Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
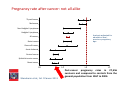
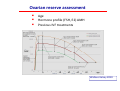
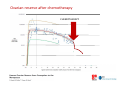
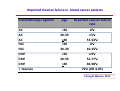
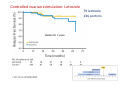
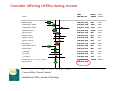
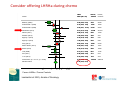
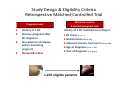
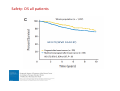
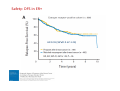
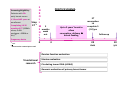
La preservazione della fertilità in oncologia: il carcinoma mammario come paradigma Olivia Pagani Centro di Senologia della Svizzera Italiana Centro di Senologia della Svizzera Italiana Pregnancy rate after cancer: not all alike Thyroid cancer Melanoma Non-Hodgkin's lymphoma Hodgkin's lymphoma Analysis adjusted for education level, previous pregnancy age All cancers Brain tumors Germ cell tumors Acute leukemia Cervical cancer Epithelial ovarian cancer Breast cancer 0.0 Stensheim et al; Int J Cancer 2011 0.5 1.0 1.5 Post-cancer pregnancy rates in 27,556 survivors and compared to controls from the general population from 1967 to 2004. Premenopausal Early Breast Cancer Fertility Considerations • Chemotherapy may cause menopause or reduce ovarian reserve • Delaying pregnancy for 5-10 years of endocrine therapy will reduce fertility • Fertility after breast cancer treatment is age and regimen dependent Fertility concerns of breast cancer patients 620 patients, median age 37 years 51% concerned about fertility 68% discussed fertility issues before starting therapy 10% used fertility preservation strategies Ruddy C J Clin Oncol 32:1151, 2014 Fertility concerns of breast cancer patients 515 ER+ patients <45 y/o in whom TAM was indicated 149 (28.9%) did not start or discontinued TAM Fertility concerns associated with: Non initiation (OR 5.04, 95%CI=2.29-11.07) Early discontinuation (HR 1.78, 95%CI=1.09-3.38) Ovarian reserve assessment Age Hormone profile (FSH, E2) AMH Previous IVF treatments NGF 0 20 30 40 50 age Wallace Kelsey 2010 Ovarian reserve after chemotherapy CHEMOTHERAPY Reported Ovarian failure in breast cancer patients Chemotherapy regimen AC AC AC FAC FAC CMF CMF CMF + Taxanes Age Reported ovarian failure rate <30 30-39 >40 <30 30-39 <30 30-39 c >40 0% 13% 57-63% 0% 10-25% 19% 51-77% 83-98% 79% (OR 4.05) Chung & Meirow 2012 What are the available options for fertility preservation? • Embryo cryopreservation: delay treatment for 1 month to undergo 1 cycle of hormone stimulation, oocyte retrieval and in vitro fertilization • Cryopreservation of mature oocytes: less effective, efficiency improving • In vitro follicle maturation, ovarian tissue cryopreservation and transplantation Discuss at the early beginning the possibility of infertility as a risk of cancer treatment Refer to appropriate specialists as early as possible Christinat, Pagani. Maturitas 73 (2012) 191– 196 Early referral ID: initial diagnosis, FPC: fertility preservation counseling BS: breast surgery, OS/OR: ovarian stimulation/oocyte retrieval Early referral ID: initial diagnosis, FPC: fertility preservation counseling BS: breast surgery, OS/OR: ovarian stimulation/oocyte retrieval Embryo freezing for fertility preservation Currently the most widely used method. Cycle success rate– according with ovarian reserve. In cancer patients- thousands of patients worldwide. IVF in breast cancer patients - Dilemmas Time needed for IVF – flexible Early referral more cycles. Older patients- low ovarian reserve. No partner –Egg freezing or Donor sperm. Hormone sensitive tumors. Aromatase inhibitor (Letrozole) reduce E2 levels. Tamoxifen blocks Estrogen receptors. Egg Freezing for fertility preservation Indications No partner. Breast cancer patients before chemotherapy. BRCA mutation carriers before BSO. 90% vitality and fertilization rate after thawing 8-12 frozen oocytes - 30% probability of a baby Controlled ovarian stimulation: Letrozole 79 letrozole 136 controls Median FU 2 years Ovarian tissue cryopreservation Objectives Fertility preservation using stored ovarian tissue WORKS! Ovarian tissue storage enables TREATMENT FLEXIBILITY. SAFETY ISSUES. Operation – laparoscopy Children born after ovarian transplantation. A review of 13 live births. Age at tissue collection 19-36 Previous chemotherapy 40%. IVF / Spontaneous pregnancy 50%. Pregnancy results- normal babies 100%. Donnez J, Silber S, Andersen CY, Demeestere I, Piver P, Meirow D, Pellicer A, Dolmans MM. Ann Med 2011 .Jan 13 Many centers, sporadic cases, different conditions. Success rate unknown. The risk of cancer cells in the ovaries of breast cancer patients Risk of breast cancer cells metastasis. Risk of primary ovarian cancer in BRCA mutation carriers. Consider offering LHRHa during chemo Odds Events, Events, Author Ratio (95% CI) Treated Controls Badawy (2009) 0.06 (0.02, 0.20) 4/39 26/39 Sverrisdottir 1 (2009) 0.19 (0.04, 1.06) 14/22 18/20 Sverrisdottir 2 (2009) 2.03 (0.31, 13.27) 27/29 20/23 Del Mastro (2011) 0.27 (0.14, 0.54) 13/148 35/133 Gerber (2011) 0.56 (0.19, 1.62) 9/30 13/30 Munster (2012) 1.09 (0.22, 5.52) 4/26 3/21 Elgindy 1 (2013) 0.76 (0.18, 3.25) 4/25 5/25 Elgindy 2 (2013) 1.00 (0.25, 4.00) 5/25 5/25 Song (2013) 0.50 (0.25, 1.03) 15/89 27/94 Karimi-Zarchi (2014) 0.05 (0.01, 0.29) 2/21 14/21 Moore (2015) 0.30 (0.10, 0.87) 5/66 15/69 Li M (2008) 0.31 (0.11, 0.89) 8/31 17/32 Sun (2011) 0.38 (0.06, 2.30) 3/11 5/10 Li Jw (2014) 0.44 (0.04, 4.35) 1/54 3/73 Fixed effect (I≤ = 47.1%, p = 0.026) 0.34 (0.25, 0.46) 114/616 206/615 Random effect 0.36 (0.23, 0.57) .01 .1 .5 Favors LHRHa / Favors Controls Lambertini et 2015, Annals of Oncology 1 2 8 14 Consider offering LHRHa during chemo Odds Events, Events, Author Ratio (95% CI) Treated Controls Badawy (2009) 0.06 (0.02, 0.20) 4/39 26/39 Sverrisdottir 1 (2009) 0.19 (0.04, 1.06) 14/22 18/20 Sverrisdottir 2 (2009) 2.03 (0.31, 13.27) 27/29 20/23 Del Mastro (2011) 0.27 (0.14, 0.54) 13/148 35/133 Gerber (2011) 0.56 (0.19, 1.62) 9/30 13/30 Munster (2012) 1.09 (0.22, 5.52) 4/26 3/21 Elgindy 1 (2013) 0.76 (0.18, 3.25) 4/25 5/25 Elgindy 2 (2013) 1.00 (0.25, 4.00) 5/25 5/25 Song (2013) 0.50 (0.25, 1.03) 15/89 27/94 Karimi-Zarchi (2014) 0.05 (0.01, 0.29) 2/21 14/21 Moore (2015) 0.30 (0.10, 0.87) 5/66 15/69 Li M (2008) 0.31 (0.11, 0.89) 8/31 17/32 Sun (2011) 0.38 (0.06, 2.30) 3/11 5/10 Li Jw (2014) 0.44 (0.04, 4.35) 1/54 3/73 Fixed effect (I≤ = 47.1%, p = 0.026) 0.34 (0.25, 0.46) 114/616 206/615 Random effect 0.36 (0.23, 0.57) .01 .1 .5 Favors LHRHa / Favors Controls Lambertini et 2015, Annals of Oncology 1 2 8 14 GRAVIDANZA DOPO UN TUMORE AL SENO Study Design & Eligibility Criteria Retrospective Matched-Controlled Trial Matched controls 3 controls/pregnant case Pregnant cases 1. 2. 3. 4. History of 1 BC Became pregnant after BC diagnosis No evidence of relapse before becoming pregnant Known ER-status History of 1 BC matched according to 1.ER status (+ vs. -) 2.Nodal status (N0 vs. N+) 3.Adjuvant chemo, hormonal (Yes vs. No) 4.Age at diagnosis (< vs. > 35) 5.Year of diagnosis (± 5 years) 1,207 eligible patients Safety: OS all patients HR 0.72 (95%CI 0.54-0.97) Safety: DFS in ER+ HR 0.91 (95%CI 0.67-1.24) Screening/eligibility: Patients with ER+ early breast cancer ≥ 18 and ≤42 years at enrollment Completing 18-30 months of ET (SERMs alone, GnRH analogue + SERM or AIs) 1 E N R O L Stop L ET 2 M 3 E months N wash T out POSITIVE SCHEMA Up to 2 years’ break to allow conception, delivery ± breast feeding ET resumption to complete 5 (-10) yrs Follow-up Pregnancy desire 0 1 + CT 3 2 No more than 1 month prior enroll. Ovarian function evaluation Translational research Uterine evaluation Circulating tumor DNA (ctDNA) Genomic evaluation of primary breast tumor 24 mos 10 yrs Conclusioni Evaluate sterilization risks. Choose fertility preservation approach. Egg, embryo freezing; results similar to non-cancer patients. Not post exposure to chemotherapy. Ovarian tissue freezing- established clinical method. Grazie



















![Genistein [446-72-0] - Università degli Studi di Roma "Tor Vergata"](http://s1.studyres.com/store/data/001069358_1-826841ed5b5b39775155b3058987503a-150x150.png)
![“Basic and translational oncology” [Selezionare la data] Italian](http://s1.studyres.com/store/data/003369983_1-0c2f97f3754c36ff0d6a75a322ab9225-150x150.png)





![Developmental toxicity of ribavirin/IF[alpha] combination therapy](http://s1.studyres.com/store/data/007999528_1-cb7557bb0c27e4b8c7666234733cbfd9-150x150.png)