Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
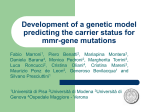
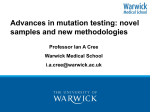
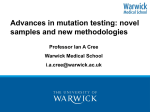
2400 Congenital Hypertrophy of the Retinal Pigment Epithelium in Familial Adenomatous Polyposis Novel Criteria of Assessment and Correlations with Constitutional Adenomatous Polyposis Coli Gene Mutations Rosa Valanzano, M.D.' Alessandro Cama, M.D? Roberto Volpe, M.D? Maria Cristina Curia, Ph.0.' Rita Mencucci, M.D? Raffaele Palmirotta, M.D? Pasquale Battista, Ph.o.2 Ferdinand0 Ficari, M.D.' Renato Mariani-Costantini, Francesco Tonelli, M.D.' M.D.' ' Dipartimento di Fisiopatologia Clinica, Unita' di Chirurgia, Universita' di Firenze, Firenze, Italy. Cattedra di Patologia Generale, lstituto di Patologia Umana e Medicina Sociale, Universita' "Gabriele D'Annunzio", Chieti, Italy. Clinica Oculistica I, Universita' di Firenze, Firenze, Italy. Preliminary data on congenital hypertrophy of retinal pigment epithelium have been published in: L'ipertrofia congenita dell'epitelio pigmentato della retina quale sensibile marker della poliposi familiare del colon. Chirurgia 1989: 2(9):472-6. Mutations of the adenomatous polyposis coli gene have been published as precised in the text and references. This work was supported by A.I.R.C. special project "I tumori ereditari del colon," by CNRACRO Grant 94.01 161.PF39, and by M.U.R.S.T. 40%. Address for reprints: Rosa Valanzano, M.D., Dipartimento di Fisiopatologia Clinica, Unita' di Chirurgia, Viale Morgagni, 85. 50134, Firenze, Italy. Received May 3,1996; revision received August 12, 1996; accepted August 12, 1996. 0 1996 American Cancer Society BACKGROUND. Congenital hypertrophy of the retinal pigment epithelium (CHRPE) is the most common extracolonic manifestation of familial adenomatous polyposis (FAP) and is an early clinical marker of the disease. It seems to be correlated with the position of constitutional mutations of the adenomatous polyposis coli (APC) gene. METHODS. The authors investigated the expression of CHRPE and its correlation with the position of the APC gene in FAP patients and in "at risk" relatives from 31 FAP kindreds. To obtain comparable data on CHRPE expression, the authors developed a novel scoring system based on morphologic and dimensional criteria. RESULTS. A positive CHRPE score was obtained in 29 of 39 FAP patients (74%) and in 16 of 53 relatives who showed no clinical evidence of FAP (30%). Colonoscopy revealed polyps in 20 of the 47 relatives who could be examined. The cumulative sensitivity and specificity of CHRPE were 72.88% and 96.29%, respectively. APC gene mutations were characterized in 34 subjects from 17 kindreds. In 28 of the subjects, mutations were detected in exon 15, between codons 876 and 1324. Mutations were found in exon 9 in 6 subjects. In 3 of the 6 subjects, they were found at the site where both forms of alternative splicing of the exon occur (codon 437). In the other 3 subjects (another kindred), mutations were found in the portion of exon 9 in which alternative splicing occurs (codon 367). Only 1 of the 6 subjects (16.6%) with mutations in exon 9 had a positive CHRPE score, compared with 28 of 28 subjects (100%) with mutations in exon 15. None of the 3 subjects with mutations in codon 437 had a positive CHRPE score. The CHRPE scores of exon 15 mutation carriers varied markedly both within and among kindreds, irrespective of the mutation site. CONCLUSIONS. The results of this study indicate that the site of APC gene mutation influences CHRPE expression but is not the only factor responsible for the presence and level of retinal lesions in FAP patients. Cancer 1996; 78:2400-10. 0 1996 American Cancer Society KEYWORDS: polyposis, familial adenomatous, hypertrophy, retinal pigment epithelium, congenital, adenomatous polyposis coli gene, mutations. F amilial adenomatous polyposis (FAP) is a dominant inherited disease characterized by the development of multiple colorectal adenomas that usually arises in the second decade of life. However, age at disease onset and the number and distribution of polyps vary among patients, even within the same family.'-3 Phenotypic variability is also evident for the extracolonic lesions associated with FAF', which include epidermoid cysts, osteomas, dental abnormalities, desmoid tumors, and congenital hypertrophy of the retinal pigment epithelium (CHRPE).CHRPE, which Retinal Lesions and APC MutationsNalanzano et al. occurs in up to 60% of patient^,^-^ is the most frequent extracolonic manifestation of the disease and is widely used a!; an early clinical marker. However, the sensitivity of CHRPE analysis varies in the literature, probably due to differences in the criteria utilized to define a positive ophthalmic exarninati~n.’~~ FAP is caused by germline mutations of the adenomatous polyposis coli (APC) gene.’-’* The APC gene is comprised of at least 15 coding exons and several noncoding exons, which can be expressed in various combinations by alternative s p l i ~ i n g . ~ The ~ ’ ~ ~APC ’~ gene product is a cytoplasmic protein of large size that contains 2843 amino acids in its most common form.”” APC proteins can associate to form homodimers i3nd interact with other cytoplasmic proteins, including microtubules and p-catenin. Microtubules bind 1 he carboxy-terminal region, typically deleted in mutant proteins, whereas p-catenin, which is necessary for the function of the cell adhesion protein Ecadherin,“ interacts with the region of exon 15 downstream of codon 1014.’6”7The vast majority of the APC mutations thus far reported in FAP patients result in premature termination of protein synthesis.I8 There are correlations between position of the APC mutation and phenotypic manifestations of FAP. Mutations near the 5’ end of the gene are associated with an attenuated form of the disease, characterized by a reduced number of colorectal polyps.’ Mutations downstream of exon 9 appear to cause the classic form of FA.P associated with CHRPE.19,20 The APC gene was analyzed in 47 FAP patients and in 14 “at risk” relatives from 26 kindreds. The analysis was conducted using a combination of screening techniques. These included single strand conformation polymorphism (SSCP) analysis of the coding region from exon 1 through exon 15, heteroduplex analysis coupled with multiple allele specific polymerase chain reaction (PCR) for the identification of 3 common mutations in exon 15,” and the in vitro synthesized protein assay (IVSP) for the detection of truncating mutations of exon 15.18,21-23 The 61 subjects who were analyzed at the molecular level are part of a larger group of 39 FAP patients and 53 relatives from 31 kindreds subjected to ophthalmoscopic studies using novel criteria designed to allow a standardized assessment of CHRPE positivity. The purpose of this article was to describe and evaluate the results of CHRPE studies in the light of data derived from molecular analyses, colonoscopy, and standardized criteria for the evaluation of ocular lesions. PATIENTS AND METHODS Patients Starting in 1988, 39 affected patients (group I) and 53 relatives at 50% genetic risk of FAP (group II), belong- 2401 ing to 31 kindreds, were evaluated for the presence of CHRPE by the same ophthalmologist. The individuals studied included 53 males and 39 females. The mean age of Group I subjects was 32.2 years 2 13.9 standard deviation (SD) (range, 8-62 years); the mean age of Group I1 subjects was 23.3 years 5 10 SD (range, 245 years). All Group I1 subjects aged older than 10 years (47 of 53) were also screened by colonoscopy. Molecular genetic analysis of the APC gene was performed on 61 subjects from 26 kindreds (Group I: 47 subjects; Group 11: 14 subjects). Ophthalmoscopic Examination CHRPE screening All individuals received a dilated fundus examination, including direct and indirect ophthalmoscopy and biomicroscopy with a Goldman lens. All cooperating subjects were submitted to wide angle fundus photography, using a Canon 60” Fundus Camera (Japan).The entire retina was photographically documented with extensive overlapping peripheral photographs. Each CHRPE lesion was evaluated with regard to size, location, and degree of pigmentation. All subjects younger than 10 years of age were followed for a minimum of 3 years, to evaluate a possible new appearance or progression of the lesions. Diagnostic criteria CHRPE lesions were classified in 3 morphologic classes: 1) very small (< 100 pm in greatest dimension), hyperpigmented areas (“spot lesions”) with well defined margins and no halo, localized in the midperiphery (Fig. la); 2) round, depigmented, or hyperpigmented areas ( < I disk in greatest dimension), generally located in the midperiphery (Fig. Ib); and 3) areas located at the posterior pole or along the main vascular arcades, with two different aspects: typical hyperpigmented or hypopigmented, oval areas surrounded by a depigmented halo (“leaf-like” lesions) (Fig. lc); or large (>1 disk in greatest dimension), round, variably pigmented areas with regular or scalloped margins (Fig. Id). For scoring purposes, each CHRPE lesion was assigned a value ranging from 1 to 3, according to the class (class 1: score 1; class 2: score 2: class 3: score 3). The individual CHRPE score was calculated by adding the relative values determined for each eye. Fundoscopy was considered positive when the individual CHRPE score was 23. Using this cutoff level, lesions of the type observable in normal subjects were considered of significance only if m ~ l t i p l e . ~ Identification of APC Mutation One propositus from each FAP kindred was initially subjected to molecular analysis to identify mutations 2402 CANCER December 1,1996 / Volume 78 / Number 11 FIGURE 1. Examples of congenital hypertrophy of the retinal pigment epithelium (CHRPE) lesions. (a) Small (< 100 p m in greatest dimension), hyperpigmented area of CHRPE with well defined margins, localized in the periphery (“spot” lesion), score = 1. (b) Oval, irregularly pigmented lesion with greatest dimension < 1 optic disk, localized just below the main vascular archade, score = 2. (c) Typical, oval pigmented lesion surrounded by a depigmented halo (“leaf-like” lesion), score = 3. (d) Two large (>1 optic disk in greatest dimension), round, irregularly pigmented lesions with regular margins, score = 3 (for each lesion). in the APC gene. In the kindreds in which mutations were detected, mutational analysis was extended to “at risk” relatives. The screening of APC mutations was performed by three independent methods. The first method was designed to identify three frequently occurring deletions of the APC gene at codons 1061, 1068, and 1309, and was comprised of heteroduplex analysis on agarose minigel (HAAM), coupled with allele specific multiple PCR. This diagnostic strategy was previously described in detail.” The second method Retinal Lesions and APC MutationsNalanzano et al. 2403 FIGURE 1. (continued) was comprised of SSCP analysis followed by PCR direct sequencing. The coding sequence of the APC gene, spanning exons 1 through 15, was amplified by PCR and subjected to SSCP as des~ribed."-'~The nucleotide sequence of amplified genomic DNA was directly determined using 35SdATP as the label.'4 The third method was comprised of IVSP, as described by Powell et a1." Because RNA samples from FAP patients were not available, the latter analysis was limited to exon 15, which contains approximately 60% of the coding sequence of the APC gene. Genetic analyses, either positive or negative for the presence of APC mutations, were always repeated using samples deriving from new DNA extractions. Duplicate experiments confirmed the results. Statistical Analysis Ophthalmoscopic data were analysed by the chisquare test. Confidence limits were calculated to estimate the possible range for sensitivity, specificity, and predictive values. The Mann-Witney U test was used to analyze correlations between CHRPE scores and positions of the mutations. CANCER December 1, 1996 / Volume 78 / Number 11 2404 15 b 12 w w u m n 0 0 9 e w n no n r n 6 u o n &;3 e5 - ... .-.. -.-...-A. ..- ! l ..- .....-. 0 An[ n a 2 EL U 4 13 12 e Kindred: GD’ f UE -- h m i n Kindred: L# * Kindreds with known APC mutation #Kindreds with undetermined APC mutation FIGURE 2. Distribution of congenital hypertrophy of the retinal pigment epithelium (CHRPE) scores in Group I (A)and Group I1 (0) of patients. Subjects of the same kindred are vertically arranged. The number of subjects with the same CHRPE score is shown inside the symbols. RESULTS CHRPE Analysis Examples of the application of the authors’ scoring method to the evaluation of CHRPE lesions are shown in Figure 1. Twenty-nine of 39 Group I subjects (74%) from 29 families and 16 of 53 Group I1 subjects (30%) from 22 families had a CHRPE score 2 3. Three young subjects of Group 11, aged 2, 8, and 9 years, respectively, had only 1 or 2 “spot” lesions each at the first eye examination and were considered negative for CHRPE. A second fundoscopy was performed at 5, 13, and 14 years, respectively. The first subject showed 3 typical “leaf-like’’lesions, 1 “spot,” and 1 Class 2 lesion (total score = 12); the second subject showed 1 “leaf-like’’lesion, 6 “spots,” and 1 Class 2 lesion (total score = 11); the last subject exhibited 5 “spot” lesions (total score = 5). Figure 2 illustrates the distribution of the CHRPE scores in both group of patients, within and among the 31 families examined, and shows the extreme variability in CHRPE expression (scores between 0 and 16). Colonoscopy revealed polyps in 20 of 47 Group I1 TABLE 1 CHRPE Status and Results of Colonoscopy in 47 Group I1 Subjects ~~ Polyps CHRPE positive (no.of subjects) CHRPE negative (no. of subjects) Present 15 5 Absent 1 26 CHRPE coneenital hwertroohv of the retinal oiament eoithelium subjects examined (42%). Fifteen of these 20 subjects were positive for CHRPE, with a mean score of 8.4 ? 4 SD (range, 3-15). Five Group I1 subjects negative for CHRPE were positive for polyps at colonoscopy (Table 1). Only one of the 27 Group I1 subjects who was negative at colonoscopy was positive for CHRPE. This subject exhibited a depigmented area < 1 disk greatest dimension in the right eye and a “spot” lesion in the left eye and thus had a CHRPE score of 3. Ten of 39 FAP Croup I subjects were negative for CHRPE. The distribution of the CHRPE scores in the 59 subjects Retinal lesions and APC MutationsNalanzano et at. 2405 18 O+* 15 w 0 r.c AA V I ++ 12 V 0 ++ W Q #W Co fY I 9 . . 0 O W * 1 O* 6 O * W m U *+*+++ 0000 * 00000 H H H-IH-t- Subjects with colorectal polyps (group I + group 11) Subjects without colorectal Polyps (group 11) Distribution of the congenital hypertrophy of the retinal pigment epithelium (CHRPE) scores in subjects positive ( + : Group I; 0 : Group !I) and negative (U) for colorectal polyps at colonoscopy. with colorectal polyps (39 in Group I and 20 in Group 11) and in the 27 Group I1 subjects negative for polyps is shown in Figure 3. The difference in CHRPE positivity between subjects negative and positive for polyps is significan.t ( P < 0.001) (Fig. 3 ) . The cumulative sensitivity of CHRPE was 72.88% (95% confidence limits [CL],59.73-83.63%; P < 0.05) and the specificity was 96.29% (95% CL, 81.02-99.90%; P < 0.05). The positive and negative predictive values were 97.72% (95% CL, 87.97-99.94%; P < 0.05) and 61.90% (95%CL, 45.63-76.42%; P < 0.051, respectively. Molecular Analysis of the APC Gene Germline mutations of the APC gene were identified in 17 unrelated FAP kindreds using 3 independent screening methods (Table 2). A total of 34 carriers of germline APC mutations were identified in the 17 kindreds (Fig. 4). The frequently occurring deletions of the APC gene at codons 1061, 1068, and 1309 were identified in 9 pedigrees (GD-3, GD-4, GD-5, GD-6, GD-7, GD-8, GD-9, GD-10, and GD-11) using HAAM coupled with allele specific multiplex PCR." In 6 additional kindreds (GD-1, GD-2, GD-12, GD-13, GD-15, and GD-17), mutations were detected using SSCP coupled with direct s e q u e n ~ i n g . ~Finally, ~ ~ ' ~ , ~in~ 2 kindreds (GD-18 and GD-19), in which SSCP analysis failed to detect the germline mutations, IVSP revealed the presence of truncated APC alleles that were further characterized by sequence analysis (Table 2). Mutations at codons 367,876,995,1112,and 1075 are novel 2406 CANCER December 1, 1996 / Volume 78 / Number 11 TABLE 2 Summary of Germline Adenomatous Polyposis Coli Gene Mutations Detected in 17 Familial Adenomatous Polyposis Kindreds Kindred Type of mutation Codon Exon GD- 1 GD-2 GD-3, GD-5, GD-6, GD-7, GD-10, GD- 1I GD-4 GD-8, GD-9 GD-12 GD-13 GD-15 GD-17 GD-18 GD-19 1 bp deletion 3 bp deletion 1324a 437“ 15 9a (donor site) 5 bp deletion 4 bp deletion 5 bp deletion 1 bp deletion Tyr-Stop Arg-Stop 2 bp deletion Arg-tStop Cys-tStop 130ga 106V 1061a 1112 1075a 1114 367 876 995 15 15 15 15 15 15 9 15 15 bp: base pair. aPpreviouslvoublished in references 21-23 and 25. in patients with mutations in exon 15 than in patients with mutations in exon 9 (Mann-Witney U test; P < 0.01) (Fig. 5). No differences in CHRPE scores were apparent in carriers of mutations in exon 15 occurring upstream or downstream of codon 1014 (2 and 26 subjects, respectively). The 2 patients with mutations before codon 1014 had a CHRPE score of 6 and 9, respectively; the mean CHRPE score of the patients with mutations after codon 1014 was 8.15 5 3.8 SD (range 3-16). FAP carrier status was ruled out in only 1 of the 16 Group I1 “at risk” subjects with positive CHRPE scores. This was a 38-year-old individual (GD 1-12) who had a depigmented area in the right eye and a spot lesion in the other eye, with a consequent CHRPE score of 3, which corresponds to the cutoff level established in this study. Subject GD 1-12 tested negative for the APC mutation responsible for the disease in his kindred and was negative for polyps at colonoscopy. DISCUSSION germline variants of the APC gene. The deletion of two base pairs at codon 367 is located in the portion of exon 9 that undergoes alternative splicing and is expected to be present only in a fraction of transcripts from the allele bearing this deletion (manuscript in preparation). All mutations are predicted to result in truncated APC proteins. CHRPE Score and Position of APC Mutations Mutations in exon 9 occurred at the site used in both forms of alternative splicing of the exon (codon 437) in one kindred (3 patients), and in the portion of exon 9 that undergoes alternative splicing (codon 367) in the other kindred (3 patients). None of the patients with the mutation in the alternatively spliced region had a positive CHRPE score. Only 1 of the 3 patients with mutations at codon 437 (GD 2-71) was positive for CHRPE (score = 6).All carriers of mutations in exon 15 were positive for CHRPE; however, the individual CHRPE scores varied both among and within the 15 kindreds examined, irrespective of the mutation site (Fig. 4). In particular, the CHRPE score varied from 3 (determined in 3 patients with mutations at codons 1112, 1114, and 1309, respectively) to 16 (determined in 2 patients, from 2 different families, with mutations at codon 1309). The same variability (CHRPE score: range 3-16) was also observed in the group of 12 patients from 6 kindreds with mutations at codon 1309 and in patients belonging to a single kindred (GD-3) bearing the 5 base pair deletion at codon 1309. Intrafamilial variability was also significant in patients with mutations at codon 1324 (from kindred GD1) (Fig. 4). The mean CHRPE score was significantly higher Not infrequently, otherwise normal individuals may have one or two areas of CHRPE, usually appearing as small (<O. 1 disk greatest dimension), unilateral, hyperpigmented lesion^.^^".^ In normal subjects, such lesions are usually < 4 and are rarely bilateral?’ There is no agreement on the number and the type of CHRPE lesions meeting clinical significance. Usually, only the presence of multiple areas of CHRPE, upward from a minimum varying from 2 to 4, is considered indicative of FAP.z7-z9In FAP patients, it has been shown that small, round, pigmented dots are significantly correlated in number with age,6but there is no evidence of any variation with age for the typical large oval pigmented lesion^.^ In this study, an increase in the number of “spot” areas and the appearance of new, large and typical lesions was observed in three young subjects who exhibited only one or two small pigmented “spot” areas of CHRPE at their first ophthalmic examination. The possibility that the first eye examination was unreliable due to the young age of the subjects appears unlikely, at least for two subjects whose entire retina was photographically documented. However, ophthalmology may not detect all lesions, because Traboulsi et al. identified 70 areas of CHRPE at autopsy in the eyes of a FAP patient with only 24 lesions previously described at f ~ n d o s c o p yTherefore, .~~ the authors could suspect the growth of already present lesions still not detectable by direct ophthalmology. The presence of multiple areas of CHRPE (regardless of size) in some controls and in many subjects with hereditary nonpolyposis colorectal carcinomazg indicates that the number of lesions per se is not always a reliable sign of FAP. Therefore, in several stud- Retinal Lesions and APC MutationsNalanzano et al. 2407 FIGURE 4. Correlation of individual congenital hypertrophy of the retinal pigment epithelium (CHRPE) scores with the site of the adenomatous polyposis coli gene mutation (codon) in 35 familial adenomatous polyposis patients from 17 kindreds (GD-1 through 13, GD-15, GD-17, GD-18, and GD-19). The order of presentation of individual patients follows the number of the codon site of the mutation. 18 - 2 0 15- cn W o, e '12 -- r 0 9- 6- 8% 3 - 5" 0- A I I ies, morphologic or dimensional criteria were combined with the number of lesions in the attempt to define clinically reliable methods for the assessment of positive ophthalmic examinations. According to Morton et al., at least 2 of the following 3 criteria should be met: 1) the presence of bilateral lesions; 2) I I the presence 2 3 lesions; and the 3 ) presence of any lesion > 0.3 optic disk in greatest dimension." Other authors propose that only oval pigmented areas with a surrounding depigmented halo should be considered pathognomonic of FAP and therefore diagnostically reliable per se.4331The authors attributed a score of 3 2408 CANCER December 1,1996 I Volume 78 / Number 11 at the cutoff level to each lesion of this type and to each variably pigmented lesion > 1 disk greatest dimension, a score of 2 to each variably pigmented lesion < 1 disk greatest dimension, and a score of 1 to each small, pigmented “spot” lesion. Therefore, lesions of the type observable in control subjects were considered significant only if m ~ l t i p l eThe . ~ only falsepositive subject detected in this study presented with a depigmented area and a “spot” lesion with a CHRPE score of 3, at the borderline. Depigmented areas are not infrequently observed in FAP patients whereas they are very rare in subjects at low risk of FAP,4so that it was reasonable to consider this subject positive for CHRPE. However, it is also reported that both depigmented and “spot” lesions are of limited diagnostic value when not associated with other types of CHRPE.4,32Moreover, a misleading phenotype with borderline CHRPE has been described.33 Otherwise, the current scoring method allowed a high specificity, comparable to that reported by Traboulsi et al. who consider only the presence of multiple lesions (> four) and/or bilateral lesions to be significant.**The sensitivity was also in agreement with that reported for other method^^-^ and even with that of authors who consider the presence of any lesion significant.’ Moreover, the scoring system allows an immediate comprehension of the patient’s CHRPE status (positive, negative, or borderline) and makes the description of number and type of lesions unnecessary, replaced by numbers. Thus, although scores within the lower range of positivity may not always indicate a FAP carrier status, the authors believe their scoring system is an easy and effective method for the uniform and comparable evaluation of CHRPE status in FAP patients and in their “at risk” relatives. Recent studies indicate that there are correlations between position of the APC mutation and the presence of CHRPE. In particular, it has been reported that CHRPE is associated with mutations located downstream of exon 9.19,20The region of exon 9 corresponding to the boundary between CHRPE positive and CHRPE negative mutations has not been clearly defined. Caspari et al. reported the presence of CHRPE in approximately 50% of FAP patients with mutations at codons 413 and 438 in exon 9.34Furthermore, it has been recently observed that patients with mutations beyond codon 1444 have a high prevalence of desmoid tumors but lack ophthalmic lesions.34This suggests that APC mutations introducing stop signals between exon 9 and codon 1444 of exon 15 result in the expression of protein products that interfere with the proliferative control of retinal pigment epithelium. Such interference might be related to a dominant-negative effect of the truncated proteins, leading to the inacti- vation of other proteins binding to the APC gene prodUCt,17,35 or to a reduced stability of APC proteins expressed by alleles carrying mutations in the 5’ region of the gene.3” The APC mutations detected in the patients analyzed in this study were comprised within the region of the gene ranging from codon 367 in exon 9 to codon 1324 in exon 15. The finding of mutations in this region of the gene might in part be related to the technical approach. The coding region of the APC gene from exon 1 through exon 15was screened by SSCP analysis. However, because of the unavailability of RNA Samples, only exon 15, which comprises approximately 60% of the coding region of the APC gene, could be analyzed by IVSP. In this region, IVSP detected two mutations that had escaped detection by SSCP. Therefore, it is possible that some patients with undetermined APC mutations characterized for CHRPE lesions have mutations in the region of the APC protein encoded by exons 1-14. Alternatively, there may have been large deletions of the coding region of the gene that escaped detection by SSCP. The current study confirms that patients with mutations in exon 9 tend to have attenuated CHRPE expression. In fact, only 1 of the six patients with mutations in exon 9 presented with a CHRPE score above the cutoff level. Interestingly, this patient had a mutation that was expected to completely abolish the correct splicing of exon 9. In contrast, the 3 patients with mutations in the portion of exon 9 that undergoes alternative splicing had a CHRPE score < 3. All the patients with APC mutations in exon 15 (between codons 876 and 1324) had CHRPE scores 2 than 3. This notwithstanding, there was extreme variability in the CHRPE scores associated with mutations in exon 15, irrespective of the position of the mutation. Even patients from the same kindred showed significant differences in CHRPE scores (Fig. 4). As reported in other ~ t u d i e s , ~ , the * ~ ,5~ ’ base pair deletion at codon 1309, known to be associated with severe colorectal disease, accounted for the highest number of FAP patients. It is particularly intriguing that the CHRPE scores associated with this deletion exhibited the highest range of variability documented in the current study, even within the same kindred. As reported by Wallis et al.,” no differences in CHRPE expression were found in carriers of mutations expected to determine the deletion or preservation of the catenin-binding In conclusion, the current study observations suggest that the site of mutation in the APC gene is not the only factor responsible for the variable expression of CHRPE in FAP patients. Nevertheless, because ophthalmologic examination is a direct, noninvasive, and inexpensive test, Retinal Lesions and APC MutationsNalanzano et al. CHRPE maintains its role in FAP screening, especially in families with known AFT mutation. Moreover, in newly diagnosed FAP kindreds, CHRPE expression could direct the mutation analysis on specific regions of the APC gene. REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10 11. 12. 13 14. 15. Spirio L, Olschwang S, Groden J, Robertson M, Samowitz W, Joslyn G, et al. Alleles of the APC gene:an attenuated form of familial polyposis. Cell 1993;75:951-7. Giardiello FM, Krush AJ, Petersen GM, Booker SV, Kerr M, Tong LL, et al. Phenotypic variability of familial adenomatous polyposis in 11 unrelated families with identical APC gene mutation. Gastroenterology 1994;106:1542-7. Nagase H, Miyoshi Y, Horii A, Aoki T, Ogawa M, Utsunomiya J, et al. Correlation between the location of germ-line mutations in the APC gene and the number of colorectal polyps in familial adenomatous polyposis patients. Cancer Res 1992;5214055-7. Hodgson SV, Bishop DT, Jay B. Genetic heterogeneity of congenital hypertrophy of the retinal pigment epithelium (CHRPE) in families with familial adenomatous polyposis. J Med Genet 1994;31:55-8. Msther ER, Barton DE, Slatter R, Koch DJ, Jones MH, Nagase H, et al. Evaluation of molecular genetic diagnosis in the management of familial adenomatous po1yposis:a population based study. J Med Genet 1993;30:675-8. Morton DG, Gibson J, MacDonald F, Brown R, Haydon 7, Cullen R, et a]. Role of congenital hypertrophy of the retinal pigment epithelium in the predictive diagnosis of familial adenomatous polyposis. Br J Surg 1992;79:689-93. Bapat BV, Parker JA, Berk T, Cohen Z, McLeod RS, Ray PN, et al. Combined use of molecular and biomarkers for presymptomatic carrier risk assessment in familial adenomatous po1yposis:implications for screening guidelines. Dis Colon Rectum 1994;37:165-71. Heyen F, lagelman DG, Romania A, Zastov N, Lavery IC, Fazio VW, et al. Predictive value of congenital hypertrophy of retinal pigment epithelium as a clinical marker for familial adenomatous polyposis. Dis Colon Rectum 1990;33:1003-8. Gioden J , Thliveris A, Samowitz W, Carlson M, Gelbert L, Albertsen H, et al. Identification and characterization of the familial adenomatous polyposis coli gene. Cell 1991;66:589600. Joslyn G, Carlson M, Thliveris A, Albertsen H, Gelbert L, Samowitz W, et al. Identification of deletion mutations and three new genes at the familial polyposis locus. Cell 1991;66:601-13. Kinzler KW, Nilbert MC, Su LK, Vogelstein B, Bryan TM, Levy DB, et a]. Identification of FAP locus genes from chromosome 5q21. Science 1991;253:661-5. Nishisho I, Nakamura Y, Myoshi Y, Miki Y, Ando H, Horii A, et al. Mutations of chromosome 5q21 genes in FAP and colorectal cancer patients. Science 1991;253:665-9. Oshima M, Sugiyama H, Kitagawa K, Taketo M. APC gene messanger RNA:novel isoforms that lack exon 7. Cancer Res 1993;53:5589-91. Thliveris A, Samowitz W, Matsunami N, Groden J, White R. Demonstration of promoter activity and alternative splicing in the region 5’ to exon 1 of the APC gene. Cancer Res 1’394;54:2991-5. Olzawa M, Rinwald M, Kemler R. Uvomorulin-catenin complex formation is regulated by a specific domain in the cyto- 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 2409 plasmic region of the cell adhesion molecule. Proc Natl Acad Sci USA 1990;87:4246-50. Rubinfeld B, Souza B, Albert I, Muller 0, Chamberlain SM, Masiarz FR, et al. Association of the APC gene product with beta-catenin. Science 1993;262:1731-4. Su LK, Vogelstein B, Kinzler KW. Association of the APC tumor suppressor protein with catenins. Science 1993; 262:1734-7. Powell SM, Petersen G, Krush AJ, Booker S, Jen J, Giardiello FM, et al. Molecular diagnosis of familial polyposis. N Engl J Med 1993;359:235-7. Olschwang S, Tiret A, Laurent-Puig P, Muleris M, Parc R, Thomas G. Restriction of ocular fundus lesions to a specific subgroup of APC mutations in adenomatous polyposis coli patients. Cell 1993;75:959-68. Wallis YL, Macdonald F, H u l t h M, Morton JEV, McKeown CM, Neoptolemos JP, et al. Genotype-phenotype correlation between position of constitutional APC gene mutation and CHRPE expression in familial adenomatous polyposis. Hum Genet 1994;94:543- 8. Cama A, Palmirotta R, Curia MC, Esposito DL, Ranieri A, Ficari F, et al. Multiplex PCR analysis and genotype-phenotype correlations of frequent APC mutations. Hum Mutat 1995;5: 144-52. Cama A, Esposito DL, Palmirotta R, Curia MC, Ranieri A, Ficari F, et al. A novel deletion in exon 15 of the APC gene in an Italian FAP kindred. Hum Mutat 1994;3:301-4. Cama A, Esposito D, Palmirotta R, Curia MC, Ranieri A, Ficari F, et al. A novel mutation at the splice junction of exon 9 of the APC gene in familial adenomatous polyposis. Hum Mutat 1995;3:305-8. Cama A, Sierra ML, Quon MJ, Ottini L, Gorden P, Taylor SI. Substitution of glutamic acid for alanine 1135 in the putative catalytic loop of the tyrosine kinase domain of the insulin receptor. A mutation that impairs proteolytic processing into subunits and inhibits receptor tyrosine kinase activity. J Biol Chem 1993;208:8060-9. Palmirotta R, Curia MC, Esposito D, Valanzano R, Messerini L, Ficari F, et al. A novel mutation and inactivation of both alleles of the APC gene in desmoid tumors. Hum Ma1 Genet 1995;4:1979-81. Burn J, Chapman P, Delhanty J, Wood C, Lalloo F, CachonGonzalez MB, et al. The UK Northern Region genetics register for familial adenomatous polyposis co1i:use of age at onset, congenital hypertrophy of the retinal pigment epithelium and DNA markers in risk assessment. J Med Genet 1991;28289-96. Chapman PD, Church W, Burn J, Gunn A. Congenital hypertrophy of the retinal pigment epithe1ium:a sign of familial adenomatous polyposis. Br Med J 1989;298:34-5. Traboulsi EI, Krush AJ, Gardner El, Booker SV, Offerhaus GJ, Yardley JH, et al. Prevalence and importance of pigmented ocular fundus lesions in Gardner’s syndrome. N EnglJ Med 1987;316561-7. Hunt LM, Robinson MHE, Hugkulstone CE, Clarke B, Vernon SA, Gregson RHS, et al. Congenital hypertrophy of the retinal pigment epithelium and mandibular osteomata as markers in familial colorectal cancer. Br JSurg 1994;70:1736. Traboulsi EI, Murphy SF, de la Cruz ZC, Maumenee IH, Green WR. A clinicopathologic study of the eyes in familial adenomatous polyposis with extracolonic manifestations (Gardner’s syndrome). Am J OphthalmoZ1990; 110:550-61. 2410 CANCER December 1, 1996 / Volume 78 / Number 11 31. Polkinhorne PJ, Ritchie S, Neale K, Schoeppner G, Thomson JPS, Jay BS. Pigmented lesions of the retinal pigment epithelium and familial adenomatous polyposis. Eye 1990;421621. 32. Berk T, Cohen Z, McLeod RS, Parker JA. Congenital hypertrophy of the retinal pigment epithelium as a marker for familial adenomatous polyposis. Dis Colon Rectum 1988; 31:253-7. 33. Caspari R, Friedl W, Propping P. Misleading phenotype in kindreds with familial adenomatous polyposis. Lancet 1992;339:1064. 34. Caspari R, Olschwang S, Friedl W, Mandl M, Boisson C, Boker T, et al. Familial adenomatous po1yposis:desmoid tu- mours and lack of ophthalmic lesions (CHRPE) associated with APC mutations beyond codon 1444. Hum Mol Genet 1995;4:337-40. 35. Su LK, Johnson KA, Smith KJ, Hill DE, Vogelstein B, Kinzler KW. Association between wild type and mutant APC gene products. Cancer Res 1993;53:2728-31. 36. Smith KJ, Johnson KA, Bryan TM, Hill DE, Markowitz S, Willson JK, et al. The APC gene product in normal and tumor cells. Proc Nut1 Acad Sci USA 1993;90:2846-50, 37. Paul P, Letteboer T, Gelbert L, Groden J, White R, Coppes MJ. Identical APC exon 15 mutations result in a variable phenotype in familial adenomatous polyposis. Hum MoZ Genet 1993;2:925-31.