Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
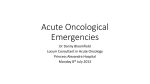
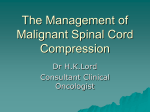
Malignant Spinal Cord Compression CCPN Round – 15 March 2016 Definition of Malignant spinal cord compression (MSCC) Comprehensive indentation, displacement, or encasement of the thecal sac that surrounds spinal cord or cauda equina by spinal epidural metastases CCON Neuro-Oncology DSG – Loblaw et al – JCO 2005 Compression of the dural sac and its contents (spinal cord and/or cauda equina) by an epidural tumor mass Minimum radiologic evidence is indentation of the theca at the level of clinical features Subclinical or Impending MSCC: Presence of the radiographic features in the absence of the clinical features Malignant spinal cord compression (MSCC) Occurs in 5-10% of all cancer patients during the course of their disease In the last 5 years of life, 2.5% of patients dying with cancer will have at least one Loblaw et al – Clin Oncol - 2003 episode of MSCC Most common cancers causing MSCC are breast, prostate, and lung cancers, each account for about 20%, and myeloma, lymphoma, renal cancer 5-10% In 20% of cancer patients with metastatic disease, MSCC is the initial manifestation of cancer, 30% of these patients have lung cancer Sites of MSCC: cervical spine 10% - thoracic spine 60-80% - lumbosacral spine 15-30% Multi-level compression seen in 10-40% of patients Epidural cord compression results from direct extension of bony metastases Vertebral body (1a) or posterior elements (1b) Paraspinal tumor infiltrating through neural foramina (2) Subdural (4) and Intramedullary (5) metastases Soft tissue epidural mass in 75%, bone collapse with fragments in 25% Spinal Cord Compression Cauda Equina Syndrome MSCC: Compression of the thecal sac by tumor in the epidural space, either at the level of the spinal cord (above L1-L2) or cauda equina Pathophysiology: Ischemia and Vasogenic Cord Edema at the Level of Compression Epidural MSCC most often related to soft tissue metastases causing compression Direct arterial embolization of cancer cells in to the bone marrow of vertebra Vertebral body mass impringes on the thecal sac, spinal cord, and epidural venous plexus Pathologic vertebral body fractures can impringe on the thecal sac MSCC is vascular in nature: Disrupted blood flow for both venous and arterial circulation Prostaglandin E2 and Vascular endothelial growth factor (VEGF) release Cord white-matter edema causing necrosis and gliosis Venous compression and vasogenic edema of white matter: Slow development of MSCC and neurologic deficits could be reversible Arterial flow disruption causing ischemia and spinal cord infarction: Faster development of MSCC and irreversible neurologic deficits Pathogenesis of spine metastases and MSCC Metastases in the bone marrow of vertebra by venous or arterial routes Cancer cells in the bone marrow invade into the spinal canal through the foramina of the vertebral veins rather than destroying the cortical bone Cancer cells growing in an infiltrative fashion posteriorly into spinal canal and soft tissue mass compresses the cord predominantly from an anterior direction Disruption of blood flow for venous and/or arterial circulation Arguello et al – Cancer J - 1990 Clinical Presentation Back pain : 70-95% incidence Motor deficits: 60-90% incidence Sensory deficits: 45-90% incidence Autonomic (bladder/bowel) dysfunction: 40-55% Rate of progression of motor deficits and Status of ambulation before initiation of treatment indicate probability of meaningful neurologic recovery Clinical Evaluation Clinical history and detailed neurologic examination Functional assessment and ambulatory status using Frankel Grading system MRI of the Entire Length of Spine – Gold Standard MRI sensitivity 93% - specificity 97% - overall accuracy 95% Complete MRI study: T1- and T2-weighted sagittal images – T1- and T2-weighted axial images A sagittal sequence of the entire spine is necessary as multi-level compression ~ 10-40% MRI provides superior resolution of soft tissue structures of the spine including cord MRI elucidates the bone-to-soft-tissue interface, providing accurate anatomical detail of tumor invasion and compression of bone, neural, and paraspinal structures MRI can discriminate MSCC from benign conditions like: Acute osteoporotic compression fracture and Spondylodiscitis causing cord compression If MRI facility is not available or in patients with cardiac pacemakers, high-resolution CT scan or spinal CT myelogram is an alternative option Prognosis or Outcome Measures (Abrahm et al – Support Oncol – 2004) Median survival of patients with MSCC depends on 1. Type of tumor (radio-responsive or radio-resistant) 1-year survival from diagnosis of MSCC: Lymphoma and myeloma – 40% - Breast – 25% - Prostate – 20% - Lung – 5% (Loblaw et al – CCON – JCO) 2. Patient’s performance status 3. Pre-treatment ambulatory status is the most important predictor of ambulation post-treatment and of improved survival 4. Duration of motor deficit development before the onset of RT is important prognosticator Predicting overall survival in patients with MSCC treated with RT Prognostic factors: 1. Tumor type (lymphoma/myeloma – breast ca – prostate ca – other ca) 2. Interval between diagnosis of cancer and MSCC ( < 12 versus > 12 months) 3. Other bone metastases 4. Visceral metastases 5. Ambulatory status before treatment 6. Duration of motor deficits ( < 14 versus > 14 days) Management of MSCC Since MSCC is usually associated with inadequate control of the primary tumor, the goal of treatment is palliative and directed at maintaining ambulation, decreasing tumor bulk, and relieving pain (Quinn and DeAngelis – Semin Oncol – 2000) Treatment Options: Symptomatic therapy – Steroids – RT – Surgery – Bisphosphonates Symptomatic therapy: Pain control – Spinal instability – Bladder and bowel function – Psychological and social distress Steroid Therapy for MSCC Steroid should be used in patients with newly diagnosed MSCC causing cord dysfunction Dexamethasone is most widely used steroid – Optimal dosage is controversial Recommended regimen of Dexamethasone: 10 mg IV bolus followed by maintenance 16 mg/day IV/PO, tapering over several weeks Dexamethasone inhibits prostaglandin E2 and VEGF production and activity, which leads to a decrease of the vasogenic edema In young patients presenting with an undiagnosed spinal mass with no previous history of cancer, steroids should be avoided until the diagnosis is made (lymphoma) Loblaw et al – CCON Neuro-oncology DSG – JCO - 2005 Conventional Radiation Therapy Alone Indications for RT alone: 1. Expected survival < 6 months 2. Radio-responsive tumors 3. Patient unable to tolerate an operation 4. Duration of neurologic deficit below the level of cord compression > 24-48 hours 5. Multilevel or diffuse spinal involvement Radiotherapy Outcome & Dose Fractionation 30 Gy in 10 fractions – 20 Gy in 5 fractions – 8 Gy in 1 fraction Choice of RT dose fractionation depends on patient’s: Disease Status and Expected Survival Pre-treatment Ambulatory Status Pre-treatment Motor function and Sensory deficit Different dose-fractionation schedules in pts with MSCC treated with RT alone Rades et al – JCO supplement 2009 Multicenter nonrandomized study of 265 patients with MSCC comparing short-course RT (8Gy/1Fx or 20Gy/5Fx) to longer-course RT (30Gy/10Fx – 40Gy/20Fx) Both regimens were of similar effectiveness regarding post-RT motor function Improved motor function in 30% of patients after SCRT and LCRT Further progression of motor deficits was prevented in another 55% of patients in both arms 1-year local control: 80% after LCRT and 60% after SCRT Better functional outcome associated with: young age - good performance status – radio-responsive tumors - 1-2 vertebral involvement - being ambulatory before RT – slow development of MSCC Effectiveness of SCRT and LCRT have not been evaluated in a prospective phase III randomized trial 65M – 40 PYS – PS ECOG 2-3 4/12 cough – hemoptysis – dyspnoea – fatigue 2/12 mid and lower back pain 1/52 weakness and numbness in legs Motor deficits in legs – ambulatory with assistance No bladder/bowel dysfunction PET/CT: RUL mass – mediastinal nodes – bone mets – right adrenal mets Bone scan: multi-level bone mets in axial skeleton MRI: epidural cord compression at mid T-spine and L-spine FNAC RUL mass: PD adenocarcinoma Stage IV NSCLC with bone and adrenal mets (T2 N2 M1) Selection of appropriate treatment individualized to a specific patient Stage IV NSCLC with adrenal and multiple bone metastases - MSCC Ambulatory - with assistance Time to develop motor deficits - 1 week Management: 1. Dexamethasone 4 mg QID IV/PO 2. Urgent RT: 8Gy/1 Fx – 20 Gy/ 5 Fx – 30 Gy/10 Fx 3. Consult to Spine Neurosurgery - NO Surgery for MSCC Patients with clinical/radiologic evidence of MSCC but no previous diagnosis of cancer (or remote cancer) Patient’s life expectancy > 6 months Radio-resistant tumors Unstable spine or bony fragment causing cord compression Previous RT and inability to receive further RT Surgery should be performed within 24 hours: high probability of improvement in ambulation – motor function - bladder/bowel function Anterior approach is preferable: 85% of metastases causing spinal instability or neurologic deficits arise anteriorly in the vertebral body Tumor is debulked and bony fragments removed, the void is filled with acrylate cement, the spine is mechanically stabilized with metal prosthesis Posterior Decompression Laminectomy Any neurosurgeon can perform with minimal intraoperative risk to the patient, and no spinal column reconstruction or stabilization To establish pathologic diagnosis 15-55% of patients who underwent PDL remained ambulatory post-surgery Neurologic benefit to the patient is minimal – increases spinal instability – worsen the pain and neurologic deficits PDL alone without spine stabilization is not recommended Anterior Spinal Decompression Surgery Approaches depends on the location of the tumor: Anterior – Posterolateral Resection involves: Decompress the cord of any malignant compression Reconstruction with plate & screw and Stabilization of the spinal column Anterior Decompression Surgery plus Spine Stabilization is superior to RT alone Klimo et al – Neuro-Oncology – 2005 24 reports (n-1000) treated with Surgery (anterior decompression & spine stabilization) and 4 reports (n- 545) treated with RT alone Post-treatment ambulatory rates: 85% for Surgery – 65% for RT alone 60% of non-ambulatory patients in Surgery group regained the ability to walk compared to 30% patients in RT alone group Indications for Decompression surgery with spinal stabilization (Klimo et al) Radio-resistant tumors Obvious spinal instability Clinically significant neural compression secondary to bone fragment or spinal deformity Progression of neurologic deficits during or immediately after RT 55F – No comorbid conditions – PS ECOG 0-1 Left nephrectomy in 2005 for renal cell carcinoma of left kidney 2010: upper back pain for 3/12 - No neurologic deficits - Ambulatory MRI: Lytic lesions in two upper thoracic vertebras with epidural soft tissue mass invading spinal canal and impending cord compression CT scan chest – abdomen – pelvis: no local recurrence in left renal bed – no lymphadenopathy or visceral metastases CT brain clear – Bone scan: metastases in two upper thoracic vertebras Establish tissue diagnosis from the spine lesion Left Nephrectomy for RCC 2005 MSCC - 2010 Selection of appropriate treatment individualized to a specific patient Past history of Renal cell cancer of left kidney treated with nephrectomy (2005) Solitary bone metastases – no visceral metastases – no local recurrence in left renal bed Interval from previous cancer diagnosis – 5 years Ambulatory at presentation of MSCC – yes No motor deficits at presentation – subclinical MSCC on MRI scan Management: 1. Consult Spine Neurosurgery: Anterior cord decompression surgery and spine stabilization - establish pathologic diagnosis 2. May need PORT 3. Lymphoma/Myeloma ? Direct decompression surgical resection plus PORT versus RT alone in patients with MSCC: A randomised trial Patchell et al – Lancet - 2005 (University of Kentucky) We assessed the efficacy of direct decompression surgery for patients with MSCC Randomised multi-institutional trial, patients assigned to either surgery followed by PORT (n=50) or RT alone (n=50) Surgery involved spinal cord decompression and maximal tumor debulking and spine stabilization RT dose for both treatment groups (30 Gy in 10 fractions over 2 weeks) Primary endpoint was the ability to walk (Ambulation) Secondary endpoints: Urinary continence - muscle strength - functional status – need for corticosteroids and opioid analgesics - survival time Findings: After an interim analysis the study was stopped because the criterion of a predetermined early stopping rule was met 125 patients were assessed for eligibility before the study closed and 100 were randomised Significantly more patients in the surgery group (42/50, 84%) than in the RT group (29/50, 57%) were able to walk after treatment (p=0·001) Patients treated with surgery also retained the ability to walk significantly longer than did those with RT alone (median 122 days versus 13 days, p=0·003) 32 patients entered the study unable to walk; significantly more patients in the surgery group regained the ability to walk than patients in the RT group (10/16 versus 3/16 ) Need for corticosteroids and opioid analgesics was significantly reduced in surgical group Interpretation: Direct decompression surgery plus PORT is superior to RT alone for patients with MSCC Limitations of the Patchell study was the patient selection criteria Highly radio-sensitive tumors like lymphoma, myeloma, SCLC were excluded from both arms KM estimates of length of time all pts remained ambulatory after treatment and pts who were ambulatory at study entry remained ambulatory after treatment Timing of PORT after Cord Decompression & Spine Stabilization 2 weeks interval between spine surgery and PORT PORT dose - 30 Gy in 10 fractions over 2 weeks Detrimental consequences of early initiation of PORT after surgical reconstruction: -Impaired wound healing -Impaired bone graft incorporation (arthrodesis) 3-4-week delay in initiation of PORT after surgical decompression and spine stabilization (Sciubba and Gokaslan – Johns Hopkins Neurosurgery unit – J Neurosurg Spine 2010) RT alone in patients with MSCC 1. Expected survival < 6 months 2. Radio-responsive tumors 3. Patient unable to tolerate an operation 4. Duration of neurologic deficit below the level of compression > 24-48 hours 5. Diffuse multi-level spinal involvement B. No significant difference in treatment outcome (improved motor function and post-RT ambulatory status) with different RT dose fractionation C. If expected survival < 6 months: 8 Gy/1 Fx or 20 Gy/5 Fx If expected survival > 6 months: 30 Gy/10 Fx or 40 Gy/16 Fx D. In-field recurrence less with higher RT dose E. Pts with good prognostic factors and radio-resistant tumors (melanoma, renal cell cancer) should be considered for dose-escalation IMRT/SBRT Surgery + PORT in patients with MSCC Strict criteria for appropriate patient selection Patients with clinical/radiologic evidence of MSCC but no previous diagnosis of cancer Radio-resistant tumors Unstable spine or bony fragment causing cord compression Previous RT and inability to receive further RT If surgery is indicated, should be performed immediately (within 24 hours) Anterior approach is recommended as 85% of metastases causing spinal instability or neurologic deficits arise anteriorly from the vertebral body Using anterior approach, the tumor is debulked and bony fragments removed, the void is filled with acrylate cement, the spine is mechanically stabilized with metal prosthesis For posteriorly placed tumors, posterior laminectomy with stabilization is recommended PORT should be initiated 3-4 weeks after surgical resection and spine reconstruction High-Precision RT Young patients with good performance status may be considered for SBRT Aim of HPRT is to achieve better sparing of critical normal tissues and/or dose escalation to the site of metastatic disease in the spine If the tumor is invading into the spinal canal, fractionated SBRT is preferred to reduce the risk of radiation-induced myelopathy and vertebral body fracture Recent reports suggest that HPRT (SBRT) is safe and effective, but has not been compared to surgery and conventional EBRT Young patients with good PS and radio-resistant tumors (melanoma, renal cancer) should be considered for dose-escalation fractionated SBRT SBRT can be an effective salvage treatment in patients with in-field recurrence after prior convention EBRT for MSCC Pros and Cons of HPRT – Spine Neurosurgeon’s prospective (Sciubba and Gokaslan – John Hopkins University – J Neurosurg Spine 2010) Convention RT delivers inadequate dose to the target and not recommended if the tumor histology is radio-resistant Advent of HPRT (SRS – SBRT) has led to a fundamental change in the treatment paradigm for spine metastases and MSCC High dose to the target with maximal sparing of critical neural structures with HPRT provides superior local disease control – preservation of neurologic function – pain relief HPRT can not correct spinal instability or deformity causing pain or neurologic dysfunction HPRT can not correct cord compression caused by pathologic vertebral body fracture and retropulsion of bone fragment into the spinal canal Retreatment of MSCC for in-field recurrence after previous EBRT A second episode of MSCC occurs in up to 15% of patients Decompression surgery would be first choice of treatment – surgery is possible in 10-15% of these patients with recurrent MSCC Re-irradiation may result in an increased risk of radiation-induced myelopathy For re-irradiation after conventional RT, HPRT like SBRT be considered Recent HPRT studies report improved motor function in 40-85% of re-irradiated patients Radiotherapy or Surgery in Spinal Cord Compression? The Choice Depends on Appropriate Patient Selection Role of radiotherapy for metastatic epidural spinal cord compression (MESCC) – Dirk Rades RT alone is the most common treatment for metastatic epidural spinal cord compression (MESCC) Decompressive surgery followed by PORT is generally indicated only in 10–15% of MESCC cases CT has an unclear role and may be considered for selected patients with lymphoma or myeloma If RT alone is given, it is important to select the appropriate regimen Similar functional outcomes can be achieved with short-course and longer-course RT regimens Longer-course RT is associated with better local control of MESCC than short-course RT Patients with a more favorable survival prognosis (expected survival of ≥6 months) should receive longer-course RT, as they may live long enough to develop a recurrence of MESCC Patients with an expected survival of <6 months should be considered for short-course RT Recurrence of MESCC in the previously irradiated region after short-course RT may be treated with another shortcourse of RT After primary administration of longer-course RT, decompressive surgery should be performed if indicated Alternatively, re-irradiation can be performed using high-precision RT (SBRT) techniques to reduce the cumulative dose received by the spinal cord Larger prospective trials are required to better define the appropriate treatment for the individual patient