Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
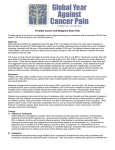
eau-ebu update series 5 (2007) 113–125 available at www.sciencedirect.com journal homepage: www.europeanurology.com Radionuclide Treatment in Metastasized Prostate Cancer Henk G. van der Poel * Department of Urology, Netherlands Cancer Institute, Plesmanlaan 121, 1066 CX Amsterdam, The Netherlands Article info Abstract Keywords: Prostate cancer Bone metastases Radionuclide treatment Painful osseous metastases are the major cause of cancer-related pain in metastasized prostate cancer. In hormone refractory prostate cancer multiple painful metastases can be treated with radionuclides. Initially, Strontium-89 was successfully used for pain palliation with pain relief in more than half the patients. More recently, radionuclides with shorter physical half-lives such as Rhenium and Samarium were shown to result in similar pain reduction rates, possibly lower myelosuppression incidences, and at least earlier recovery of hematological parameters allowing repetitive dosing. The low number of randomized trials on radionuclides in prostate cancer does prohibit proper selection based on efficacy and toxicity. Hence application is often dependent on local availability of the different radionuclides. # 2007 European Association of Urology and European Board of Urology. Published by Elsevier B.V. All rights reserved. * Tel. +31205122553; Fax: +31205122554. E-mail address: [email protected]. 1. Introduction The majority of patients with metastasized prostate cancer experiences painful osseous metastases during the course of the disease [1]. Androgen ablation results in pain reduction in most patients with painful metastases. In hormone refractory prostate cancer (HRPC) painful osseous metastases is one of the most prevalent clinical problems [2]. Local radiotherapy, chemotherapy, and bisphosphonates were shown to provide some pain relief [1]. Bone seeking intravenous radionuclide treatment is an effective other modality in these patients. Radionuclide treatment was initially introduced in 1942 using Strontium-89 (Sr89) [3]. Reported pain response rates to radionuclides vary widely from 36% to 92% [4–7] probably depending on assessment method and population characteristics. Oosterhof et al. (2003) [7] showed that patients with a smaller decrease in hemoglobin concentration after radionuclide treatment had a better pain response. Others found better responses in patients with less extensive osseous involvement [4,8–10]. Whether the relatively long half-life of 50.5 days for Sr89 and toxicity of bone marrow suppression account for the reported reduction in survival when compared to external beam radiotherapy [7] is unknown but it may favor the use of radionuclides with shorter half-lives such as Rhenium-186 (Re186, half-life 3.8 days), Re188 (17 hours), and Samarium153 (Sm153, 2 days) [11]. Although Re186 was shown to be superior to placebo in a randomized trial [12], only minimal differences with respect to efficacy and toxicity of Re186 versus Sr89 was shown and most non-randomized studies in breast and prostate 1871-2592/$ – see front matter # 2007 European Association of Urology and European Board of Urology. doi:10.1016/j.eeus.2007.02.002 Published by Elsevier B.V. All rights reserved. 114 eau-ebu update series 5 (2007) 113–125 cancer suggest similar efficacy for Sr89 and Re186 [5,8,13]. Whereas toxicity may be reduced in patients treated with radionuclides with a shorter half-life, such as Re186, and recovery from myelosuppression may be shorter, Sr89 seems to provide somewhat longer duration of efficacy. Sporadically, 117mSn (low-energy conversion electrons) and 223Ra (alphaemitter) are used in bone metastases but experience in prostate cancer management is limited [14,15]. The percentage of prostate cancer patients presenting with osseous metastases at initial diagnosis decreased significantly over recent years. Moreover, due to earlier diagnosis, many patients have HRPC even before the clinical manifestation of osseous metastases. This often implies that chemotherapeutic agents will be applied earlier in disease, in some cases even in the absence of metastasized disease. Although bisphosphonates seem to delay skeletal related invents in the long run, they are less effective in management of acute osseous pain. For these reasons, radionuclide treatment may be value in patients with osseous metastases from hormone and chemotherapy refractory prostate cancer in later phases of disease. Here the most widely used radionuclides for treatment of painful osseous metastases from prostate cancer are reviewed. Strontium-89 (Sr89) [18,19]. Both substances have a natural tendency to bind to bone. Over 80% of the total body phosphate is present in bone, bound as inorganic phosphate to hydroxyapatite. Radiophosphorus, administered intravenously as P32-sodium orthophosphate for skeletal targeting, was used extensively in the 1970s to treat metastatic hormone refractory prostate cancer (HRPC) [20]. More recent data suggest equal efficacy after oral administration [21]. The main disadvantage of P32 therapy is dose-limiting myelosuppression with reversible pancytopenia with nadir values at 5–6 weeks after administration. In comparison to Sr89 the higher myelotoxicity of P32 rendered Sr89 the radionuclide of choice for painful osseous metastases [22]. P32 is nowadays rarely used in the US or Europe but its relatively low costs and oral availability make it a potential alternative to Sr89. Compared with hemi-body radiation the use of radionuclides such as Sr89 provide pain relief from multiple bone lesions with less toxicity like bowel and pulmonary complaints often observed after hemi-body radiotherapy. More recently used radionuclides such as Rhenium-186, Rhenium-188, and Samarium-153 all lack the natural tendency to bind bone. Hence, chelation with a bisphosphonate is required to target these radionuclides to areas of osteoclastic/osteoblastic activity (Table 1). 2. History of radionuclide treatment for osseous metastases 3. Early studies using radionuclides for painful osseous metastases comprise Phosphor-32 (P32) [16,17], and Strontium is named after the UK-village it was first discovered in in 1790. Strontium is close to calcium Strontium-89 (Sr89) Table 1 – Studies comparing pain response between different radionuclides Radionuclides N Tumor Study design Sr89 vs Sm153 N = 57 Prostate Sr89 vs 32P N = 31 Various tumors Non-randomized, retrospective Non-randomized Sr89 vs Re186 vs Re188 Sr89 vs Re186 N = 44 Various tumors Non-randomized N = 50 Breast Randomized Sm153 vs Re186 N = 29 (prostate, N = 22) N = 46 Various tumors Non-randomized Breast, Prostate Non-randomized N = 60 Prostate Non-randomized, retrospective (selection on metastases extent) Sm153-EDTMP vs Re188-HEDP Re186 vs Sr89 Result No difference in pain response rate and toxicity No difference in pain response rate and response duration. Higher drop in platelet count for P32 but not clinical relevance No difference in pain response or toxicity. Re188 best improvement in QoL Earlier pain response in Re186, similar duration of response, earlier recovery from hematological toxicity in Re186 (6w versus 12w) Bone uptake and soft-tissue clearance higher for Sm153 No differences in pain response, Karnofsky performance score, and bone marrow toxicity No difference in response rate or toxicity Ref. [49] [21] [13] [5] [91] [11] [35] eau-ebu update series 5 (2007) 113–125 in the periodic table of elements and has the same metabolic handling. Strontium-89 has a natural affinity for metabolically active bone. The cause of the higher affinity of Sr89 is debated. Since Sr89 is close to calcium in the periodic table and bone metabolism and turn-over is higher in osseous metastases from prostate cancer it can be postulated that more readily uptake of calcium and Sr89 in these areas accounts for the higher affinity observed. Strontium-89 is a beta-emitter with a physical half-life of 50.5 days. The partical range in tissue is approximately 7 mm. Sr89 was shown to have a higher affinity for tumor containing bone than normal bone [23] and half-life in normal bone (14 days) is considerably shorter than in tumor containing bone (50 days). Excretion is renal and thus glomerular filtration rate should be considered prior to administration. A double-blind randomized trial showed higher efficacy for Sr89 compared to the Sr86 and Sr88 radionuclides [24]. The role of dosing Sr89 is less clear. Dose-finding studies did not find an association between pain relief and dose [19,25]. Retrospective analyses, however, suggested that higher doses of Sr89 resulted in improved pain relief [26]. In general, 130–200 MBq is used to treat osseous metastases in prostate cancer. 3.1. Sr89 and pain response A placebo-controlled randomized study using the low dose of 75 MBq i.v. Sr89 could not confirm an improvement in pain response superior to placebo [27] whereas a higher dose of Sr89 (150 MBq) was associated with a risk reduction of pain relief of 0.32 [24]. Initial studies using intravenous Sr89 showed efficacy for pain relief as high as 80%. Complete pain response rates vary widely among studies and have been reported in 8–77% of cases whereas a reduction in pain was reported by 18–50% of patients treated with Sr89 for an overall response rate varying from 33 to 82% [24,25,28–34]. A pain flare occurs in 15% of patients within one week after infusion [26]. The duration of response varies between 14 days and up to 15 months with a median of around 60 days [7,35,36]. The problematic assessment of pain response and documentation of analgetics use hamper comparison between studies and probably explains the wide variation in reported pain responses. Although Sr89 is assumed to exert pain relief through a reduction in growth of bone metastases, serological PSA and alkaline phosphatase responses have only been observed in a minority of patients [35,36]. In 37% of patients Turner et al. [37] observed a more than 50% reduction in serum PSA whereas 115 Oosterhof et al. (2003) [7] found biochemical responses in 13% of patients. Others, however, did not observe a noticeable response when Sr89 was applied to treat painful osseous metastases in HRPC [35,38]. An important medical condition in patients with HRPC is the development of acute spinal cord compression (SCC) resulting in lower body paralysis. Signs of SCC are a contraindication for radionuclide treatment. The possible flare up after radionuclide treatment and the higher efficacy of local treatment such as external radiotherapy and surgery make latter 2 options first choice. In a retrospective analysis Soerdjbalie et al. (2002) [39] found a reduced incidence of SCC during follow-up in patients treated with Sr89 but not in patients treated with the biphosphonate olpadronate. 3.2. Sr89 toxicity The most frequently observed toxicities are associated with the bone marrow suppression associated with Sr89 use: a reduction in white-blood cell count and thrombocyte count between 11–65% in more than half the patients. Blood cell counts do return to normal within 8 weeks and rarely cause grade 3 or 4 toxicity when Sr89 is applied to patients with normal hematological parameters. The influence of Sr89 on serum hemoglobin concentration seems to be limited and did not exceed the reduction in serum hemoglobin observed in patients treated with external beam radiotherapy [7]. No difference in hematological toxicity between external beam radiotherapy and Sr89 was observed in a randomized trial [7]. The reduced survival of patients treated with Sr89 compared with external beam radiotherapy observed in this recent EORTC trial remained unexplained but placebo controlled randomized studies with Sr89 could not confirm an unfavorable effect of Sr89 on overall survival [24,27]. Similarly, other radionuclides were not associated with decreased survival [24,27,40]. 3.3. Sr89 response prediction Several patient characteristics could predict a favorable response to Sr89. A normal serum hemoglobin prior to treatment is associated with a higher pain response rate [10,35]. Oosterhof et al. (2003) [7] found that patients who had a response to treatment showed a lesser decrease in median hemoglobin level after 4 and 8 weeks than those who did not respond to treatment. This finding applied to both radionuclide and external beam radiotherapy. Beer et al. (2004) found an association between 116 eau-ebu update series 5 (2007) 113–125 anemia, response to androgen ablation and survival in patients with metastasized prostate cancer even after correcting for extent of disease [41]. They suggested that anemia may lead to increased intratumoral hypoxia rendering tumor cells more resistant to therapeutic interventions such as radiation [42]. Moreover, possible etiological factors of anemia such as cytokines (IL6, IL8) are often elevated in prostate cancer patients [43] and may play a role in response to pain stimuli in these patients as well [44]. Hence, the factors leading to anemia may increase pain perception and decrease sensitivity to radiation through hypoxia thus resulting in a decreased pain response. Other predictors of a poor pain response were low performance status, higher serum PSA, more extensive osseous metastases [7,8], and poor PSA response [45]. These findings make clear that efficacy of Sr89 increases when applied in earlier phases of disease where the patient has a better performance, and less extensive disease and pain. Repeated doses of Sr89 were shown to result in similar pain response rates when compared to initial treatment efficacy rates [9,28,35]. Due to myelotoxicity it is generally advisable to repeat dosing at intervals of at least 6 weeks. 3.4. Comparison of Sr89 and external beam radiotherapy External beam radiotherapy is an effective means of treating pain of osseous metastases in prostate cancer. Several studies compared the efficacy of external beam radiotherapy and Sr89. Oosterhof et al. (2003) [7] compared Sr89 (150 MBq) and local field external beam radiotherapy in a randomized fashion. Patients treated with Sr89 showed a 34.7% pain response rate whereas external beam radiotherapy resulted in pain reduction in 33.3% of patients. One third of the study population had only one painful metastatic site. The authors concluded that the higher costs associated with radionuclide treatment favor external beam radiotherapy. In comparison to hemi-body radiotherapy Sr89 treatment showed similar response rates with fewer new active sites during follow up suggesting that a preventive effect was present after Sr89 treatment [46,47]. Adjuvant high-dose Sr89 (400 MBq) to external beam radiotherapy did result in a reduced number of new sites but not in less pain in the initial painful site [48]. This additive effect to external beam radiotherapy, however, was not confirmed for the normal Sr89 dose (150 MBq) [40]. Data suggests that a combination of external beam radiotherapy and Sr89 was of limited value for pain control (Table 2). 3.5. Comparison of Sr89 with other radionuclides and chemotherapy Comparison of Sr89 in osteoblastic metastases with other radionuclides such as 32P [21], Rhenium-186 [5,13,35], and Samarium153 [49] showed comparable efficacy for pain control. Most studies, however, were non-randomized. In one randomized study of patients with osseous metastasized breast cancer the hematological parameters returned quicker to baseline after treatment with Re186 compared to Sr89 [5]. Hence, radionuclides based on Samarium and Rhenium with shorter half-lives compared to Sr89 may be preferable over Sr89 especially when repetitive or chemotherapy-combined approaches are considered. In a recent report Nilsson et al. (2005) [50] used a double-blind randomized study-design to compare the palliative efficacy of a combination chemotherapy protocol (FEM, 5-FU, epirubicin, mitomycin-C) and Sr89. Both arms in the study showed comparable reduction in pain score during the entire 12 weeks of the study. Treatment related toxicity, however, was higher in the FEM arm where the number of hospitalizations due to treatment toxicity was twice as high as in the Sr89 arm. 4. Rhenium-186 (Re186) Rhenium is a group VII metal. Irradiation of enriched Rhenium-185 produces the radionuclide Rhenium186 (Re186). Re186 decays with the emission of a beta particle (Emax 1.07 Mev) and (9%) gamma ray Table 2 – Comparison of radionuclides and external beam radiotherapy (EBRT = external beam radiotherapy, Sr89 = Strontium-89) n Dearnaley et al. (1992) [47] Quitly et al. (1994) [46] Oosterhof et al. (2003) [7] 78 284 203 Study design matched control randomized randomized Radiotherapy hemibody hemibody/local local Pain reduction Median survival EBRT vs Sr89 EBRT vs Sr89 63% vs 52% 64% vs 66% 33% vs 35% 20w vs 21w 28w vs 33w 11m vs 7.2m eau-ebu update series 5 (2007) 113–125 (137 keV) which renders it suitable for imaging (Fig. 1) with a physical half-life of 3.8 days. Re-186 bound with the bisphosphonate hydroxyethylidene diphosphonate (HEDP) was first described for treatment of painful bone metastases in the late 1970’s [51,52]. The complexed Re186 binds to hydroxyapatite crystals by forming hydroxide bridges in a hydrolysis reaction. Re186-HEDP is cleared from the plasma with a half-life of 41 hours and the majority is secreted within 24 hours with the urine. It has been used for the palliation of bone pain in several studies with response rates ranging from 30 to 80% with mean duration of response of 7–9 weeks [53,54]. In a rat animal model, Re186-HEDP delayed clinical symptoms from vertebral metastases such a leg paralysis and urinary retention in the bladder [55]. The maximum tolerated dose for Re186-HEDP is 2960 MBq [56,57] and no dose response was noted in the dose range of 1295–2960 MBq [58]. Typically, pain response occurs 1–3 weeks after infusion with a duration of 5–12 months. After approximately one week a pain flare does occur in up to 50% of patients. Toxicity has been shown to consist of thrombocytopenia whereas leucopenia seems to play a minor role [59]. Grade 2 and 3 thrombocytopenia occurs in 117 12% and 7% respectively but rarely is clinically relevant. The same applies for neutropenia that is seen in 29% of cases but rarely results in clinical interventions. In a randomized trial the Re186-HEDP was shown to be superior over placebo: 27% of patients reported pain relief compared to still 13% in the placebo group [12]. Twenty of 131 men did not receive Re186-HEDP due to rapid progression suggesting that the population in this study was in a poor condition. Since a low serum hemoglobin and poor performance were shown to be associated with poor pain response [7,35] this may explain the relatively low response rate compared to the 50% of pain responses reported in other analyses [35,60]. At higher doses the use of Re186-HEDP is limited by its myelosuppressive toxicity. Re186-HEDP at higher doses (up to 5000 MBq) with autologous blood stem cell rescue and re-infusion 2 weeks after Re186 injection was shown to result in a partial PSA response in 20% of cases that received more than 3500 MBq [61]. No grade IV thrombocytopenia or leucopenia was reported. These initial findings resulted in a phase-II trial of 38 patients treated with high dose Re186-HEDP (dose range 4770– 5100 MBq). In this second study 21% of patients Fig. 1 – Comparison of Technetium-99 (Tc-99M) and Rhenium-186 (Re186) bone scan. Gamma-emitting radionuclides such as Rhenium and Samarium can be used for imaging to confirm corrrect uptake of the therapeutic radionuclide to the areas of bone activity found on the Technetium bone scan. 118 eau-ebu update series 5 (2007) 113–125 experienced grade 3 thrombocytopenia with a nadir platelet count value after 3 weeks. In 29% of cases a PSA decrease of at least 50% was observed that lasted for more than 4 weeks. The median duration of PSA response was 5.6 months. Re186-HEDP results in considerable pain relief and mild toxicity at lower doses. At high dose, Re186-HEDP resulted in a modest PSA response, but significantly more bone marrow suppression. 5. Rhenium-188 (Re188) Another radionuclide derived from Rhenium is Re188. Compared to Re186 it has a shorter half-life (12 hours for the entire body and 16 hours in bone metastases) [62]. In a dose-escalation analysis the maximal tolerated dose was determined on 3.3 GBq [63]. Pain palliation is reported in 66–77% of patients with a complete response percentage of 16–25% [6,11,64]. Moreover, an improvement in quality of life-score was noted in the 6–12 week period following Re188-HEDP infusion [6]. Similar to Re186-HEDP, Re188 complexed to HEDP resulted in hematological toxicity with a reduction in platelet count in 20% of cases and a reduction in leucocyte count in 25% of cases. These parameters return to normal within 3 months and proper patient selection rarely results in serious toxicity [6,62,65,66]. An alternative to Re188-HEDP is Re188 chelated to dimercaptisuccinic acid (Re188-DMSA). Re188DMSA was shown to target bone metastases from prostate cancer specifically but clinical experience is limited to one report [67]. Palmedo et al. (2003) [68] studied the effects of repetitive Re188-HEDP injections for pain palliation in osseous metastases from prostate cancer. In a randomized fashion patients were assigned to either a single Re188-HEDP injection or 2 injections with an 8 week interval. Repetitive dosing not only improved pain response but also resulted in a higher percentage of PSA responses (39% versus 7%) and significantly improved median overall survival from 7 months in the single dose group to 12.7 months in the repetitive dosing group. Maximal toxicity in both groups was transient grade-2 thrombocytopenia and leukopenia. A non-randomized comparison of Re188-HEDP and Sm153-EDTMP in patients with painful metastases from prostate and breast cancer Liepe et al. [11] showed comparable response and toxicity for both agents. Re188-HEDP was shown equally effective and toxic to Sm153-EDTMP in non-randomized analyses and repetitive dosing is feasible. 6. Samarium-153 (Sm153) Bombardment of enriched Samarium-152 with neutrons in a nuclear reactor results in samarium153 (Sm153). Sm153 has no natural affinity for bone but can be complexed with several aminocarboxylates and aminophosphonates such as ethylenediamine-tetramethylenephosphonate (EDTMP) directing osseous targeting. Clearance from the bloodstream is completed 6 hours after injection and excretion is done in the urine [69] whereas nuclear decay half-life is 1.9 days with 0.22 MeV beta-emission and 103 keV gamma rays. Hence, similar to Rhenium-based radionuclides Sm153EDTMP can be used for imaging. Bone metastases bind 5 more Sm153 compared to normal bone [70]. Dose limiting toxicity consists of thrombocytopenia and is seen in 20–42% of patients. In more than 95% of patients platelet count normalizes within 5 weeks [70–73]. Pain relief from osseous metastases after Sm153-EDTMP occurs in 30–85% of patients in a variety of tumors [74]. Several randomized, double-blind studies have analyzed the efficacy of Sm153-EDTMP. A higher dose (37 MBq/kg) was shown to be more effective for palliation of pain from osseous metastases in both breast and prostate cancer compared to a lower dose (18.5 MBq/kg) [75]. In breast cancer patients, but not in prostate cancer patients, the highest dose of Sm153-EDTMP was associated with improved survival. Another three-arm randomized trial comparing low dose (18.5 MBq/kg) and high dose Sm153-EDTMP (37 MBq/kg), versus placebo reported an improvement in pain for both low dose (42%) and high dose (67%) Sm153-EDTMP after 4 weeks [76]. A more recent randomized phase-III trial compared Sm153-EDTMP to placebo [77]. Analgetics use decreased significantly after a 2–4 week interval. Moreover, 9% of patients in the Sm153-EDTMP group showed a reduction of more than 50% in serum PSA levels. In all three trials only mild thrombocytopenia and neutropenia were reported with platelet count reduction between 43–55% and white-blood cell count reduction between 45–60% at 3–4 weeks after infusion. Normalization of hematological parameters was reported in all trials by 8 weeks. Sm153 in repetitive dosing was shown to be effective [70]. Repetitive dose was studied in 15 patients of which 13 (87%) showed pain improvement after secondary treatment. Both the median duration of pain control (24 versus 8 weeks) and survival (9 versus 4 months) in the retreated group were substantially greater than for patients treated 119 eau-ebu update series 5 (2007) 113–125 for example cisplatin and docetaxel are known and exploited to increase efficacy of external beam radiotherapy [78,79]. On the other hand, both radionuclide and chemotherapy result in myelotoxicity and, therefore, hematological toxicity may increase with the combination therapy. In the 2005 EAU-guidelines for prostate cancer [80] the authors mention (section 16.10) that palliative treatment with Samarium and Strontium radionuclides may be effective but could compromise later chemotherapy due to myelotoxicity of both treatments. Recent data, however, suggests that radionuclide treatment does not prohibit further chemotherapy and that the effects on bone marrow function is limited to the first 6 to 12 months after administration [81]. with a single dose. However, 60% of the patients in the re-treatment group required blood transfusions for anemia. This increased efficacy of repeat dosing was not observed in other studies [35]. Selection of patients may have caused this inconsistency. Repetitive dosing of Sm153 is feasible. When treatment intervals exceed 6 weeks toxicity is limited and reversible. 7. Comparing radionuclides for efficacy Based on effects of myelosuppression it can be expected that radionuclides with shorter half-life would potentially be less toxic. The local availability and approval of use by regulatory bodies of radionuclides with shorter half-lives dictate the use in different countries. So far, based on clinical efficacy and toxicity data, none of these radionuclides has shown convincing superiority of the others neither with respect to efficacy nor with respect to toxicity. Based on limited comparison analyses the shorter half - life of Re188 compared to Re186 and Sm153 may favor its use in the light of toxicity. The need for a production facility close by the hospital with the use of short half-life radionuclides such as Re188 may prohibit the extensive use of the agents (Table 3). 8. Combination therapy 8.1. Radionuclides and chemotherapy 8.2. Chemotherapy and Sr89 Sr89 was shown to be of benefit to patients that earlier received and were resistant to chemotherapy [36]. Conversely, Sr89 treatment did not prohibit future chemotherapy application [81]. Akerley et al. (2002) [82] showed that Sr89 (2.2 MBq/kg) in combination with estramustine (600 mg/m2) and vinblastine (4 mg/m2) resulted in a PSA decline of more than 50% for longer than 6 weeks in 48% of patients. Pain response was not assessed in this non-randomizedstudy. Pain response was improved upon the addition of low-dose cisplatin (18 mg/m2) to Sr89 (148 MBq) [83,84]. Any reduction in pain was experienced by 91% of patients in the combination arm against 63% in the Sr89 monotherapy arm. However, the rate of ‘‘complete’’ response was not significantly different for both arms. Interestingly, none of the hematological toxicity parameters was significantly different for both arms. No significant difference in overall Based on several findings there is reason to believe that a combination of radionuclides and and chemotherapeutic agents may have synergistic antitumor activity. The radiosensitizing effects of Table 3 – Available radionuclides for bone metastases targeting Radionuclide Bisphosphonate T Response time Response duration Energy (MeV) Particle type 32P 89Sr 153Sm-EDTMP Phosphor Strontium Samarium 14.3 d 50.5 d 46.3 hrs 14d 21d 7d 10w 20w 8w 1.71 1.46 0.80 beta beta beta/gamma 186Re-HED Rhenium 89 hrs 7d 8w 1.07 beta/gamma 188Re-HEDP Rhenium 17 hrs 7d 8w 2.12 beta/gamma 117mSn-DTPA Tin 13.6 d 14d 4w 0.13-gamma gamma-photon 223Ra Radium – – Ethelenediaminetetramethylane phosphoracid Hydroxy ethylidene difosfonaat (etidronate) Hydroxy ethylidene difosfonaat (etidronate) Diethylene triamine pentaacetic acid – 11.4 d – – 28-alpha alpa/gamma 120 eau-ebu update series 5 (2007) 113–125 survival between Sr89 and S89+cisplatin was observed. The combination of Sr89 and doxorubicin after two or three courses of induction doxorubicin was found to prolong survival in a small randomized trial. The addition of doxorubicin to Sr89 extended median survival from 16.8 months in the doxorubicin only group to 27.7 months in the combined treatment group [85]. These data suggest that a combination of Sr89 and chemotherapeutic agents may potentially improve survival in a subgroup of patients and has mild toxicity. The limited data available prohibit widespread use of the combination, in particular with respect to the effects on bone marrow suppression. 8.3. Chemotherapy and Sm153-EDTMP The ongoing TAXSAM study is a non-randomized phase II analysis to evaluate the tolerability and efficacy of a combination of Sm153-EDTMP and docetaxel in patients with hormone refractory prostate cancer. Docetaxel was administered at a dose of 30 mg/m2 weekly for 5 weeks. Eighteen to twenty-four hours prior to the fourth administration of docetaxel, the approved dose of Sm153-EDTMP (1 mCi/kg) was injected. Patients received a second cycle of the TAXSAM combination regimen at PSA and/or clinical progression. Grade 3 and 4 neutropenia was observed in 3 of 29 patients between 2–6 weeks after Sm153-EDTMP infusion. Thrombocytopenia higher than grade 2 did not occur. Within 12 weeks 34% and 18% of patients had a more than 50% reduction in serum PSA after the first and second Sm153-EDTMP, respectively [86]. Higher PSA response rates were reported by Fizazi et al. [87] combining Sm153-EDTMP with docetaxel after a positive response to 4 courses of 70 mg/m2 docetaxel and estramustine 3-weekly. Twenty-five of 36 (69%) of patients had a PSA decrease of more than 50% and 80% of patients reported a decrease in VAS-score pain assessment by more than 2 points after the initial 4 docetaxel induction cycles. Patients that experienced a positive response after the initial 4 cycles of docetaxel were treated with a maintenance protocol with a single Sm153-EDTMP infusion combined with weekly docetaxel 20 mg/m2 for 6 weeks. For the patients that completed 6 weeks maintenance treatment the pain response was 94%. These data suggest that a single Sm153-EDTMP treatment increases the incidence of grade 3–4 neutropenia of weekly docetaxel: 5% grade 3–4 neutropenia in docetaxel [88] compared to 10% in the combination. Thrombocytopenia was not more frequent in the combined treatment, whereas PSA response and pain response were higher. Data from ongoing randomized studies is needed here to evaluate both pain response and survival of the combination of chemotherapy and Sm153-EDTMP treatment but initial findings seem promising. 8.4. Bisphosphonates and radionuclide treatment Bisphosphonate treatment was shown to result in a modest reduction in pain from osseous metastases in prostate cancer but pain relief occurred after considerable longer intervals compared to radionuclide treatment [89]. Since bisphosphonates are used to target Re186, Re188, and Sm153 to bone metastases it was studied whether earlier treatment with bisphosphonates may influence efficacy of these radionuclides. Recently, a non-randomized comparison in a small group of patients found that the combination of zoledronic acid and Sr89 was more effective for pain relief than either of the two agents in monotherapy [90]. These limited findings suggest that bisphosphonates not necessarily counteract the efficacy of radionuclide treatment and patients experiencing pain while on bisphosphonates could continue these while receiving radionuclide treatment. 9. Recommendations for radionuclide use Data from both retrospective and prospective studies do indicate that pain palliation obtained by radionuclide treatment is most likely in patients with relatively good performance status and pain reduction can be obtained in over 50% of patients which seems higher than for chemotherapy. Pretreatment a bone scan be done to confirm metastases and exclude patients with a so-called super-scan, since it is generally assumed that bone marrow toxicity may be higher in these patients. Hematological parameters showed be assessed and be higher than lower normal limits. It is recommended to use radionuclides only in patients with renal clearance over 60 ml/min. As for chemotherapy, the likely of pain relief decreases when serum hemoglobin starts to drop, this reflecting a poor overall condition. Radionuclides with shorter physical half-lives, such as Sm153, Re186 and Re188, that, based on the earlier recovery of bone marrow toxicity compared to initially used radionuclides (Sr89) could potentially be given at higher frequency which favors repetitive use and supports treatment earlier in the course of disease. Moreover, data now clearly show that radionuclide treatment not necessarily precludes further chemotherapy. eau-ebu update series 5 (2007) 113–125 Considering the milder side-effect profile for radionuclides compared to chemotherapy it should be considered first choice in patients with multiple painful osseous metastases where external beam radiotherapy is not feasible due to the number of metastases. Moreover, radionuclide treatment should be considered in patients with painful metastases after chemotherapy. Combination of radionuclide treatment and chemotherapy should be considered experimental. Although increased efficacy was has been observed for the combination, the incidence of grade 3 and 4 neutropenia also increased. A combination of bisphosphonates with radionuclides was not associated with increased toxicity and potentially increases efficacy of pain relief. 121 - Bone marrow suppression with thrombocytopenia and neutropenia occurs in similar frequency and grade in all radionuclides but a shorter half-life seems to be associated with earlier recovery to baseline blood cell counts. - Repetitive dosing of all radionuclides was shown to be feasible when the intervals were at least 6 weeks. - Combination of radionuclides with external beam radiotherapy and chemotherapy was shown to be beneficial, but toxicity increased significantly. - Combination of radionuclides with chemotherapeutic agents should be considered an experimental treatment and study data are awaited. References 10. Future Combination of chemotherapy and radionuclide treatment and a direct comparison of both modalities should be studied. The initial findings of a combination of Samarium based radionuclides and docetaxel hold promise. Alpha-particle emitters deliver a higher energetic and localized radiation with a much smaller range in tissue than betaparticles. These alpha-particle radiation induces predominantly non-reparable DNA double-strand breaks which may kill dormant cells but alphaemitters are potentially more toxic and mutagenic than beta-emitters. Further evaluation of alphaemitters such as Ra223 that has a natural affinity for bone like Sr89 is awaited but initial data suggests reduced thrombocytopenia in patients with prostate cancer [14,15]. 11. Remarks - Pain response is seen in approximately half the patients treated with radionuclides for painful osseous metastases of prostate cancer. - P32 and Sr89 show a natural affinity for bone, whereas Re186, Re188, and Sm153 require chelation to bisphosphonates for targeting. - Of the different radionuclides used those with a shorter half-life such as Re186-HEDP, Re188-HEDP, and Sm153-EDTMP showed similar efficacy compared to Sr89, with a longer half-life. - Several parameters are associated with a favorable pain response: higher performance score and lower pain score at treatment, higher serum hemoglobin, and a limited number of osseous metastases. [1] Morris MJ, Scher HI. Clinical approaches to osseous metastases in prostate cancer. Oncologist 2003;8:161–73. [2] Smith Jr JA, Soloway MS, Young MJ. Complications of advanced prostate cancer. Urology 1999;54:8–14. [3] Pecher C. Biological investigation with radioactive calcium and strontium: preliminary report on the use of radioactive strontium in the treatment of metastatic bone cancer. Univ Calif Publ Pharmacol 1942;2:117–49. [4] Kolesnikov-Gauthier H, Carpentier P, Depreux P, Vennin P, Caty A, Sulman C. Evaluation of toxicity and efficacy of 186Re-hydroxyethylidene diphosphonate in patients with painful bone metastases of prostate or breast cancer. J Nucl Med 2000;41:1689–94. [5] Sciuto R, Festa A, Pasqualoni R, Semprebene A, Rea S, Bergomi S, et al. Metastatic bone pain palliation with 89-Sr and 186-Re-HEDP in breast cancer patients. Breast Cancer Res Treat 2001;66:101–9. [6] Liepe K, Kropp J, Runge R, Kotzerke J. Therapeutic efficiency of rhenium-188-HEDP in human prostate cancer skeletal metastases. Br J Cancer 2003;89:625–9. [7] Oosterhof GO, Roberts JT, de Reijke TM, Engelholm SA, Horenblas S, von der Maase H, et al. Strontium(89) chloride versus palliative local field radiotherapy in patients with hormonal escaped prostate cancer: a phase III study of the European Organisation for Research and Treatment of Cancer Genitourinary Group. Eur Urol 2003;44:519–26. [8] Dafermou A, Colamussi P, Giganti M, Cittanti C, Bestagno M, Piffanelli A. A multicentre observational study of radionuclide therapy in patients with painful bone metastases of prostate cancer. Eur J Nucl Med 2001;28:788–98. [9] Kraeber-Bodere F, Campion L, Rousseau C, Bourdin S, Chatal JF, Resche I. Treatment of bone metastases of prostate cancer with strontium-89 chloride: efficacy in relation to the degree of bone involvement. Eur J Nucl Med 2000;27:1487–93. [10] Windsor PM. Predictors of response to strontium-89 (Metastron) in skeletal metastases from prostate cancer: report of a single centre’s 10-year experience. Clin Oncol (R Coll Radiol) 2001;13:219–27. 122 eau-ebu update series 5 (2007) 113–125 [11] Liepe K, Runge R, Kotzerke J. The benefit of bone-seeking radiopharmaceuticals in the treatment of metastatic bone pain. J Cancer Res Clin Oncol 2005;131:60–6. [12] Han SH, de Klerk JM, Tan S, het Schip AD, Derksen BH, van Dijk A, et al. The PLACORHEN study: a double-blind, placebo-controlled, randomized radionuclide study with (186)Re-etidronate in hormone-resistant prostate cancer patients with painful bone metastases. Placebo Controlled Rhenium Study. J Nucl Med 2002;43:1150–6. [13] Liepe K, Franke WG, Kropp J, Koch R, Runge R, Hliscs R. Comparison of rhenium-188, rhenium-186-HEDP and strontium-89 in palliation of painful bone metastases. Nuklearmedizin 2000;39:146–51. [14] Bruland OS, Nilsson S, Fisher DR, Larsen RH. High-linear energy transfer irradiation targeted to skeletal metastases by the alpha-emitter 223Ra: adjuvant or alternative to conventional modalities? Clin Cancer Res 2006;12: 6250s–7s. [15] Nilsson S, Larsen RH, Fossa SD, Balteskard L, Borch KW, Westlin JE, et al. First clinical experience with alphaemitting radium-223 in the treatment of skeletal metastases. Clin Cancer Res 2005;11:4451–9. [16] Glaser MG, Howard N, Waterfall N. Carcinoma of the prostate: the treatment of bone metastases by radiophosphorus. Clin Radiol 1981;32:695–7. [17] Taymor ML, McArthur JW, Ingersoll FM. The effect of interstitial cell stimulating hormone upon the uptake of P32 in the rat prostate. Surg Forum 1953;317–21. [18] Schmidt CG, Firusian N. 89-Sr for the treatment of incurable pain in patient with neoplastic osseous infiltrations. Int J Clin Pharmacol 1974;7:199–205. [19] Silberstein EB, Williams C. Strontium-89 therapy for the pain of osseous metastases. J Nucl Med 1985;26:345–8. [20] Potsaid MS, Irwin Jr RJ, Castronovo FP, Prout Jr GR, Harvey WJ, Francis MD, et al. [32P] diphosphonate dose determination in patients with bone metastases from prostatic carcinoma. J Nucl Med 1978;19:98–104. [21] Nair N. Relative efficacy of 32P and 89Sr in palliation in skeletal metastases. J Nucl Med 1999;40:256–61. [22] Montebello JF, Hartson-Eaton M. The palliation of osseous metastasis with 32P or 89Sr compared with external beam and hemibody irradiation: a historical perspective. Cancer Invest 1989;7:139–60. [23] Blake GM, Zivanovic MA, Blaquiere RM, Fine DR, McEwan AJ, Ackery DM. Strontium-89 therapy: measurement of absorbed dose to skeletal metastases. J Nucl Med 1988; 29:549–57. [24] Lewington VJ, McEwan AJ, Ackery DM, Bayly RJ, Keeling DH, Macleod PM, et al. A prospective, randomised doubleblind crossover study to examine the efficacy of strontium-89 in pain palliation in patients with advanced prostate cancer metastatic to bone. Eur J Cancer 1991;27:954–8. [25] Laing AH, Ackery DM, Bayly RJ, Buchanan RB, Lewington VJ, McEwan AJ, et al. Strontium-89 chloride for pain palliation in prostatic skeletal malignancy. Br J Radiol 1991;64:816–22. [26] Mertens WC, Stitt L, Porter AT. Strontium 89 therapy and relief of pain in patients with prostatic carcinoma meta- [27] [28] [29] [30] [31] [32] [33] [34] [35] [36] [37] [38] [39] [40] static to bone: a dose response relationship? Am J Clin Oncol 1993;16:238–42. Buchali K, Correns HJ, Schuerer M, Schnorr D, Lips H, Sydow K. Results of a double blind study of 89-strontium therapy of skeletal metastases of prostatic carcinoma. Eur J Nucl Med 1988;14:349–51. Robinson RG, Preston DF, Schiefelbein M, Baxter KG. Strontium 89 therapy for the palliation of pain due to osseous metastases. JAMA 1995;274:420–4. Correns HJ, Mebel M, Buchali K, Schnorr D, Seidel C, Mitterlechner E. 89Strontium therapy of bone metastases of carcinoma of the prostatic gland. Eur J Nucl Med 1979; 4:33–5. Firusian N, Mellin P, Schmidt CG. Results of 89strontium therapy in patients with carcinoma of the prostate and incurable pain from bone metastases: a preliminary report. J Urol 1976;116:764–8. Robinson RG, Spicer JA, Preston DF, Wegst AV, Martin NL. Treatment of metastatic bone pain with strontium-89. Int J Rad Appl Instrum B 1987;14:219–22. Tennvall J, Darte L, Lundgren R, el Hassan AM. Palliation of multiple bone metastases from prostatic carcinoma with strontium-89. Acta Oncol 1988;27:365–9. McEwan AJ, Amyotte GA, McGowan DG, MacGillivray JA, Porter AT. A retrospective analysis of the cost effectiveness of treatment with Metastron in patients with prostate cancer metastatic to bone. Eur Urol 1994;26(Suppl 1):26–31. Mertens WC, Filipczak LA, Ben Josef E, Davis LP, Porter AT. Systemic bone-seeking radionuclides for palliation of painful osseous metastases: current concepts. CA Cancer J Clin 1998;48:361–74. van der Poel HG, Antonini N, Hoefnagel CA, Horenblas S, Valdes Olmos RA. Serum hemoglobin levels predict response to strontium-89 and rhenium-186-HEDP radionuclide treatment for painful osseous metastases in prostate cancer. Urol Int 2006;77:50–6. Gunawardana DH, Lichtenstein M, Better N, Rosenthal M. Results of strontium-89 therapy in patients with prostate cancer resistant to chemotherapy. Clin Nucl Med 2004; 29:81–5. Turner SL, Gruenewald S, Spry N, Gebski V. Less pain does equal better quality of life following strontium-89 therapy for metastatic prostate cancer. Br J Cancer 2001;84:297– 302. Fossa SD, Paus E, Lochoff M, Backe SM, Aas M. 89Strontium in bone metastases from hormone resistant prostate cancer: palliation effect and biochemical changes. Br J Cancer 1992;66:177–80. Soerdjbalie-Maikoe V, Pelger RC, Nijeholt GA, Arndt JW, Zwinderman AH, Papapoulos SE, et al. Strontium-89 (Metastron) and the bisphosphonate olpadronate reduce the incidence of spinal cord compression in patients with hormone-refractory prostate cancer metastatic to the skeleton. Eur J Nucl Med Mol Imaging 2002;29:494–8. Smeland S, Erikstein B, Aas M, Skovlund E, Hess SL, Fossa SD. Role of strontium-89 as adjuvant to palliative external beam radiotherapy is questionable: results of a doubleblind randomized study. Int J Radiat Oncol Biol Phys 2003;56:1397–404. eau-ebu update series 5 (2007) 113–125 [41] Beer TM, Tangen CM, Bland LB, Thompson IM, Crawford ED. Prognostic value if anemia in newly diagnosed metastatic prostate cancer: a multivariate analysis of southwest oncology group study 8894. J Urol 2004;172:2213–7. [42] Movsas B, Chapman JD, Hanlon AL, Horwitz EM, Greenberg RE, Stobbe C, et al. Hypoxic prostate/muscle pO2 ratio predicts for biochemical failure in patients with prostate cancer: preliminary findings. Urology 2002;60:634–9. [43] Bogdanos J, Karamanolakis D, Tenta R, Tsintavis A, Milathianakis C, Mitsiades C, et al. Endocrine/paracrine/ autocrine survival factor activity of bone microenvironment participates in the development of androgen ablation and chemotherapy refractoriness of prostate cancer metastasis in skeleton. Endocr Relat Cancer 2003;10:279– 89. [44] Lee BN, Dantzer R, Langley KE, Bennett GJ, Dougherty PM, Dunn AJ, et al. A cytokine-based neuroimmunologic mechanism of cancer-related symptoms. Neuroimmunomodulation 2004;11:279–92. [45] Zyskowski A, Lamb D, Morum P, Hamilton D, Johnson C. Strontium-89 treatment for prostate cancer bone metastases: does a prostate-specific antigen response predict for improved survival? Australas Radiol 2001;45:39–42. [46] Quilty PM, Kirk D, Bolger JJ, Dearnaley DP, Lewington VJ, Mason MD, et al. A comparison of the palliative effects of strontium-89 and external beam radiotherapy in metastatic prostate cancer. Radiother Oncol 1994;31:33–40. [47] Dearnaley DP, Bayly RJ, A’Hern RP, Gadd J, Zivanovic MM, Lewington VJ. Palliation of bone metastases in prostate cancer. Hemibody irradiation or strontium-89? Clin Oncol (R Coll Radiol) 1992;4:101–7. [48] Porter AT, McEwan AJ, Powe JE, Reid R, McGowan DG, Lukka H, et al. Results of a randomized phase-III trial to evaluate the efficacy of strontium-89 adjuvant to local field external beam irradiation in the management of endocrine resistant metastatic prostate cancer. Int J Radiat Oncol Biol Phys 1993;25:805–13. [49] Dickie GJ, Macfarlane D. Strontium and samarium therapy for bone metastases from prostate carcinoma. Australas Radiol 1999;43:476–9. [50] Nilsson S, Strang P, Ginman C, Zimmermann R, Edgren M, Nordstrom B, et al. Palliation of bone pain in prostate cancer using chemotherapy and strontium-89. A randomized phase II study. J Pain Symptom Manage 2005; 29:352–7. [51] Mathieu L, Chevalier P, Galy G, Berger M. Preparation of rhenium-186 labelled EHDP and its possible use in the treatment of osseous neoplasms. Int J Appl Radiat Isot 1979;30:725–7. [52] Deutsch E, Libson K, Vanderheyden JL, Ketring AR, Maxon HR. The chemistry of rhenium and technetium as related to the use of isotopes of these elements in therapeutic and diagnostic nuclear medicine. Int J Rad Appl Instrum B 1986;13:465–77. [53] Maxon III HR, Schroder LE, Thomas SR, Hertzberg VS, Deutsch EA, Scher HI, et al. Re-186(Sn) HEDP for treatment of painful osseous metastases: initial clinical experience in 20 patients with hormone-resistant prostate cancer. Radiology 1990;176:155–9. 123 [54] Maxon III HR, Schroder LE, Hertzberg VS, Thomas SR, Englaro EE, Samaratunga R, et al. Rhenium-186(Sn)HEDP for treatment of painful osseous metastases: results of a double-blind crossover comparison with placebo. J Nucl Med 1991;32:1877–81. [55] Geldof AA, van den Tillaar PL, Newling DW, Teule GJ. Radionuclide therapy for prostate cancer lumbar metastasis prolongs symptom-free survival in a rat model. Urology 1997;49:795–801. [56] de Klerk JM, Zonnenberg BA, het Schip AD, van Dijk A, Han SH, Quirijnen JM, et al. Dose escalation study of rhenium186 hydroxyethylidene diphosphonate in patients with metastatic prostate cancer. Eur J Nucl Med 1994;21:1114– 20. [57] de Klerk JM, het Schip AD, Zonnenberg BA, van Dijk A, Quirijnen JM, Blijham GH, et al. Phase 1 study of rhenium186-HEDP in patients with bone metastases originating from breast cancer. J Nucl Med 1996;37:244–9. [58] Han SH, Zonneberg BA, de Klerk JM, Quirijnen JM, het Schip AD, van Dijk A, et al. 186Re-etidronate in breast cancer patients with metastatic bone pain. J Nucl Med 1999;40:639–42. [59] de Klerk JM, het Schip AD, Zonnenberg BA, van Dijk A, Stokkel MP, Han SH, et al. Evaluation of thrombocytopenia in patients treated with rhenium-186-HEDP: guidelines for individual dosage recommendations. J Nucl Med 1994;35:1423–8. [60] Quirijnen JM, Han SH, Zonnenberg BA, de Klerk JM, het Schip AD, van Dijk A, et al. Efficacy of rhenium-186etidronate in prostate cancer patients with metastatic bone pain. J Nucl Med 1996;37:1511–5. [61] O’Sullivan JM, McCready VR, Flux G, Norman AR, Buffa FM, Chittenden S, et al. High activity Rhenium-186 HEDP with autologous peripheral blood stem cell rescue: a phase I study in progressive hormone refractory prostate cancer metastatic to bone. Br J Cancer 2002;86:1715–20. [62] Liepe K, Hliscs R, Kropp J, Runge R, Knapp Jr FF, Franke WG. Dosimetry of 188Re-hydroxyethylidene diphosphonate in human prostate cancer skeletal metastases. J Nucl Med 2003;44:953–60. [63] Palmedo H, Guhlke S, Bender H, Sartor J, Schoeneich G, Risse J, et al. Dose escalation study with rhenium-188 hydroxyethylidene diphosphonate in prostate cancer patients with osseous metastases. Eur J Nucl Med 2000;27:123–30. [64] Lambert B, de Klerk JM. Clinical applications of 188Relabelled radiopharmaceuticals for radionuclide therapy. Nucl Med Commun 2006;27:223–9. [65] Li S, Liu J, Zhang H, Tian M, Wang J, Zheng X. Rhenium-188 HEDP to treat painful bone metastases. Clin Nucl Med 2001;26:919–22. [66] Liepe K, Hliscs R, Kropp J, Gruning T, Runge R, Koch R, et al. Rhenium-188-HEDP in the palliative treatment of bone metastases. Cancer Biother Radiopharm 2000;15:261–5. [67] Blower PJ, Lam AS, O’Doherty MJ, Kettle AG, Coakley AJ, Knapp Jr FF. Pentavalent rhenium-188 dimercaptosuccinic acid for targeted radiotherapy: synthesis and preliminary animal and human studies. Eur J Nucl Med 1998;25:613–21. 124 eau-ebu update series 5 (2007) 113–125 [68] Palmedo H, Manka-Waluch A, Albers P, Schmidt-Wolf IG, Reinhardt M, Ezziddin S, et al. Repeated bone-targeted therapy for hormone-refractory prostate carcinoma: tandomized phase II trial with the new, high-energy radiopharmaceutical rhenium-188 hydroxyethylidenediphosphonate. J Clin Oncol 2003;21:2869–75. [69] Bayouth JE, Macey DJ, Kasi LP, Fossella FV. Dosimetry and toxicity of samarium-153-EDTMP administered for bone pain due to skeletal metastases. J Nucl Med 1994;35:63–9. [70] Turner JH, Claringbold PG, Hetherington EL, Sorby P, Martindale AA. A phase I study of samarium-153 ethylenediaminetetramethylene phosphonate therapy for disseminated skeletal metastases. J Clin Oncol 1989;7: 1926–31. [71] Collins C, Eary JF, Donaldson G, Vernon C, Bush NE, Petersdorf S, et al. Samarium-153-EDTMP in bone metastases of hormone refractory prostate carcinoma: a phase I/II trial. J Nucl Med 1993;34:1839–44. [72] Anderson PM, Wiseman GA, Dispenzieri A, Arndt CA, Hartmann LC, Smithson WA, et al. High-dose samarium-153 ethylene diamine tetramethylene phosphonate: low toxicity of skeletal irradiation in patients with osteosarcoma and bone metastases. J Clin Oncol 2002;20:189– 96. [73] Alberts AS, Smit BJ, Louw WK, van Rensburg AJ, van Beek A, Kritzinger V, et al. Dose response relationship and multiple dose efficacy and toxicity of samarium-153EDTMP in metastatic cancer to bone. Radiother Oncol 1997;43:175–9. [74] Sartor O. Overview of samarium sm 153 lexidronam in the treatment of painful metastatic bone disease. Rev Urol 2004;6(Suppl 10):S3–12. [75] Resche I, Chatal JF, Pecking A, Ell P, Duchesne G, Rubens R, et al. A dose-controlled study of 153Sm-ethylenediaminetetramethylenephosphonate (EDTMP) in the treatment of patients with painful bone metastases. Eur J Cancer 1997;33:1583–91. [76] Serafini AN, Houston SJ, Resche I, Quick DP, Grund FM, Ell PJ, et al. Palliation of pain associated with metastatic bone cancer using samarium-153 lexidronam: a double-blind placebo-controlled clinical trial. J Clin Oncol 1998;16:1574– 81. [77] Sartor O, Reid RH, Hoskin PJ, Quick DP, Ell PJ, Coleman RE, et al. Samarium-153-Lexidronam complex for treatment of painful bone metastases in hormone-refractory prostate cancer. Urology 2004;63:940–5. [78] Nabell L, Spencer S. Docetaxel with concurrent radiotherapy in head and neck cancer. Semin Oncol 2003;30:89–93. [79] Eapen L, Stewart D, Collins J, Peterson R. Effective bladder sparing therapy with intra-arterial cisplatin and radiotherapy for localized bladder cancer. J Urol 2004;172:1276– 80. [80] Aus G, Abbou CC, Bolla M, Heidenreich A, Schmid H-P, Van Poppel H, et al. EAU guidelines on prostate cancer. Eur Urol 2005;48:546–51. [81] Tu SM, Kim J, Pagliaro LC, Vakar-Lopez F, Wong FC, Wen S, et al. Therapy tolerance in selected patients with androgen-independent prostate cancer following strontium-89 combined with chemotherapy. J Clin Oncol 2005;23:7904– 10. [82] Akerley W, Butera J, Wehbe T, Noto R, Stein B, Safran H, et al. A multiinstitutional, concurrent chemoradiation trial of strontium-89, estramustine, and vinblastine for hormone refractory prostate carcinoma involving bone. Cancer 2002;94:1654–60. [83] Sciuto R, Festa A, Rea S, Pasqualoni R, Bergomi S, Petrilli G, et al. Effects of low-dose cisplatin on 89Sr therapy for painful bone metastases from prostate cancer: a randomized clinical trial. J Nucl Med 2002;43:79–86. [84] Mertens WC, Porter AT, Reid RH, Powe JE. Strontium-89 and low-dose infusion cisplatin for patients with hormone refractory prostate carcinoma metastatic to bone: a preliminary report. J Nucl Med 1992;33:1437–43. [85] Tu SM, Millikan RE, Mengistu B, Delpassand ES, Amato RJ, Pagliaro LC, et al. Bone-targeted therapy for advanced androgen-independent carcinoma of the prostate: a randomised phase II trial. Lancet 2001;357:336–41. [86] Widmark A, Modig H, Johansson M, Johansson E, Franzen L, Turesson I, et al. TAXSAM: a new chemo-radiation regimen for bone metastases in hormone refractory prostate cancer. Proceedings Prostate Cancer Symposium 2006;1:204. [87] Fizazi K, Beuzeboc P, Lumbroso J, Theodore C, Di Palma M, Prapotnich D, et al. A phase II trial of maintenance docetaxel and samarium in patients with castration-refractory bone metastases from prostate cancer with response or stabilization after induction docetaxel-estramustine: preliminary results. Proceedings Prostate Cancer Symposium 2006;1:205. [88] Tannock IF, de Wit R, Berry WR, Horti J, Pluzanska A, Chi KN, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med 2004;351:1502–12. [89] Yuen KK, Shelley M, Sze WM, Wilt T, Mason MD. Bisphosphonates for advanced prostate cancer. Cochrane Database Syst Rev 2006:CD006250. [90] Storto G, Klain M, Paone G, Liuzzi R, Molino L, Marinelli A, et al. Combined therapy of Sr-89 and zoledronic acid in patients with painful bone metastases. Bone 2006;39:35– 41. [91] Brenner W, Kampen WU, Kampen AM, Henze E. Skeletal uptake and soft-tissue retention of 186Re-HEDP and 153Sm-EDTMP in patients with metastatic bone disease. J Nucl Med 2001;42:230–6. eau-ebu update series 5 (2007) 113–125 CME questions Please visit www.eu-acme.org/europeanurology to answer these CME questions on-line. The CME credits will then be attributed automatically. 1. 125 B. a-particles are potentially less toxic to cells than b-particles. C. a-particles cannot be used for the treatment of prostate cancer. D. a-particles result in DNA double-strand breaks. 89 SrCl2 is a radionuclide for which one of the following applies: A. It does not have a natural ability to bind bone. B. Its physical half-life is <1 d. C. Its efficacy for pain relief is markedly shorter than other radionuclides. D. It has a natural ability to bind bone. 2. Physical half-lives differ between radionuclides. What is the correct order when ordered from short to long physical half-life? A. 89Sr; 186Re; 153Sm B. 153Sm; 186Re; 89Sr C. 186Re; 153Sm; 89Sr D. 188Re; 89Sr; 153Sm 3. The a-emitting radionuclides are relatively new in the field of palliation for bone pain from metastases. Which of the following is true: A. a-particles travel longer ranges in tissue compared to b-particles. 4. The most prevalent typical toxicity of all radionuclides is: A. Neuropathy B. Hepatotoxicity C. Nephrotoxicity D. Thrombocytopenia 5. Which of the following radionuclides is not dependent on a bisphosphonate for bone targeting? A. 153Sm B. 186Re C. 188Re D. 223Ra 6. Pain response to radionuclide treatment was shown to be associated with: A. Serum hemoglobin level B. Patient age C. Renal function D. Location of bone metastases