember
comorbidities;
therefore,
the association
zumab therapy following the completion
anthracycline
therapy
systems.
Using administrative
and pharmacy
codes, weuse
identified
anthracycline,
trastuzumab, and other
anthracycline
and/or trastuzumab
and HF/CM
in this popula(3–5). Randomized clinical trials have
demonstrated
that these reg- procedure
chemotherapy
We identified
incident
following The
chemotherapy
initiation
assessed risk of HF/CM
is not HF/CM
well understood.
effectiveness
of theseand
treatments
imens are highly effective in improving
disease-freeuse.
survival
(6–9); tion
with time-varying chemotherapyand
exposures
vs no chemotherapy.
proportional
risk of cardiotoxicity
may differMultivariable
in communityCox
practice.
Three hazards regreshowever, side effects are not minimal.
Phase I/II trials of NPLA (Myocet®) in combina:on with Trastuzumab: Sefng Autor Treatment (dose mg/m2) N. RR (%) PFS (months) Cardiac Toxicity (%) CHF (%) MBC anthra pretr. Myocet®70 q21+ Trastuzumab (w) 37 58 nr 37 5 Myocet®60 q21+ Paclitaxel 80 (w) + Trastuzumab (w) + 69 98 23 17 0 Myocet®50 q21+ Docetaxel 75 q21 + Trastuzumab (w) 31
66
13
10
0
Myocet®50 q21+ Docetaxel 30 (gg2,9) + Trastuzumab (w) 45 56 10.9 4 0 Theodoulou 2002 LABC / MBC chemo naive Cortes 2009 MBC 1st line Venturini 2010 MBC 1st line Amadori 2011 Azienda Sanitaria Firenze
19
Phase I/II trials of PLA (Caelix®) in combina:on with Trastuzumab: Sefng Autor Treatment (dose mg/m2) N. RR (%) PFS (months) Cardiac Toxicity (%) CHF (%) MBC anthra pretr. Caelix®50 q28 + Trastuzumab (w) 30
52
12
10
0
Caelix®40 q21+ Trastuzumab (w) 12
66
nr
25
0
Caelix®40 q28+ Trastuzumab (w) 16
50
9.6
0
0
Caelix®30 + Docetaxel 60 q21 + Trastuzumab (w) 46
45
10.6
25
0
Chia 2006 MBC anthra pretr Andreopoulou 2007 MBC 1st line S:ckeler 2009 MBC 1st line Wolff 2010 Azienda Sanitaria Firenze
20
Liposomal Anthracyclines in metasta:c sefng ¤ In pa'ents with metasta'c breast cancer, liposomal anthracyclines have proven to be as effec've and less toxic when compared face to face with conven'onal anthracyclines, allowing a longer period of treatment and a higher cumula've dose of the anthracyclines. ¤ The combined analysis of available data indicates an overall reduc'on in risk for both cardiotoxicity and clinical heart failure. ¤ The safety of liposomal anthracyclines endorsed its use in pa'ents with some cardiac risk factors. Azienda Sanitaria Firenze
21
Liposomal Anthracyclines in combina:on with Trastuzumab: ¤
In HER2-‐posi've breast cancer, the addi'on of trastuzumab to chemotherapy significantly increased response rate, progression-‐free survival, and overall survival. ¤
Ini'al studies demonstrated synergy when trastuzumab was combined with anthracyclines, but their excessive cardiac toxicity limited their use, and nonanthracycline therapeu'c strategies were therefore designed. ¤
Liposomal anthracyclines have proven to be effec've and safe when combined with trastuzumab both in advanced and early breast cancer. Of par'cular interest is the use of the combina'on of liposomal anthracyclines plus trastuzumab in pa'ents with early and HER2-‐overexpressing breast cancer, as this is probably the subgroup that would benefit most from a treatment with anthracyclines. ¤
The poten'al clinical benefit of anthracyclines in this se8ng should be inves'gated in a clinical trial comparing a regimen with liposomal anthracyclines versus a nonanthracyclines combina'on. Azienda Sanitaria Firenze
22
Grazie per l’attenzione